Immature tooth with apical periodontitis and sinus tract undergoes apexogenesis. A case report.
28/04/2022
The Community
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
It is believed that Apical Periodontitis develop in teeth where the pulp is necrotic.
However, some studies show that remnants of vital pulp tissues might still be in the canal even in teeth with signs of pulp necrosis. In open apex cases, those remnants of vital pulp tissues can be important in achieving desired outcomes like maturation of the root even if there is apical periodontitis and sinus tract, as we will see in this case.
In this case, a 12 years old girl presented with history of pain from tooth 15. Clinically, a buccal sinus tract and discomfort in the area of the tooth were recorded.

Fig. 1
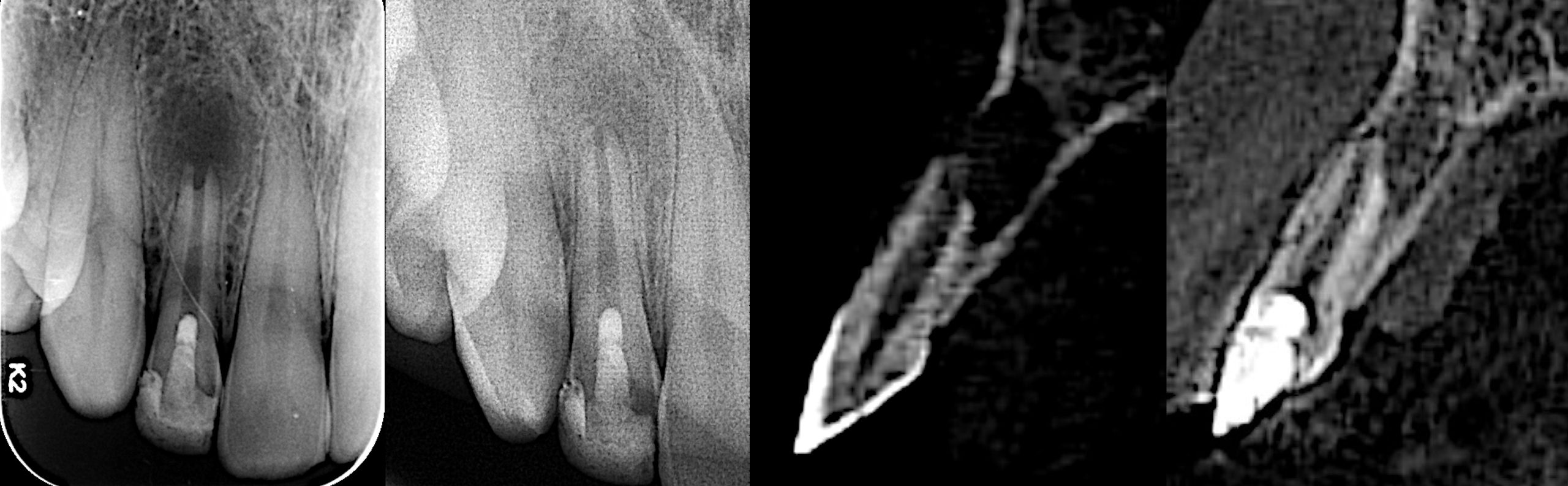
The Preoperative X-ray by referral dentist shows tooth 15 with immature root, open apex and periapical radiolucency.
Cause of the lesion is not known.

