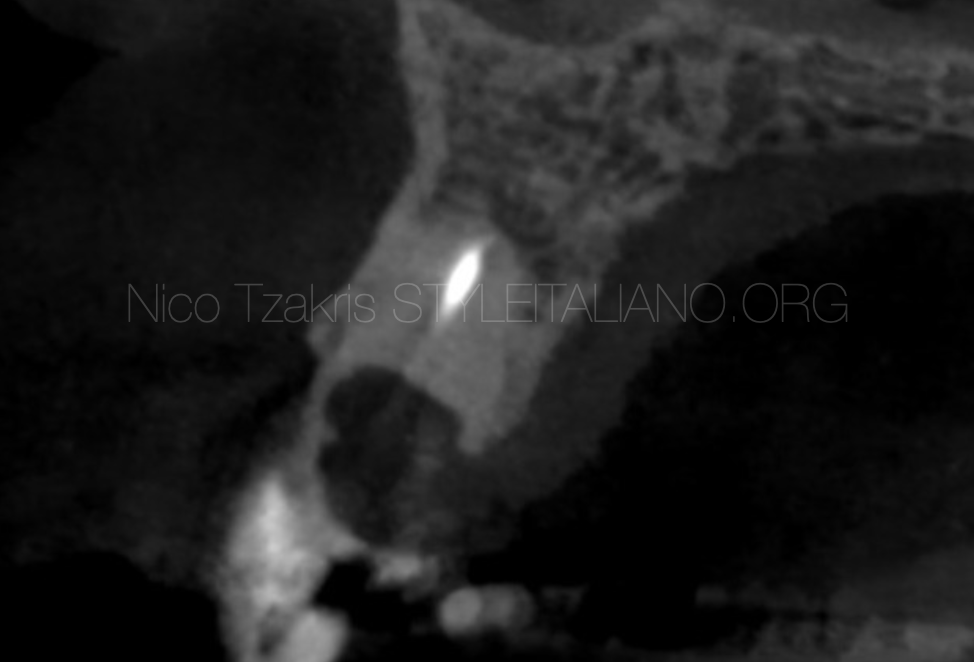
Preservation of compromised teeth can be challenging, especially when an extensive periapical lesion is affecting prognosis.

 The fine line between extraction and retreatment: a conservative approach to a compromised premolar — 24-Month Follow-Up
The fine line between extraction and retreatment: a conservative approach to a compromised premolar — 24-Month Follow-Up
Preservation of compromised teeth can be challenging, especially when an extensive periapical lesion is affecting prognosis.
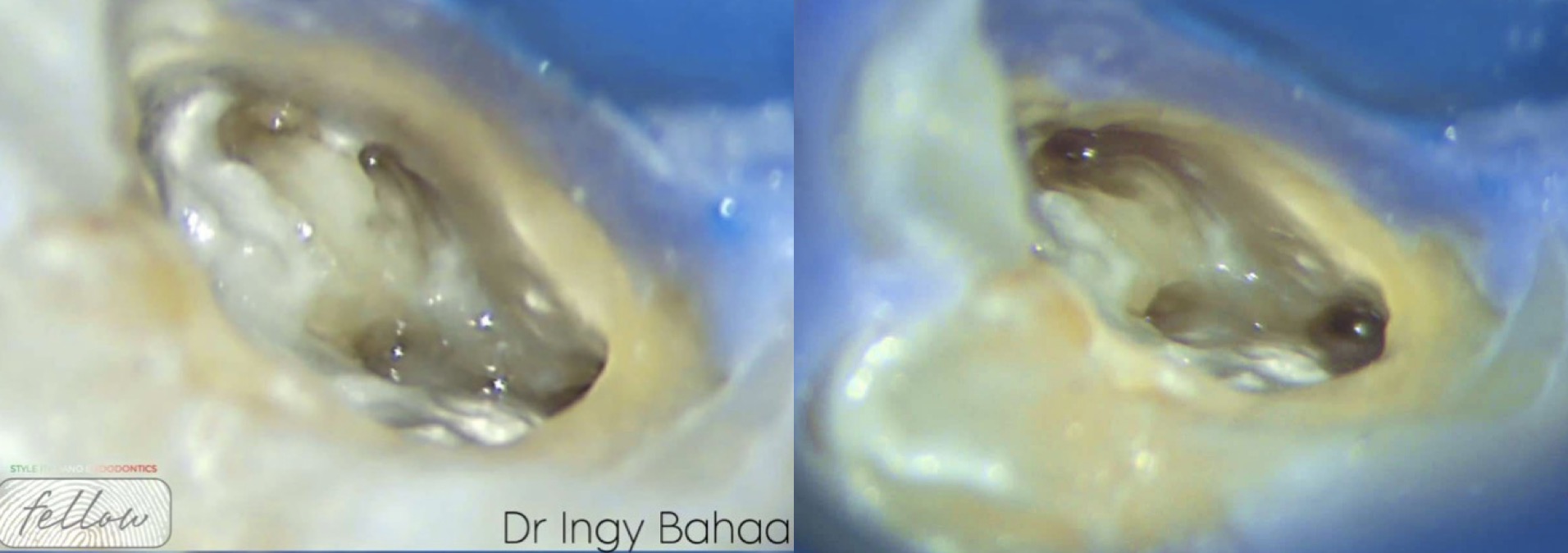
 Saving the unsavable: Intentional replantation
Saving the unsavable: Intentional replantation
Where do we draw the line and accept the extraction as a treatment option in endodontics? Is there a limit of what endodontics can achieve? Today we will discuss about intentional replantation and how it can provide us with a solution beyond the borders of conventional root canal treatment presenting a case with a two year follow up.
