

Treatment of an extensive radicular fracture: the pre-endodontic restoration of a structurally compromised tooth. Part 1
29/05/2022
Davide Guglielmi
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Trauma related fractures are one of the most common types of dental injury in the permanent dentition.
The purpose of this case report is to present a multidisciplinary management of a sub-gingival crown- root fracture in a patient. Management of traumatic dental injuries (TDI) should involve a multidisciplinary approach to optimize healing while maintaining function and esthetics.
The challenge is to identify the most suitable treatment for a given patient combining evidence-based guidelines to clinical experience.
Since the 50s, we have seen arising several classifications in our scientific literature. All of these aimed to codify traumatic dental lesions based on topographic and morphological criteria. The International Association of Dental Traumatology (IADT) has developed in 2017 a consensus statement based on a review of the currently available dental scientific literature(4) .
This classification defines fractures as: (Fig. 1)(7)
infractions, enamel fractures, enamel-dentine fractures, enamel-dentine-pulp fractures, crown-root fracture without pulp exposure, crown-root fracture with pulp exposure (complicated), root fracture, alveolar fracture, concussion, subluxation, extrusive luxation, lateral luxation, intrusive luxation. Complicated crown-radicular fractures, involving the enamel, dentin, and pulp, account for up to 20% of all TDJ, the majority of them occurring in the maxillary anterior region. From the guidelines of the International Association of Dental Traumatology emerges that, in case of crown-radicular fractures with pulp exposure (without open apex), different therapies can be performed, such as the removal of the coronal fragment with subsequent endodontic treatment, followed by gengivectomy/gengivectomy + ostectomy and osteoplasty, and a restoration with a post retained crown (4).
The clinical case we are presenting through this report shows a new conservative approach which combines a pre-endodontic reconstruction with and a split full buccal envelope opened flap.
Restorability assessment is essential before proceeding with the endodontics treatment. This should include an overall evaluation of the restorative status of the tooth (structural, periodontal and endodontic).(3)
Both the limited residual tooth tissue and the sub-gingival margins of the root fractures complicate the endodontics procedures (8).
