Endodontic management of immature central incisor by apexification
16/12/2023
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Trauma or caries in young children or adolescents can cause pulp necrosis, which may arrest root development in permanent teeth. This in turn results in thin dentinal walls, wide-open apices or sometimes divergent configuration or reverse anatomy, and inadequate crown-root ratio.
Treatment of necrosed permanent teeth with immature apices mainly revolves around Apexification and Regenerative endodontic therapy (RET).
Apexification is a method to encourage the development of an apical barrier to close the open apex of an immature necrotic permanent tooth in which filling materials can be placed within the root canal space. Apexification is done in the tooth which has nearly completed root formation with an open apex.
RET is a biologically based procedure designed to replace damaged structures, such as the root and dentin, along with cells of the pulp–dentin complex.
RET is recommended when the root development is severely deficient (less than two-thirds according Cvek’s classification) with thin canal walls, a wide-open apex and where the tooth’s prognosis is hopeless even with an apexification procedure.
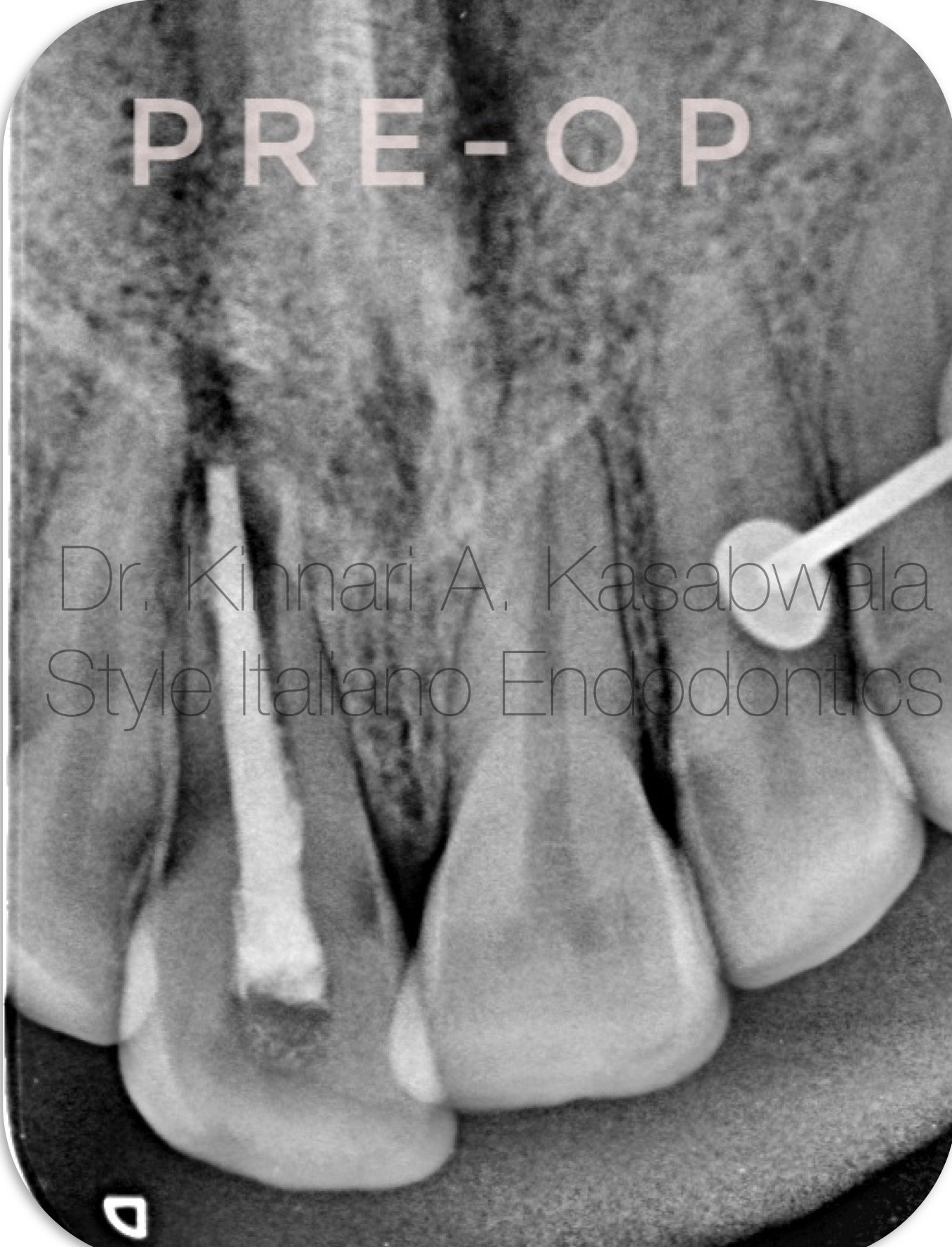
Fig. 1
12 year old patient reported with H/O recurrent pain and pus discharge from upper front tooth region.