 Rising case study
Rising case study
Anatomy is one of the biggest challenges in the root canal treatment. During the step of shaping lots of errors may happen like zipping, ledges, transportation, straightening the anatomy and file […]
 Coalescence Phenomena of MB2 Canal
Coalescence Phenomena of MB2 Canal
The Presence of Second Mesio-buccal canal in Upper Molars is One of the most common scenarios of Anatomical Variations. According to Studies from Different Middle Eastern Countries, The prevalence of […]
 Regenerative endodontics: a case report
Regenerative endodontics: a case report
Obtaining a proper seal in immature teeth is a difficult task because of the wide apical delta it presents. But regernerative endodontics gives us the chance to create pulp in […]
 Non-Surgical Retreatment of Tooth 46 with Stripping Perforation: A Case Report
Non-Surgical Retreatment of Tooth 46 with Stripping Perforation: A Case Report
This case details the non-surgical retreatment of tooth 46 in a 40-year-old female presenting with symptomatic apical periodontitis. Clinical and radiographic evaluation revealed a poorly adapted crown, metallic posts, secondary […]
 The best implant is your natural tooth
The best implant is your natural tooth
Dental trauma is a significant public health concern, often resulting from accidents, sports injuries, or falls. Among the various types of dental injuries, avulsion and extrusion represent severe forms of […]