Fig. 2
Sinus tract tracing with GP cone, confirms that tooth 15 is the cause. Cold test was negative.
Based on the examination, diagnosis was pulp necrosis with chronic apical abscess.
Treatment plan was to do calcium hydroxide dressing, and MTA apexification in the next visit.
Given that the tooth seems to be intact, tooth was opened intentionally without anesthesia (aka drill test). The coronal part of the pulp was necrotic. However, inserting a file inside the canal provoked pain and bleeding deep in the canal, which means that there is some remnants of vital pulp.
So, the pulp status is partial necrosis.
Without any instrumentation, 3.25% sodium hypochlorite irrigation and Calcium Hydroxide dressing was done.
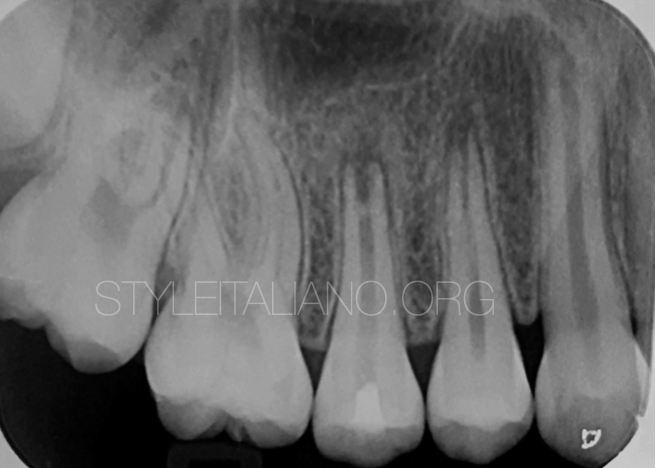
Fig. 3
2 months later, the tooth is asymptomatic, and the buccal sinus tract has healed.
A PA radiograph was taken before the treatment. We can see reduction of the size of the PA lesion and we can notice the formation of a calcified barrier at apical third, with slight thickening of canal walls.
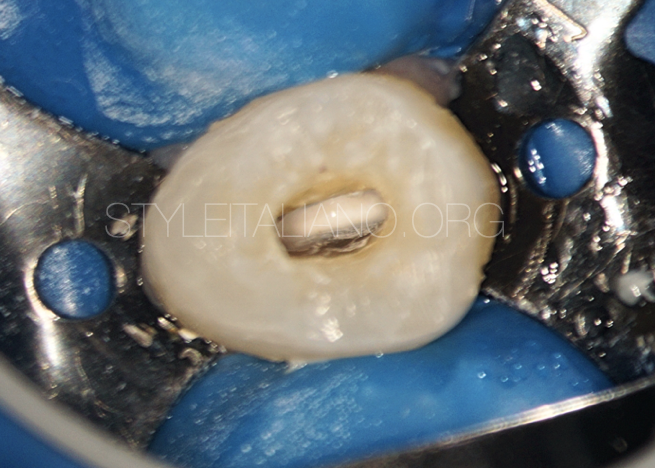
Fig. 4
Calcium Hydroxide from previous visit.
This video shows the calcified barrier that is formed by the remnants of the vital pulp tissues that were in the canal, as a response to calcium hydroxide dressing.
A calcified tissue can be noticed inside the canal at the apical third which also was obvious clinically under the operating microscope.
Seeing this, I changed the treatment plan, and decided to obturate the canal up to the calcified barrier.

Fig. 5
Calcified barrier
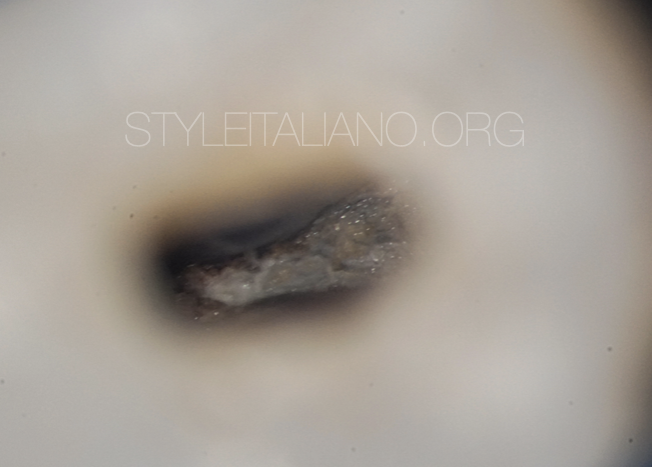
Fig. 6
Calcified barrier in high magnification.
The barrier is stable and sealing the canal.
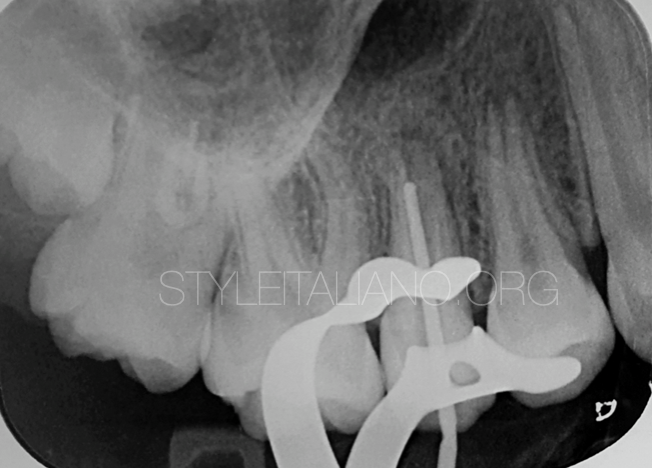
Fig. 7
Length confirmation