H/O trauma 4 years ago.
H/O RCT 6 months ago.
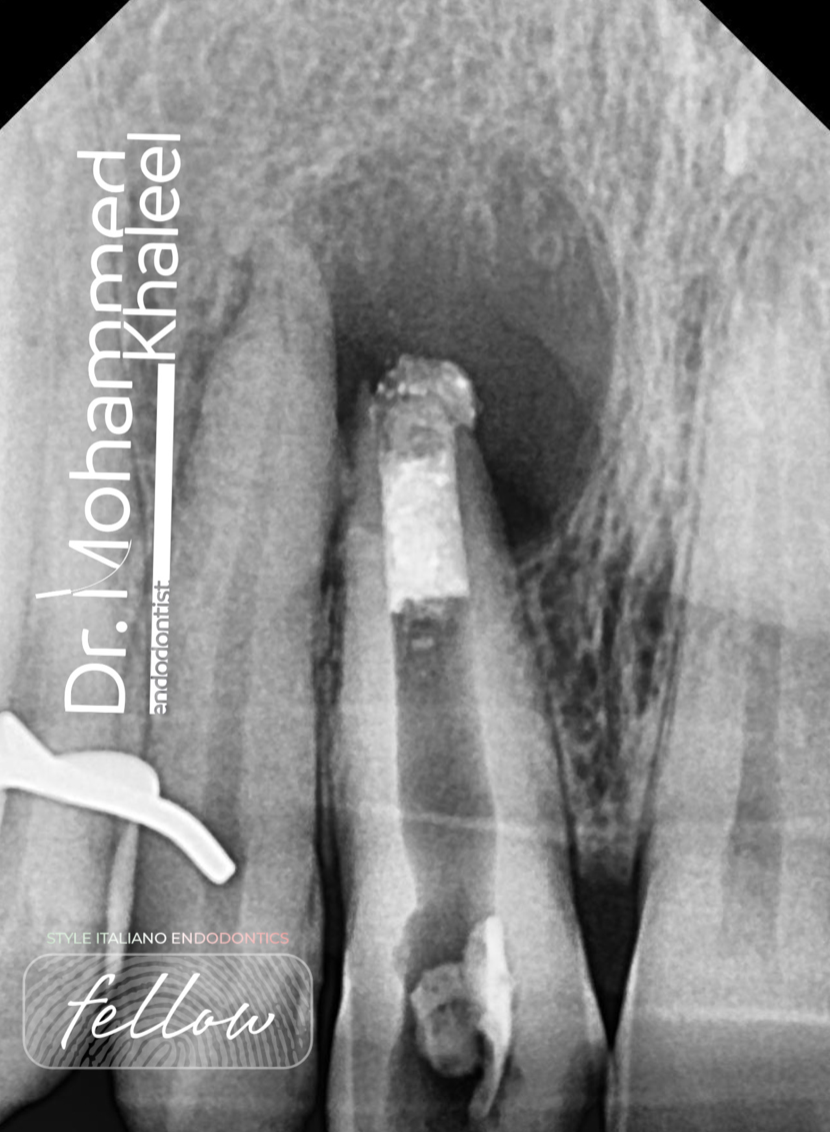
IOPA shows blunderbuss canal (reverse apical anatomy) in 11 with conventional RCT done using gutta percha points and deficient apical seal and periapical lesion.
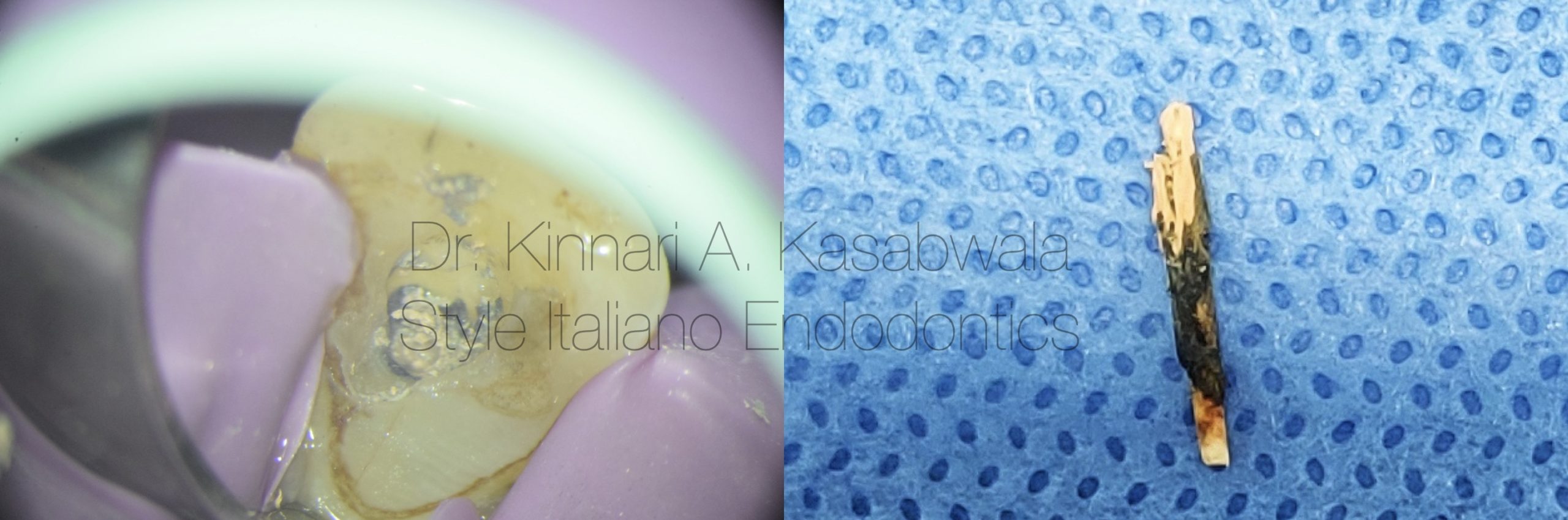
Fig. 2
Under rubber dam isolation and using dental operating microscope,
removal of coronal restoration showed poorly compacted GP.