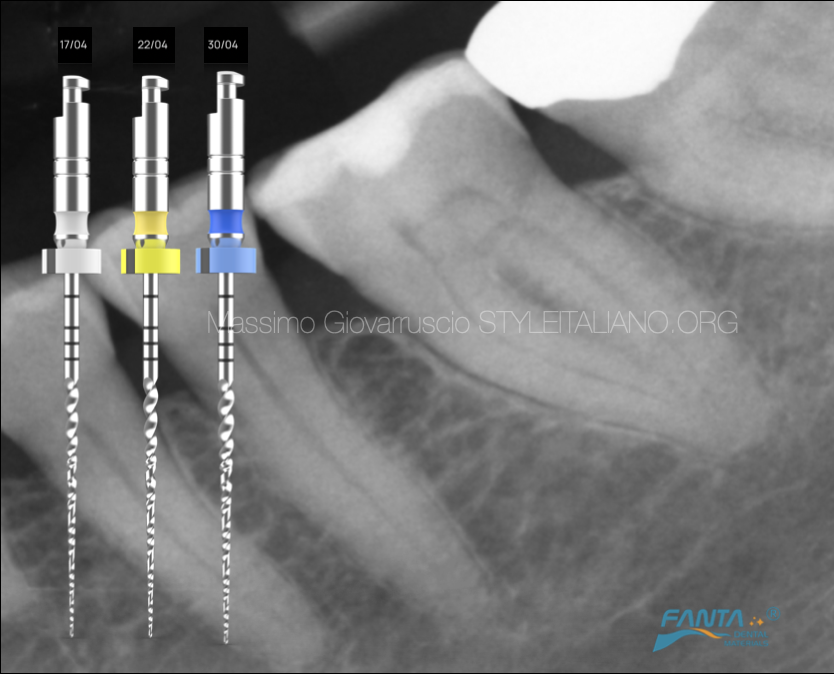
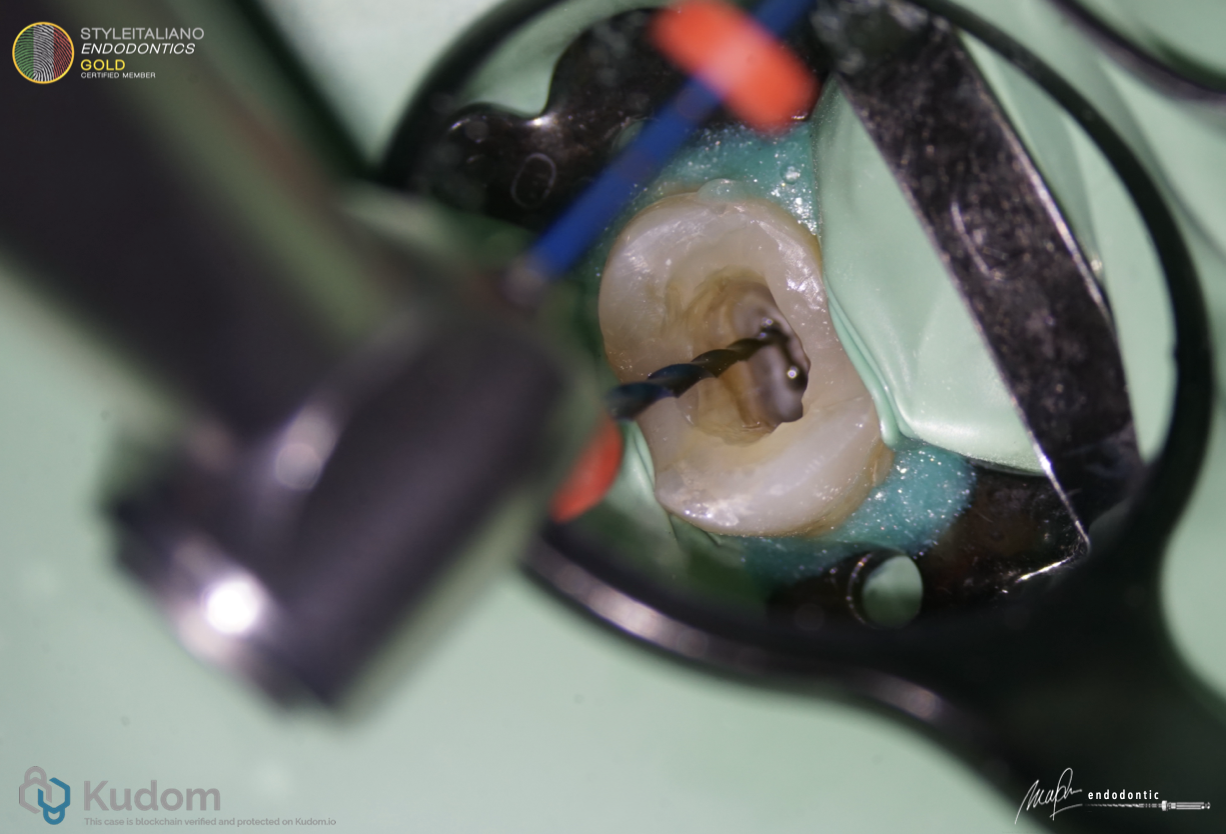 Clinical Application of R One Mini that Emphasises on Dentin Preservation
Clinical Application of R One Mini that Emphasises on Dentin Preservation
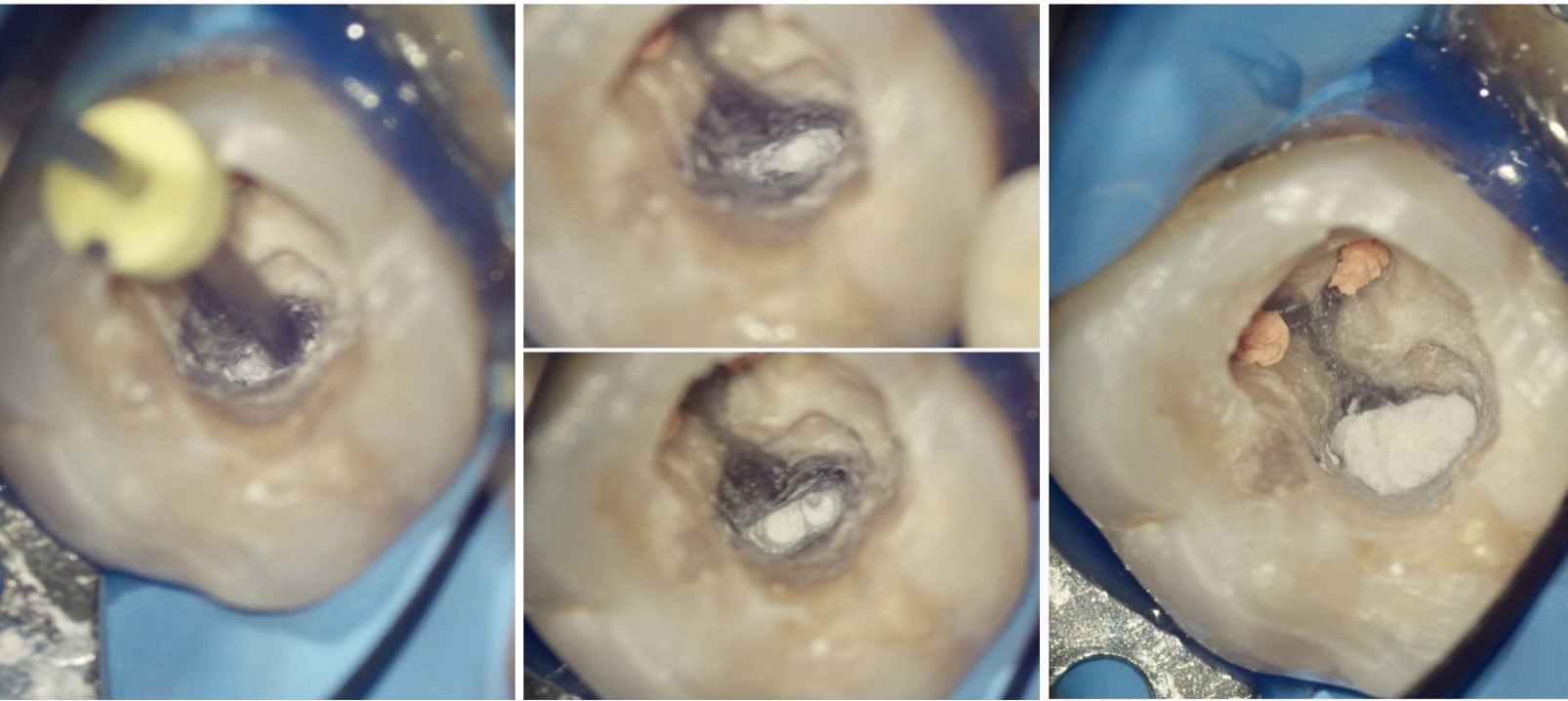
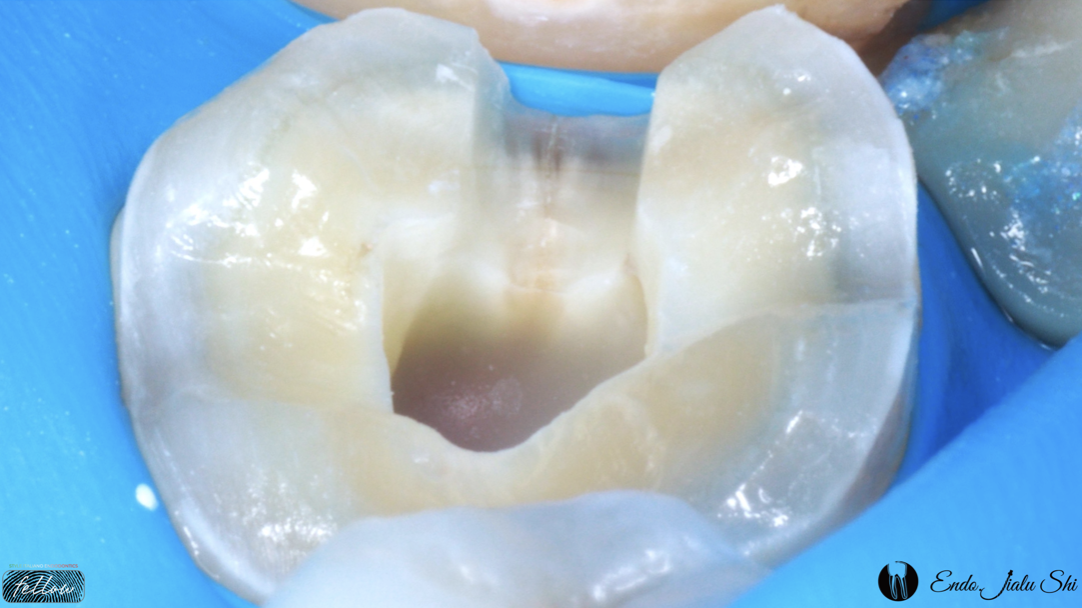
Endodontic treatment aiming to cure and prevent apical periodontitis to retain tooth as long as possible, functioning without symptoms. In order to achieve this, we must performed root canal preparation to reduce bacteria to the level that necessary, this mean we shape and clean the root canal system to its terminus.