The sub-gingival margins of root fractures are associated with biological and technical problems such as difficulty in isolating the working field with a dental dam, adhesion procedures, impression taking and final positioning of the restoration itself in relation with the sopra-crestal tissue attachment (STA)(1). The supra-crestal tissue attachment (STA), formerly known as biologic width, consists in the junctional epithelium and supra-crestal connective tissue attachment.
STA violation is believed to trigger adverse periodontal effects, although the specific aetiology (which has been proposed to be biofilm, trauma, material toxicity or a combination of these factors) is not clear. Mean STA apico-coronal dimension is found to be 2.15–2.30 mm; however, considerable variability exists according to tooth type, site, periodontal health and periodontal phenotype.
Definitive assessment of restorability should be performed only after total removal of previous restorations, caries and unsupported tooth tissue.
A pre-endodontic restoration could be successful for various reasons: (3)
- it improves isolation quality for the subsequent endodontics treatment,
- it creates space for prolonged function of irrigation solutions,
- it allows effective inter-appointment temporisation to prevent bacterial microleakage, seepage of intracanal medicaments and gingival ingrowth into the cavity,
- it prevents fractures of the weakened tooth structure, thus maintaining repeatable reference points
- it improves aesthetics during the endodontic treatment period, thus enhancing patients’ acceptance,
- it facilitates post-endodontic restoration.
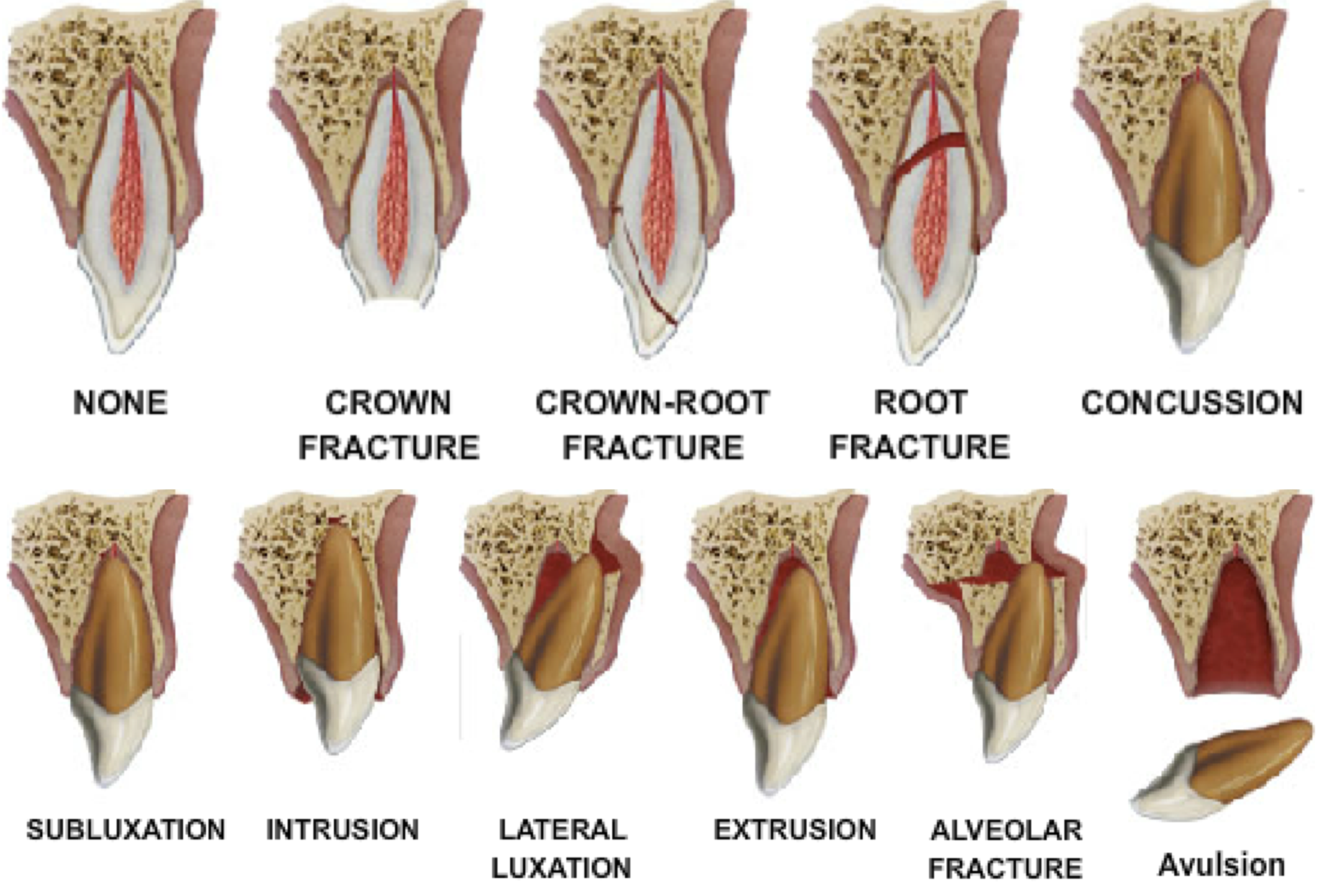
Fig. 1
Schematic Illustration of Fractures and Luxations of Permanent Teeth (7).
Diangelis AJ, Andreasen JO, Ebeleseder KA, et al. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 1. Fractures and luxations of permanent teeth. Dent Traumatol 2012;28:2-12.
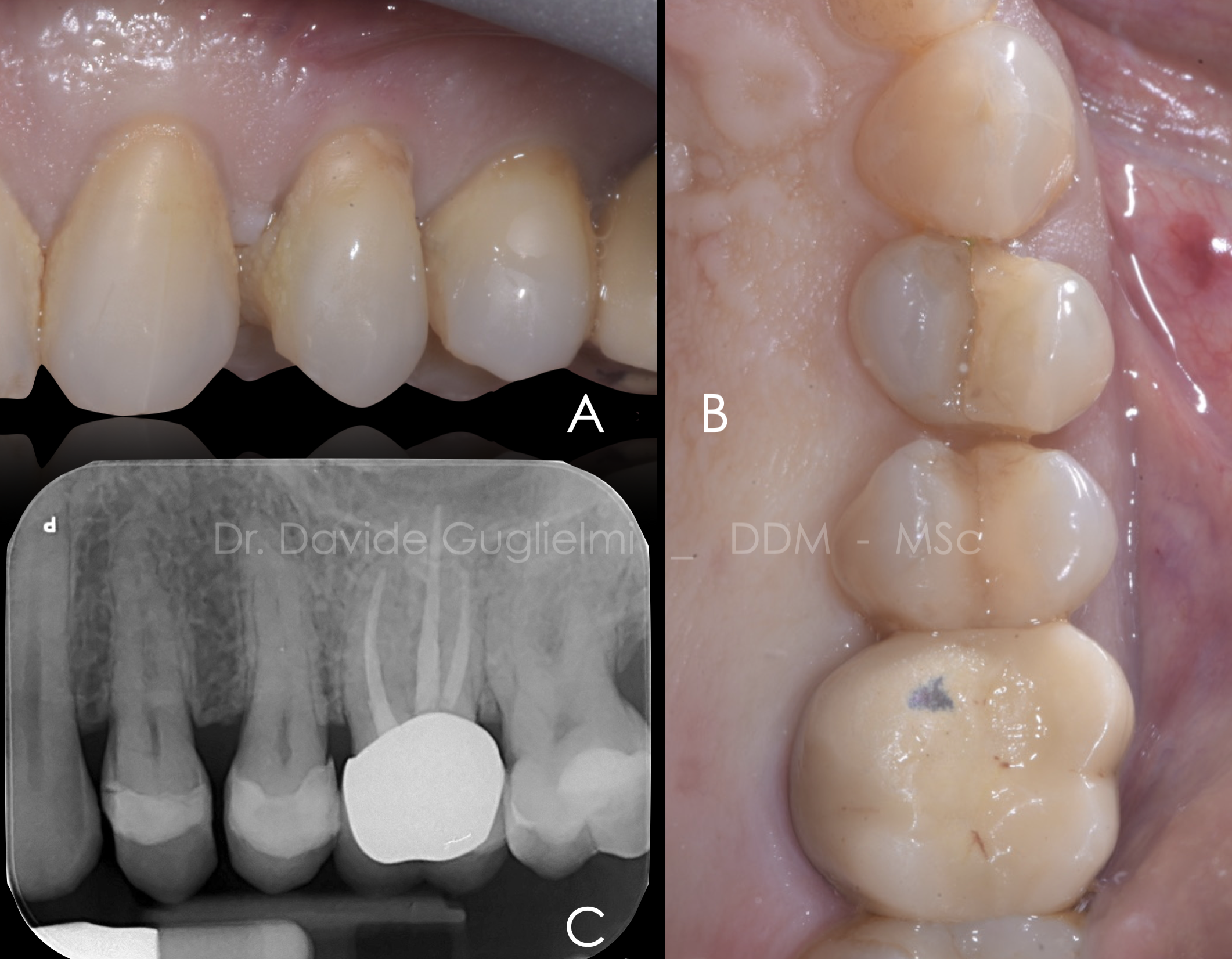
Fig. 2
Case of a 66 years old patient referring pain in the left upper jaw when chewing.
Both sensibility testing and bleeding on probing are negative, pocket probing depth of the element 2.4 is ≤ 5 mm circumferentially.
Higher mobility and pain during the percussion test are recorded.
A: lateral view
B: occlusal view
C: periapical X-Ray
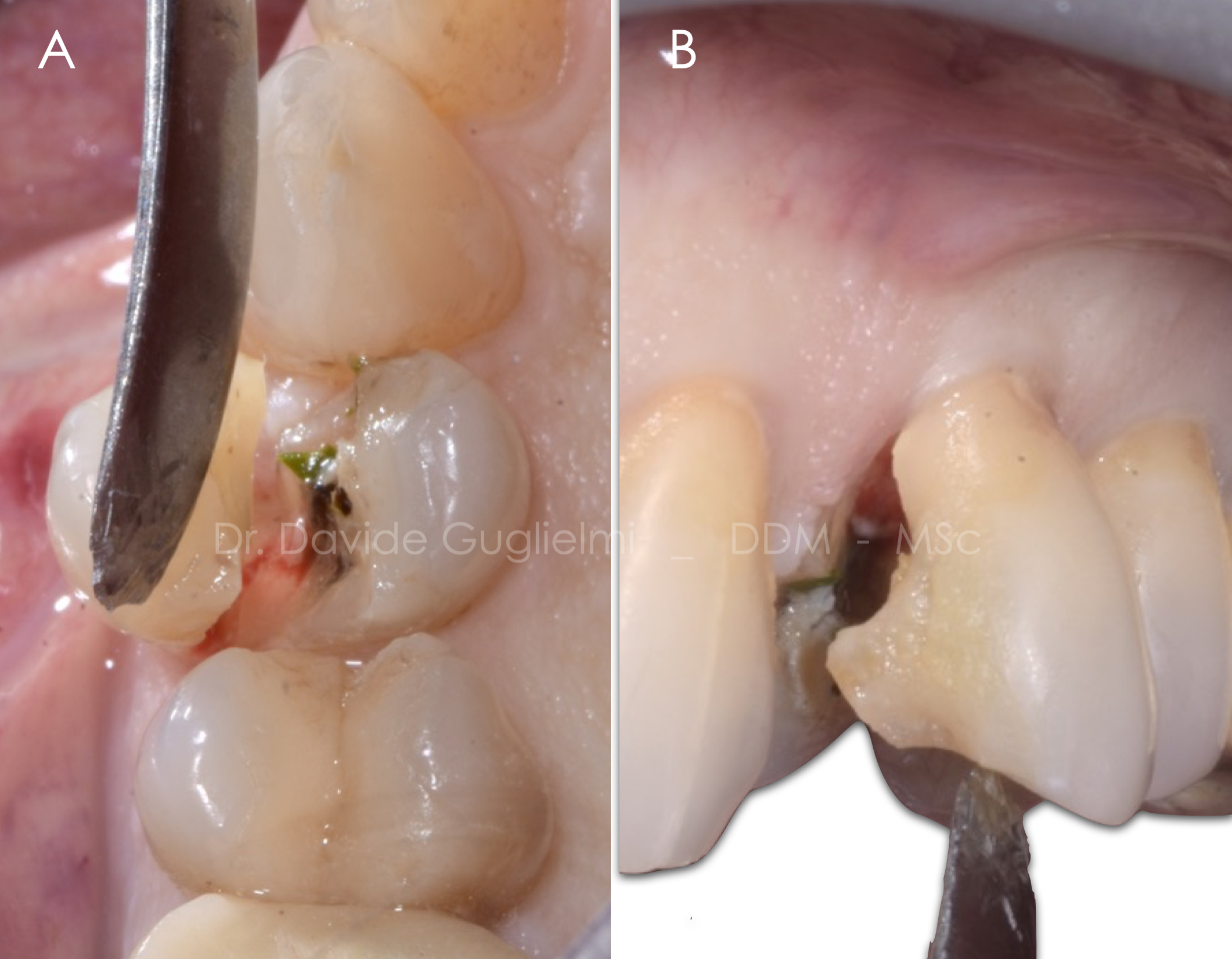
Fig. 3
Naturally, a proper diagnosis, treatment planning and follow up visits are important to achieve a favorable outcome.
After a correct diagnosis and a local anesthesia it was possible to start removing the fractured portion of the tooth.