Existing GP points were removed using re-treatment rotary files and H files using minimal apically directed pressure.
Upon in toto retrieval of GP there was evidence of pus discharge from the canal.

Fig. 3
Arbitrary WL determination was done with apex locator and confirmed with IOPA.
Since 140 size K file was freely passing through the apex, a decision for apexification was made.
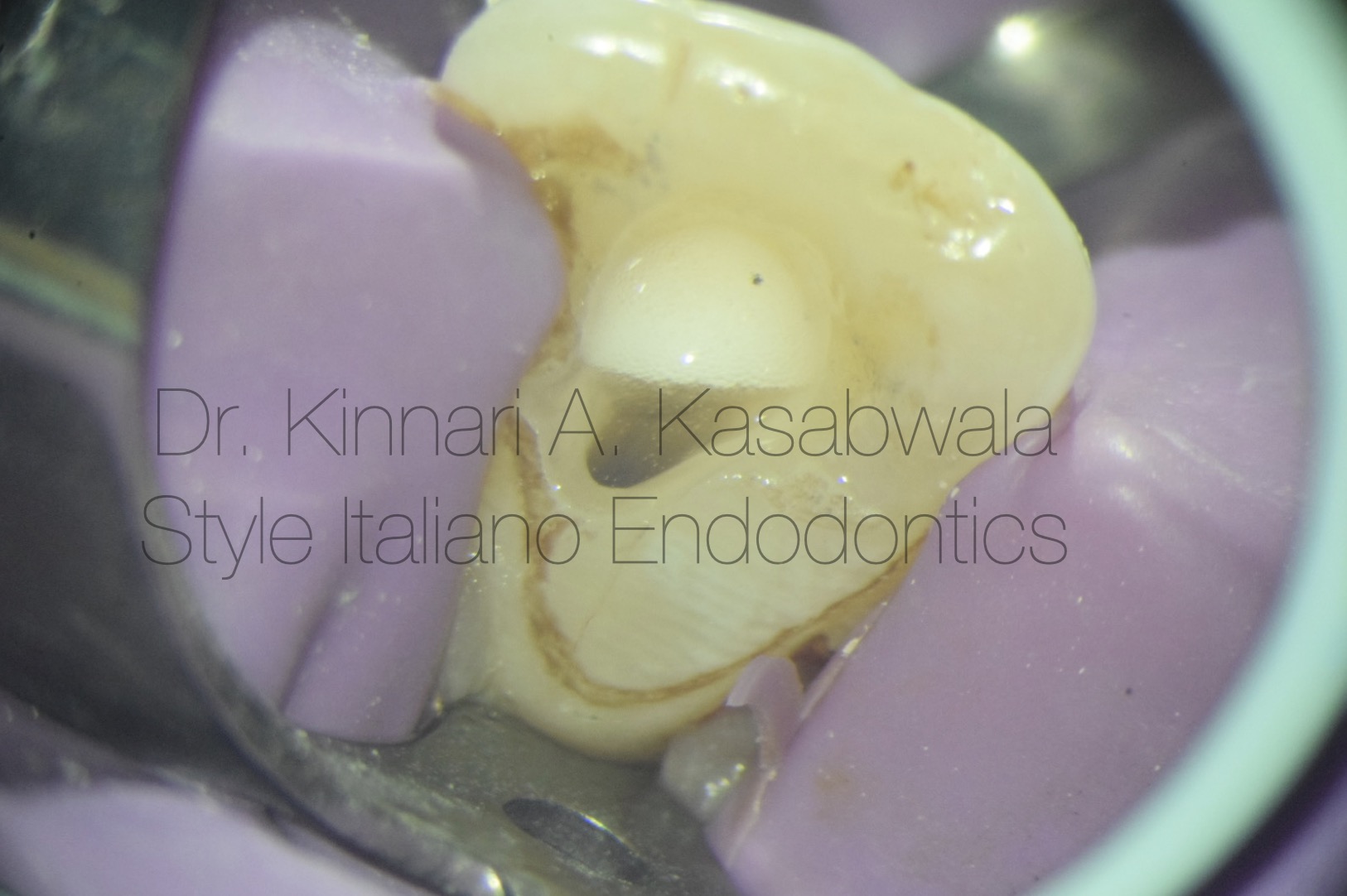
Fig. 4
Minimal instrumentation and circumferential filing was done with K files to remove infected dentin and sealer remnants.