But we need to bear in mind that in order to achieve long term predictability we also need to save tooth structure specially the PCD area in order tooth to withstand occlusal force for period of time
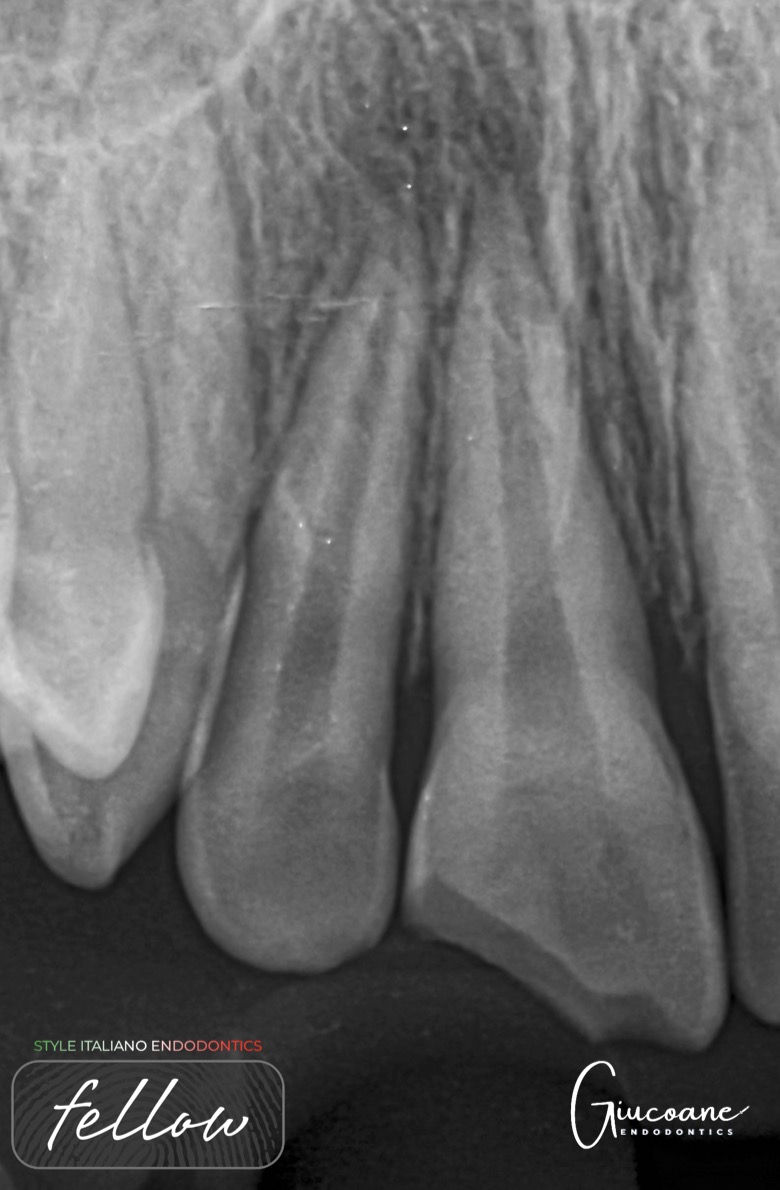
 Treatment of an external inflammatory root resorption
Treatment of an external inflammatory root resorption
External inflammatory resorption (EIR) is present on the external surface of the root of majority of the teeth diagnosed with chronic apical periodontitis. EIR also affects teeth that suffer severe […]
 One-visit RCT of a cracked tooth
One-visit RCT of a cracked tooth
Cracked teeth have always been a difficult problem. The rate of cracked teeth increased during the initial outbreak of the COVID-19 pandemic; several studies provided evidence on the association between […]
 Treating curved canals with Harmony files
Treating curved canals with Harmony files
The primary goal of root canal shaping is to create a continuously tapered, funnel-shaped canal while preserving the original anatomy. This is significantly harder to achieve in a curved canal […]
 UL6 with unusual anatomy
UL6 with unusual anatomy
The incidence of MB2 and MB3 in upper first molars is low (Ronald Ordinola-Zapata et al., 2020), however one of the most common reasons for endodontic failures is missed anatomy […]