Fig. 4
Once the fracture line was exposed it was possibile to classify the fracture as vertical crown-root fracture.
The exposure of the pulp is also noticeable.
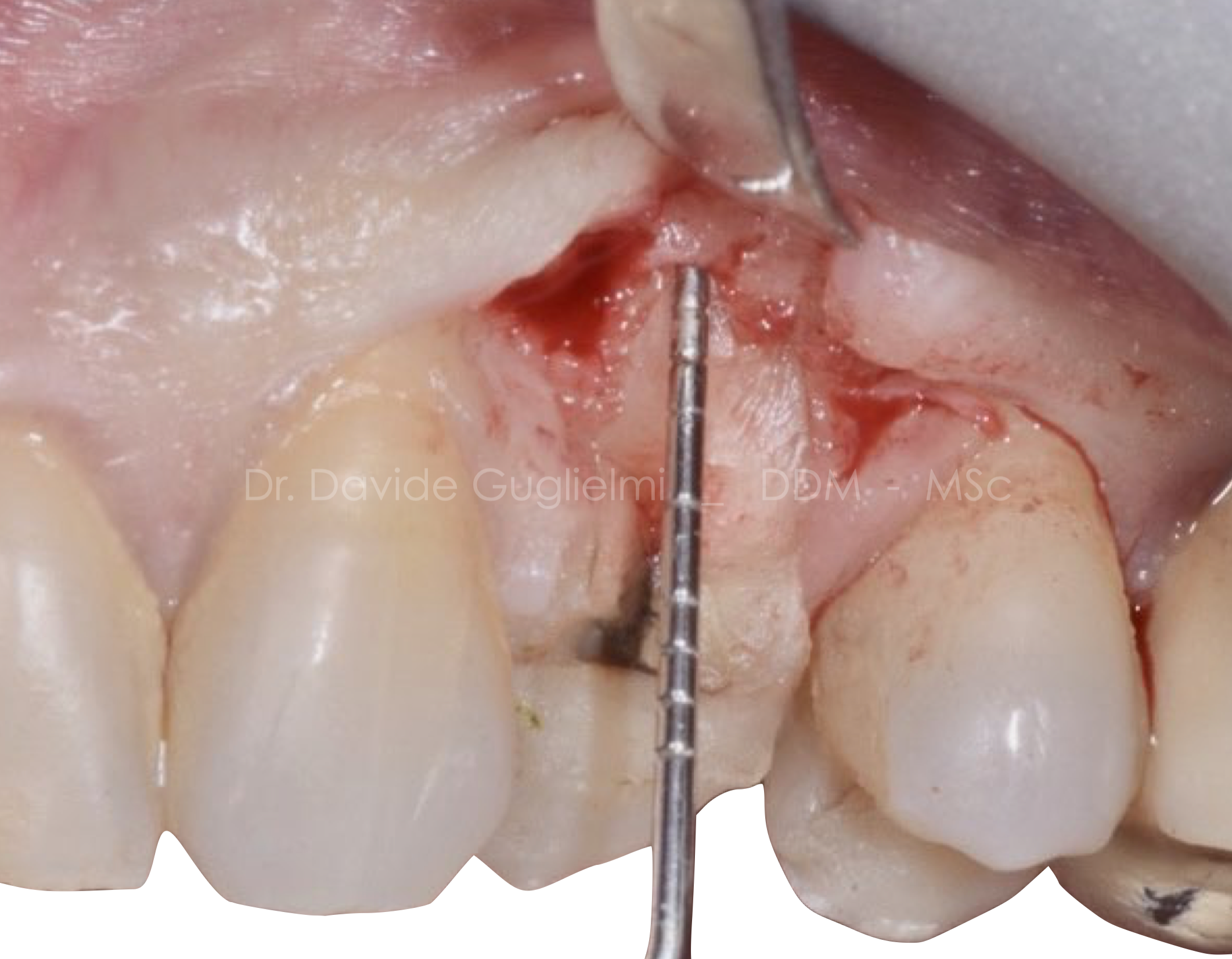
Fig. 5
Buccal view of the flap design and the flap elevation.
We perform here a split thickness incision of the anatomic papillae and a full thickness flap elevation apically to the sulcus.
The papillae is raised apico-coronally in order to preserve the vascular plexi (6).