Owing to the open apex, Sodium hypochlorite was diluted in saline and expressed in the canal using 30 gauge side vented needle. Irrigation activation was done with Endoactivator (Dentsply) kept 3 mm short of the determined WL to avoid inadvertent extrusion.

Fig. 5
Calcium hydroxide interim intracanal medicament given for 2 weeks due to weeping canal.

Fig. 6
Canal was rinsed with saline and EDTA to rinse out CaOH and smear layer.
Canal was finally disinfected with diluted NaOCL.

Fig. 7
Plugger fit check was done at 2nd appointment after confirming dry canal using paper points and inspection under microscope.
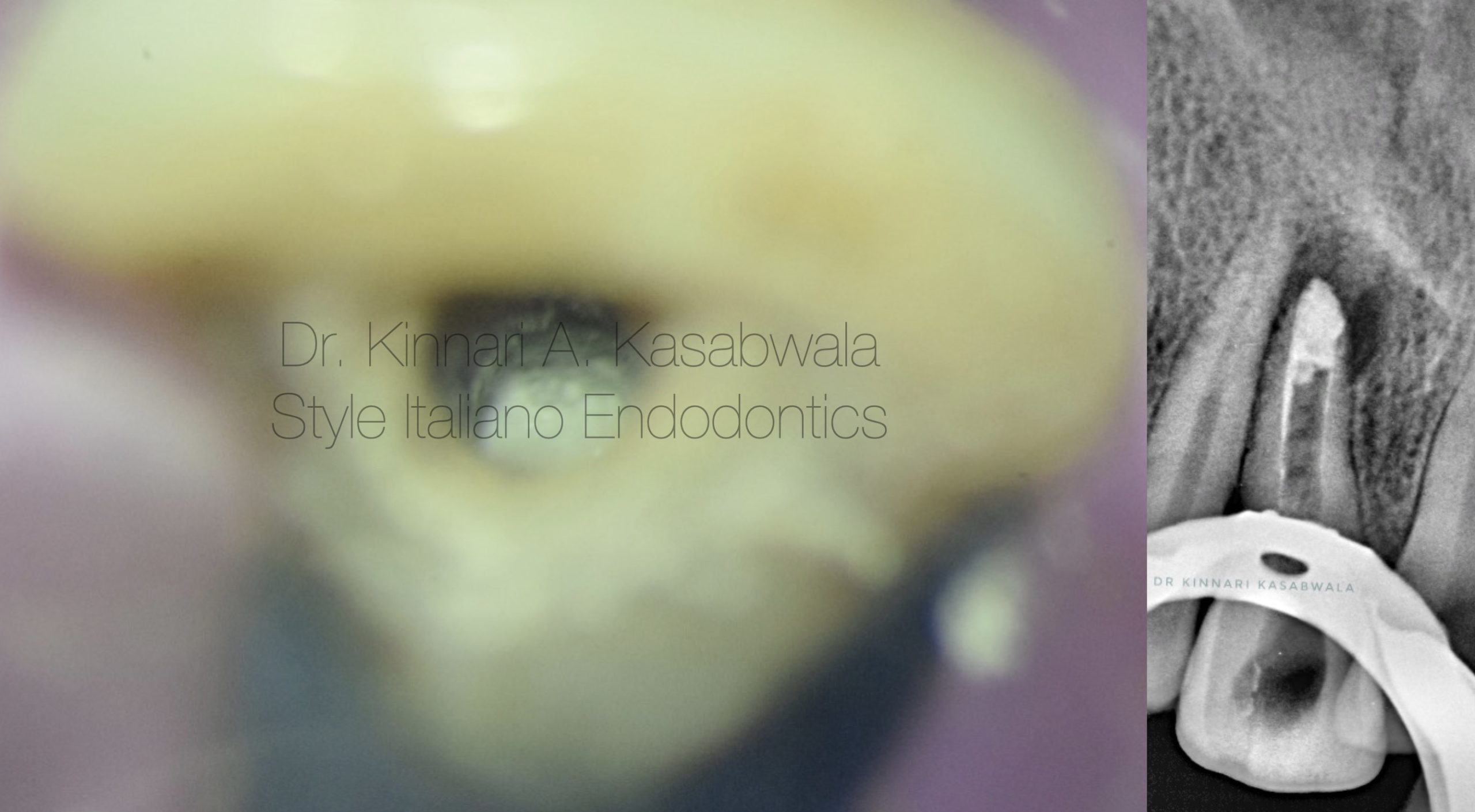
Fig. 8
Incremental placement of White MTA (Angelus) was done at apex, using Angelus MTA carrier.
