Iatrogenic perforations represent one of the most biologically challenging complications encountered in endodontic practice, particularly when they occur at the pulpal floor of molar teeth. These defects compromise the structural and biological integrity of the root canal system, establishing a direct pathway for microbial ingress into the periodontal tissues and significantly influencing prognosis if not managed appropriately.
Contemporary endodontics has evolved from traditional, often aggressive approaches to a more conservative, biologically driven philosophy that emphasises preservation of tooth structure and optimisation of healing. Within this context, minimally invasive repair strategies—supported by advanced biomaterials and enhanced visualisation—have redefined the management of such complications.
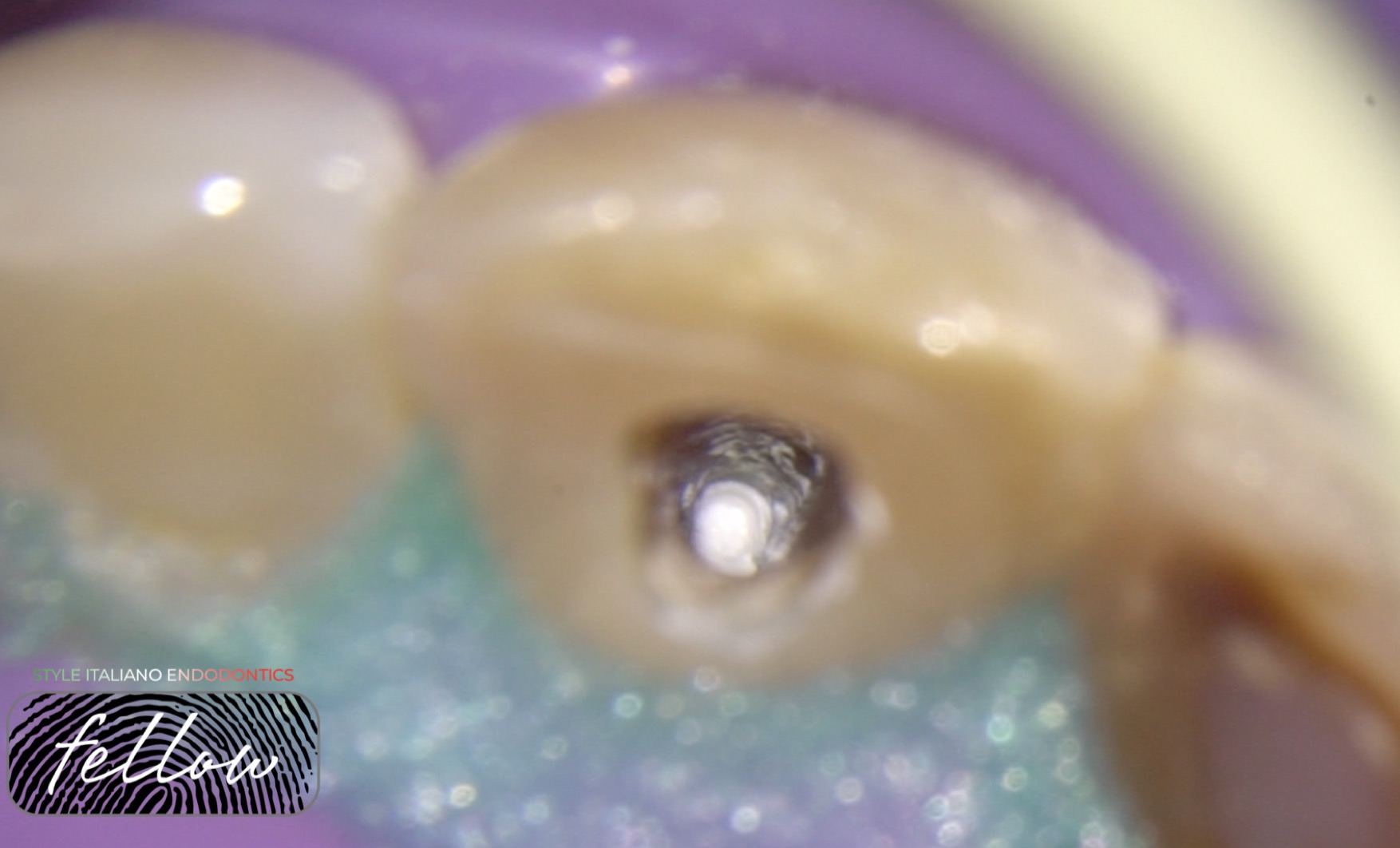
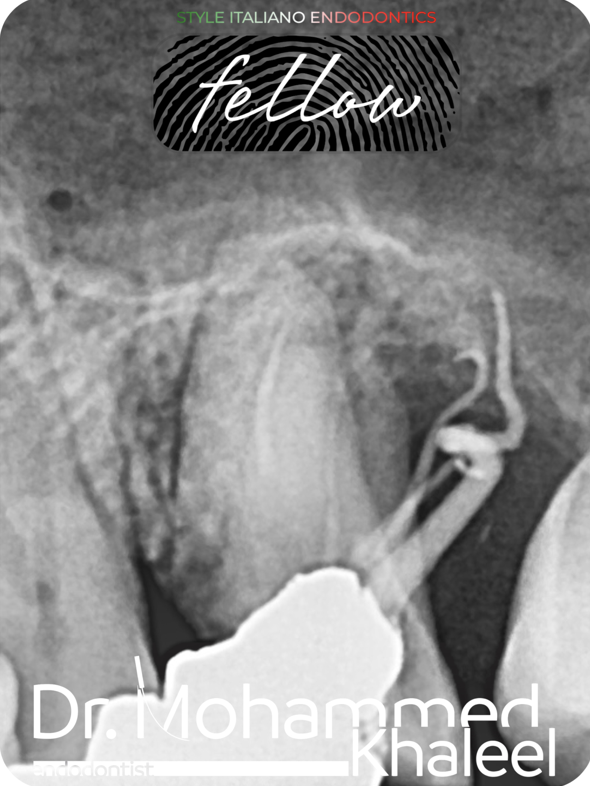
This chapter presents a detailed clinical narrative of a referred mandibular first molar (tooth 36) exhibiting a pulpal floor perforation, managed using mineral trioxide aggregate (MTA) delivered with precision through the appropriate system. Emphasis is placed on the role of magnification, controlled material placement, and adherence to the principles of corrective root canal therapy. The clinical workflow, biological rationale, and key procedural considerations are explored in depth, supported by current evidence and contemporary clinical insights.