Fig. 6
Once the surgical flap was raised, the rubber dam was positioned with a clamp (212 Hu-friedy) (5)
Before being positioned the dam was treated in order to reduce bacterial count with a mouth-wash containing 0,2% chlorexidine (Curaden - Curasept 0,20% + hyaluronic Acid)(2)

Fig. 7
The tooth has been isolated without suturing the underlying flap; a full isolated field was obtained by placing a liquid dam in the most cervical portion of the tooth.

Fig. 8
The decayed tissue was removed and a cavity access to the pulp chamber was performed using a diamond-coated bur.

Fig. 9
During the opening phase of the pulp chamber, an ultrasonic diamond-coated tip (ET18 Satelec) was used in order to avoid the complications given by the presence of pulp calcifications.

Fig. 10
Over time, the calcifications have become worse due to the neo-deposition of secondary dentine which, partially or completely, has deleted the anatomy of the pulp chamber.
In fig.10 you can see the orifices of the root canals: two buccal and the palatine ones.

Fig. 11
Different approaches may be considered when a non-adhesive final restoration is planned (for example, conventional crown).
In this case multiple walls are missing.
The so-called ‘doughnut’ technique involves a circumferential build-up of the cavity walls and use of a suitable barrier (cotton pellet, thermoplastic gutta-percha, PTFE, liquid dam) to prevent blockage of root canal orifices.)(9;3)

Fig. 12
In this case three sterilized paper points were used by inserting them into the root canals. The buccal aspect of the tooth was etched with Dentoetch, (37% ortho-phosphoric acid ) that was characterized by a perfect viscosity with provided quick and easy rinse (A).
The tooth is then dried with air and the paper points are substituted with dry ones. (B).
Ultimately primer (C) and bonding (D) (QuickBond, Itena Clinical) are applied as suggested by the manufacturer.

Fig. 13
Nano - filled composite dual cure material placement (Dentocore Body, Itena Clinical).
A recent study demonstrated that the hardness of this material is close to the dentine one.
Moreover this material has a low shrinkage rate, despite being a very fluid material, thia can be an advantage to avoid bubbles in the post cementation.

Fig. 14
The Dentocore is a dual curing Material.
It is suggested to cure this resin composite material for at least 40 seconds.

Fig. 15
After removing the rubber dam if liquid rubber dam is still present it can be polished with a Brownie SHOFU (CA 0403) and a Greenie SHOFU (CA 0404)

Fig. 16
The clinician must be careful not to leave the excess material (liquid dam) on the reconstructed CEJ (cement enamel junction).
With a lateral vision of the tooth it is possible to appreciate the integrity of the material polished and finished due to a correct emergency profile. (2)
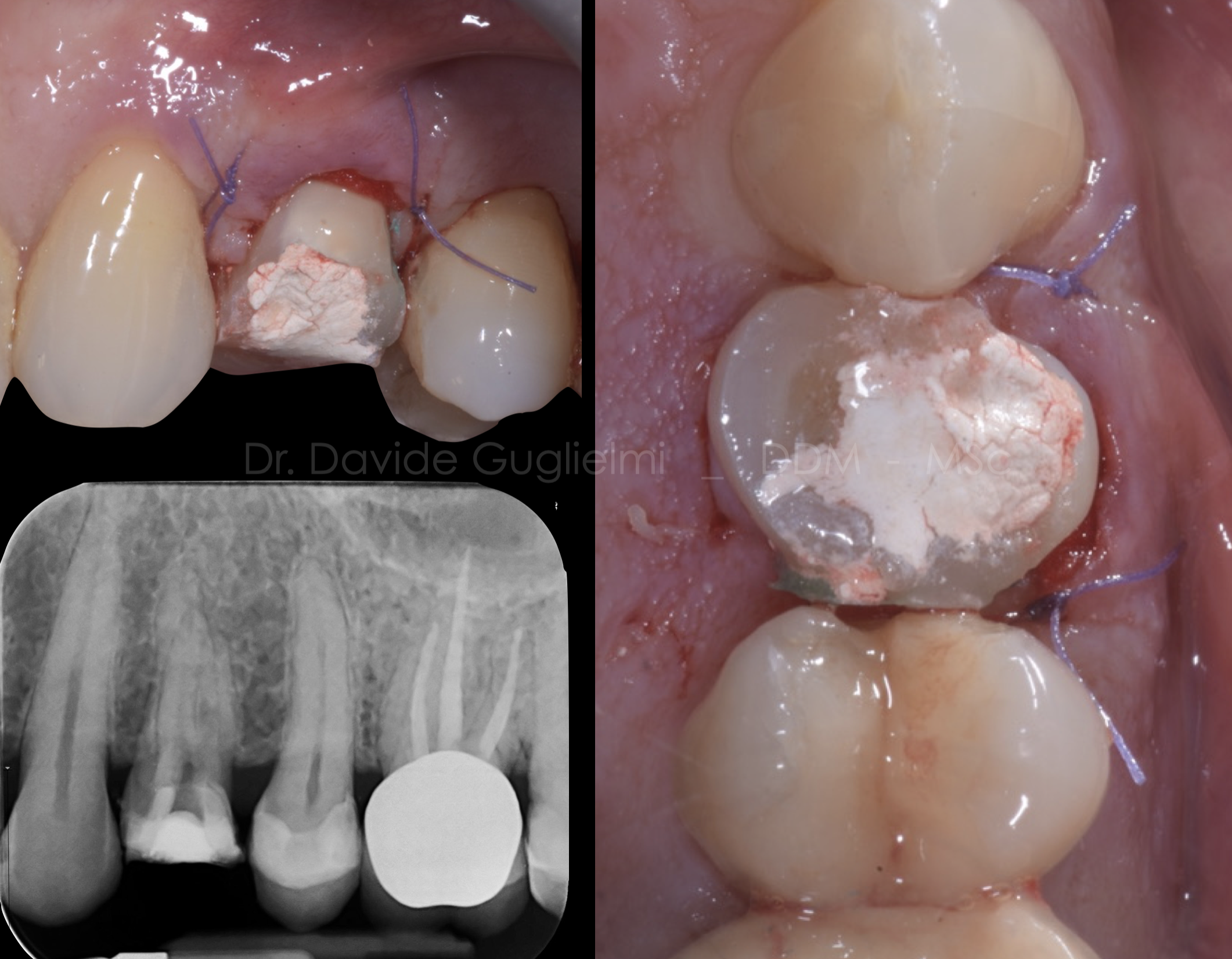
Fig. 17
A resorbible surgical suture, 5/0 (Vycril) has been used in order to avoid plaque accumulation in the days following the procedure. Two single stitches have been placed either on the mesial and distal papilla.
The sutures have been removed after two weeks from the surgery.
A: lateral view
B: occlusal view
C: periapical X-Ray