After placement, MTA was compacted with pluggers (Dentsply Maillefer) and butt end of paper points, to form an apical plug.
Excess MTA along the walls was removed using moist paper points.
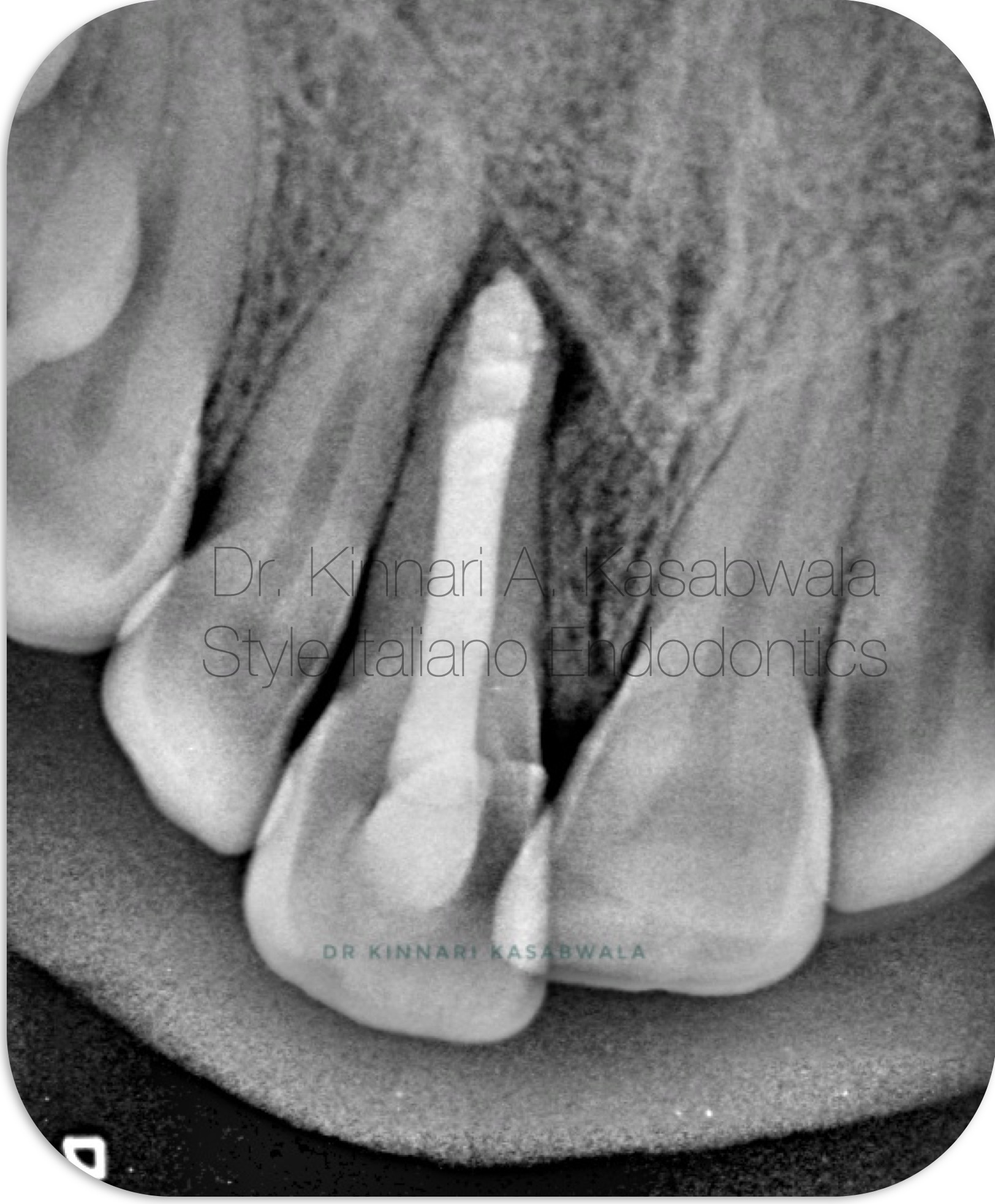
Fig. 9
The remainder canal was later backfilled with thermoplastic gutta percha (EQV –Meta Biomed) and Bio-C sealer (Angelus).
Immediate composite coronal restoration done.