Fig. 8
The apical part of the root was sealed with MTA, then thermoplasticized GP, and a permanent filling.
MTA was positioned in increments by using MAP system (Produits Dentaires, Vevey, Switzerland).

Fig. 9
An intra operative x-ray was taken to confirm the position of initial MTA increment

Fig. 10
MTA plug is ready
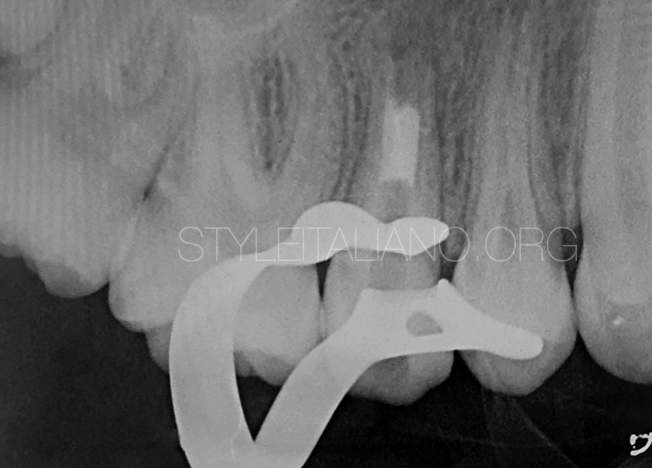
Fig. 11
MTA plug

Fig. 12
The coronal portion if the canal is filled by thermoplasticized Gutta Percha

Fig. 13
Immediate Post Operative

Fig. 14
5 months follow up
The tooth is asymptomatic. The PA lesion has healed, with further thickening of canal walls at apical third, but apex is still open.

Fig. 15
13 Months follow up.
The tooth is asymptomatic.
Radiographically, apex is closed, mainly by canal walls thickening and minimal elongation.
We can notice canal obliteration, and PDL formation, with continuous lamina dura.

Fig. 16
The author:
Dr. Foad Ganem
Graduated in 2010 from Jordanian University of Science and Technology (Jordan).
Since 2012, practice limited to Endodontics, with a lot of experience in immature teeth and open apex management.
In the last few years, interested in dental photography and video documentation
Conclusions
In open apex cases with pulpal involvement, the ultimate goal of the treatment is to preserve vitality of the pulp as much as we can.
Sometimes, even in teeth that seem to be necrotic with apical periodontitis, there might be some remnants of vital pulp tissues.
If that is the case, then it is worth to try pulpotomy as a treatment option, so we could get desired outcomes such as thickening of canal walls and complete apical closure as we saw in this case.
Bibliography
Chueh LH, Huang GT. Immature teeth with periradicular periodontitis or abscess undergoing apexogenesis: a paradigm shift. J Endod. 2006 Dec;32(12):1205-13. doi: 10.1016/j.joen.2006.07.010. Epub 2006 Oct 13. PMID: 17174685.
Tsukiboshi M, Ricucci D, Siqueira JF Jr. Mandibular Premolars with Immature Roots and Apical Periodontitis Lesions Treated with Pulpotomy: Report of 3 Cases. J Endod. 2017 Sep;43(9S):S65-S74. doi: 10.1016/j.joen.2017.06.013. Epub 2017 Aug 1. PMID: 28778508.
Edanami, N., Yoshiba, K., Shirakashi, M. et al. Impact of remnant healthy pulp and apical tissue on outcomes after simulated regenerative endodontic procedure in rat molars. Sci Rep 10, 20967 (2020). https://doi.org/10.1038/s41598-020-78022-w