Fig. 18
2 months follow up
Conclusions
Based on author knowledge and experience, the Itena DentoClic products (Itena) seem to be safe and effective for pre-endodontic restorations as well as for those one in which restorative margins are sub-gingival (in respect of the specific dimension of the connective tissue attachment).
However high-quality clinical trials are needed.
Bibliography
Ercoli, C., & Caton, J. G. (2018). Dental prostheses and tooth-related factors. Journal of Clinical Periodontology, 45(5S), S207–S218. http://doi.org/10.1111/jcpe.12950
Guglielmi, D., & F. Gorni. (2019). Immediate Crown Replacement: a case report of extensive radicular fracture with intra-canal anchorage. Giornale Italiano Di Endodonzia, (33), 57–64. Gavriil, D., Kakka, A., Myers, P., & O Connor, C. J. (2021).
Pre-endodontic restoration of structurally compromised teeth: current concepts. Br Dent J, 231(6), 343–349. http://doi.org/10.1038/s41415-021-3467-0
Guidelines for the Management of Traumatic Dental Injuries: 1. Fractures and Luxations of Permanent Teeth. Pediatr Dent. 2017. Sep 15;39(6):401-411.
Tonini R. An Innovative Method for Fragment Reattachment after Complicated Crown Fracture. J Esthet Restor Dent. 2017 May 6;29(3):172-1
De Sanctis M, Clementini M. Flap approaches in plastic periodontal and implant surgery: crit- ical elements in design and execution. (2014). Journal of Clinical Periodontology. 2014. 41(s15), S108–S122.
Diangelis AJ, Andreasen JO, Ebeleseder KA, et al. International Association of Dental Traumatology guidelines for the manage- ment of traumatic dental injur- ies: 1. Fractures and luxations of permanent teeth. Dent Traumatol 2012;28:2-12.
Ferrari M, Koken S, Grandini S, Ferrari Cagidiaco E, Joda T, Discepoli N. Influence of cervical margin relocation (CMR) on periodontal health: 12-month results of a controlled trial. J Dent 2018; 69: 70–76.
Rao S, Ballal N V. Endodontic Buildups – A Case Series. J Dentists 2017; 5: 6–12.