Fig. 10
Inverted immediate post-op IOPA
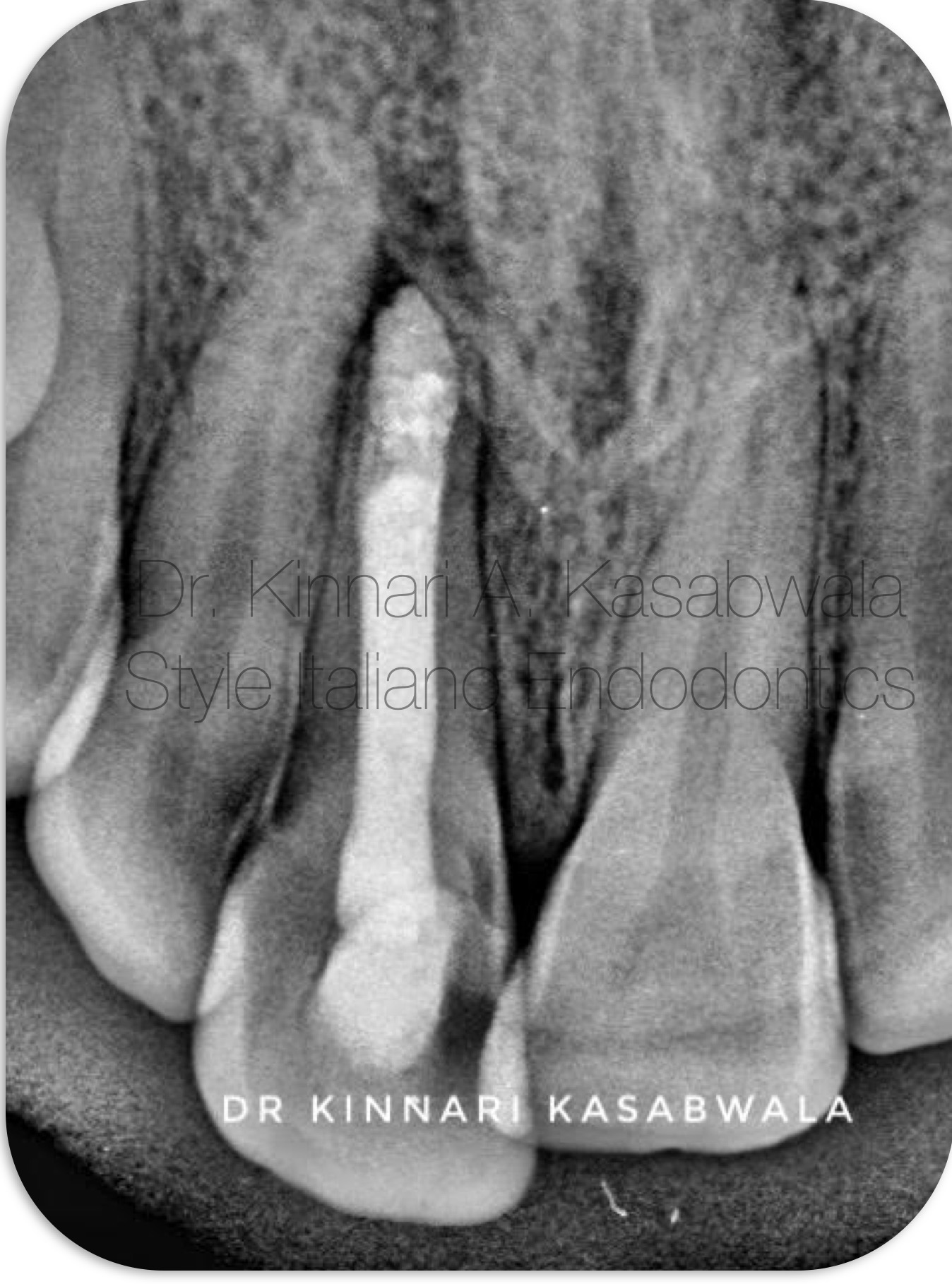
Fig. 11
1 month Recall IOPA
Shows uneventful healing in progress
Subsided pain and healing sinus tract clinically.

Fig. 12
Case 2:
18 year old patient complained of intermittent swelling, throbbing pain and occasional pus discharge.
H/O trauma 8-9 years ago
H/O RCT 2 years ago and development of symptoms since 1.5 years.
Clinically tooth 11 was discoloured.
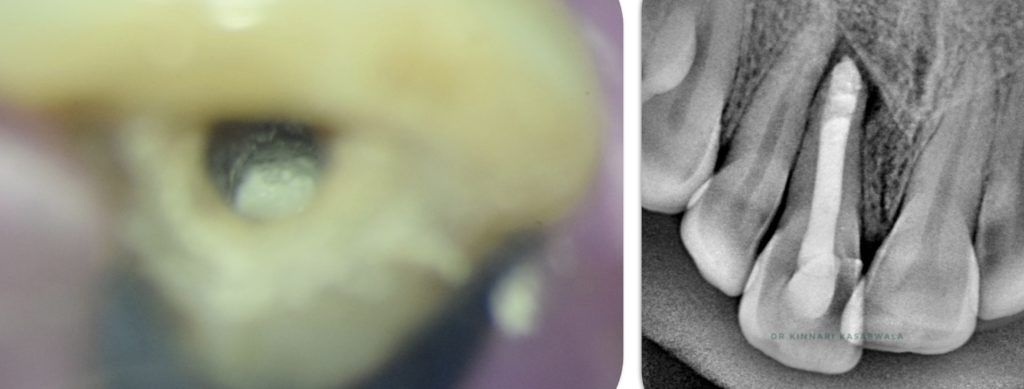
IOPA showed conventional RCT done with gutta percha point and incomplete apical seal and large periapical lesion and dislodged coronal restoration.

Fig. 13
Under rubber dam isolation, using Dental operating microscope, existing coronal restoration was removed, access opening was modified and GP was removed.
Canal was cleaned and shaped with minimal instrumentation.
Since 60 size K file was freely passing through the apex, a decision for apexification was made.
Sodium hypochlorite diluted in saline was used for irrigation using 30 gauge side vented needle. Agitation of NaOCL was done with Endoactivator (Dentsply) kept 3 mm short of the determined WL to avoid extrusion.

Fig. 14
2 cycles of Interim calcium hydroxide dressing were given, each spanning 2 weeks, to arrest weeping canal.

Fig. 15
Canal was rinsed with saline and EDTA to rinse out CaOH and smear layer.
Canal was finally disinfected with diluted NaOCL.
After confirming dry canal using paper points under microscope,
- Plugger fit check was done
- Incremental placement of Biodentine (Septodont) was done at the apex, using Angelus MTA carrier
- Biodentine was compacted with pluggers (Dentsply Maillefer), and butt end of paper points to form an apical plug.

Fig. 16
Immediate post-op IOPA
Backfilling from Biodentine apical plug till coronal third was done with thermoplastic gutta percha (EQV –Meta Biomed) and Bio-C sealer (Angelus).
Composite coronal restoration was done in the next visit.

Fig. 17
3 months post-op IOPA
Shows diffuse bone formation within the radiolucency
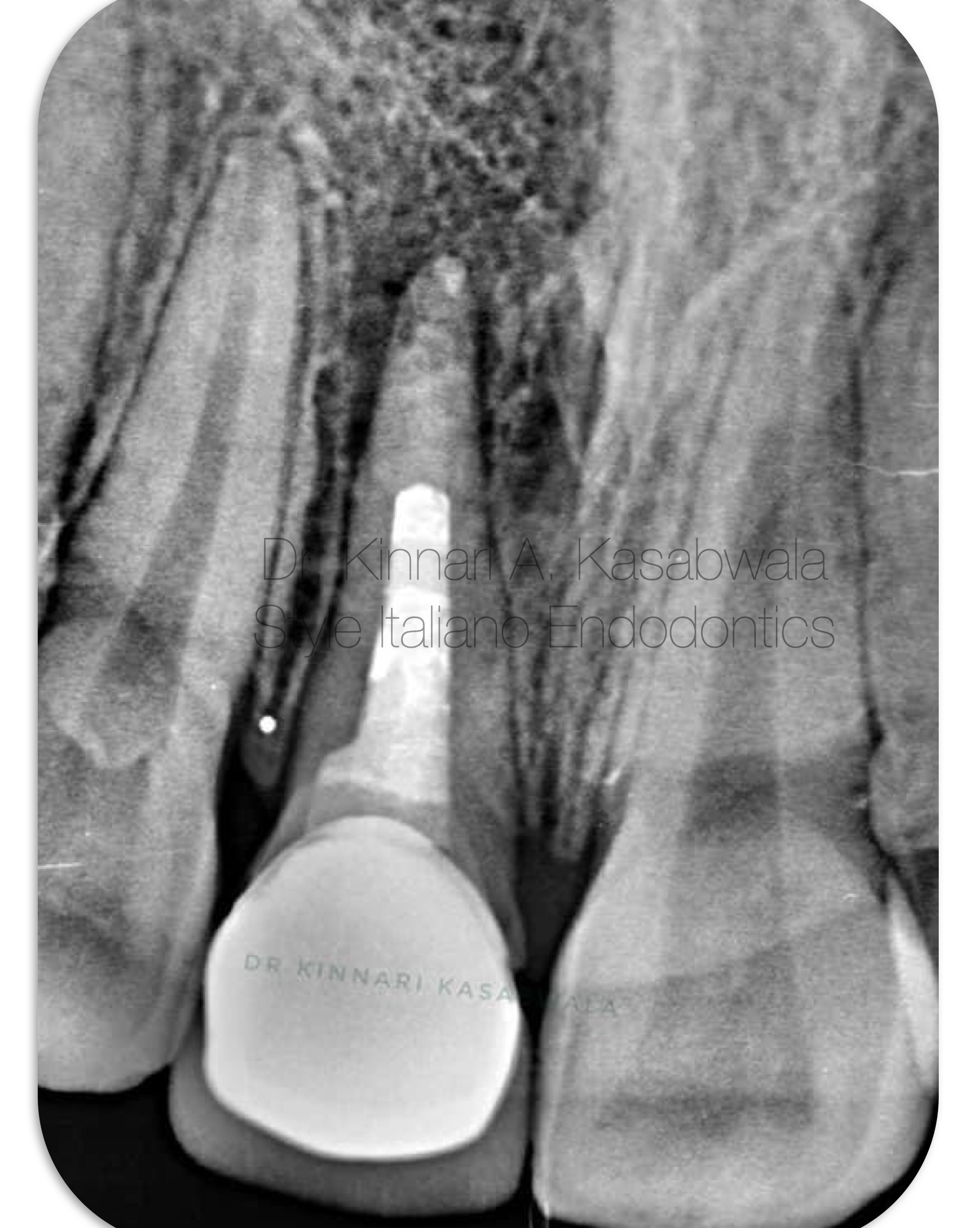
Fig. 18
15 months post-op IOPA
Shows significant healing with complete cessation of symptoms.

Fig. 19
15 months post-op IOPA (inverted)

Fig. 20
Dr Kinnari Abhilash Kasabwala
- B.D.S. from Nair hospital dental college, Mumbai (2011-2016)
- M.D.S. specializing in Conservative dentistry and Endodontics from Meenakshi Ammal dental college and hospital, MAHER University, Chennai (2017-2020)
She is awarded with the following:
- "Emerging star 2019" for being the outstanding postgraduate by Conservative dentistry and endodontics association of Tamil Nadu
- Selected as top finalist at the National level in Endodontics for "Young Achiever award 2020" by Indian association of conservative dentistry and endodontics IACDE.
- Gold medal from MAHER university for securing first position in MDS final examination.
- "Best outgoing student" for year 2020 by Conservative dentistry and endodontics department of Meenakshi Ammal dental college and hospital, Chennai
- Awarded "Best student of the year" for years 2017-2018, 2018-2019, 2019-2020 amongst the post graduate students at Endodontics department Meenakshi Ammal dental college and hospital
She is a patent holder of "Indigenous cost-effective biofilm flow cell model and bubble trap" under Intellectual property India, Government of India.
She has authored and co-authored several publications in National and International journals.
She is recently inducted as a national key opinion leader with Bombay dental surgical.
She is recently inducted as a fellow with Style Italiano endodontics forum from May 2023.
Dr. Kinnari Kasabwala is currently practising as a private practioner, specializing in micro-endodontics at Dr Kasabwala dental speciality clinic in Mumbai.
Her interests are Endodontics, Dental aesthetic procedures and multi-disciplinary dentistry.
Conclusions
Conclusion:
Whenever there is adequate crown-root ratio in immature necrotic permanent teeth that are less likely to fracture over time, MTA apexification may be a suitable treatment option.
However, apexification procedure is incredibly challenging, time-consuming and technically complex due to risk of extrusion because of absence of an apical barrier and technique sensitivity in creation of an apical seal.
Bibliography
Rafter M. Apexification: A review. Dent. Traumatol. 2005;21:1–8.
Panda, P., Mishra, L., Govind, S., Panda, S., & Lapinska, B. (2022). Clinical Outcome and Comparison of Regenerative and Apexification Intervention in Young Immature Necrotic Teeth-A Systematic Review and Meta-Analysis. Journal of clinical medicine, 11(13), 3909.
Nicoloso, G. F., Goldenfum, G. M., Pizzol, T. D. S. D., Scarparo, R. K., Montagner, F., de Almeida Rodrigues, J., & Casagrande, L. (2019). Pulp Revascularization or Apexification for the Treatment of Immature Necrotic Permanent Teeth: Systematic Review and Meta-Analysis. The Journal of clinical pediatric dentistry, 43(5), 305–313.
Xie, Y., Lu, F., Hong, Y., He, J., & Lin, Y. (2021). Revascularisation versus apexification for treatment of immature teeth based on periapical healing and root development: A systematic review and meta-analysis. European journal of paediatric dentistry, 22(3), 207–214. https://doi.org/10.23804/ejpd.2021.22.03.6
Guerrero F., Mendoza A., Ribas D., Aspiazu K. Apexification: A systematic review. J. Conserv. Dent. 2018;21:462–465.
Cervino, G., Laino, L., D'Amico, C., Russo, D., Nucci, L., Amoroso, G., Gorassini, F., Tepedino, M., Terranova, A., Gambino, D., Mastroieni, R., Tözüm, M. D., & Fiorillo, L. (2020). Mineral Trioxide Aggregate Applications in Endodontics: A Review. European journal of dentistry, 14(4), 683–691