

Build up and onlay preparation of an endodontically treated tooth with QuickBond adhesive system and Dentocore core build up composite
10/04/2022
Federico Ceroni
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Rehabilitating endodontically treated teeth that have partially maintained coronal structure with overlay is nowadays the gold standard. Adhesive dentistry has changed the way we approach these cases: the goal is to maintain the coronal structure that has not been removed during caries removal and during root canal therapy.
Adhesives and composites have permitted more conservative protocols for repairing severely damaged teeth by reducing the invasiveness that was historically involved with the ‘’classic’’ prosthetic approach.
From the literature we know that an endodontically treated tooth that has lost a marginal ridge turns out to be a tooth that must be carefully analyzed to avoid a negative long-term prognosis. The loss of the interaxial dentin together with the marginal ridge leads to a weakening of the element which should not be underestimated. it will therefore be essential to evaluate the thickness of the cusp residues adjacent to the lost marginal ridge. If these thicknessess are less than 2.5 / 3 mm we will have to proceed with a cusp coverage.
Fig. 1
In this case this lower molar, once cleaned from the carious process and after the root canal therapy, results to have very thin cusps adjacent to the lost marginal ridge. After measuring with a thickness gauge the residual walls, I realized that it was less than the reference of 3mm. I therefore decided to perform an onlay that will cover these two cusps in order to protect them from chewing acts and avoid a possible fracture of the element over time
When we deal with adhesive rehabilitations such as overlays, it is essential to perform 2 procedures before taking the impression. The first procedure is immediate dentin sealing (IDS): this allows to seal the dentinal tubules just cleaned from the carious process and allows us to obtain higher adhesion values.
In this case the adhesive procedures was performed using the QuickBond SAM2 adhesive system, no orthophosporic acid was used.
First I applied 3 layers of A prime, lived undisturbed for 5 sec and then dried with a blast of air, then I applied 2 layers of B bond ,with his dual activator, also dried with a blast of air and cured for 20sec with a light-curing unit.
The second fundamental step is to perform a build up of the tooth before taking the impressions. The build up can be performed with a paste composite, a flowable or a dual curing composite.
A build up is necessary for a variety of reasons: first of all it allows to fill the undercuts of the cavity created once the caries has been removed. By filling the undercuts the onlay preparation will be less invasive, as we will not have to eliminate the undercuts to allow passive insertion of the onlay.
In addition, the execution of a build up allows us to standardize the thickness of the onlay that will be manufactured. With the build up, one will increase the thickness of the reconstruction in the areas where more structure has been lost, this will allow us to have an onlay with a uniform and controlled thickness.
In this case I decide to perform the build up with a dual curing composite (Dentocore, Itena ) because as the floor of the pulp chamber was very deep, I wanted to be sure that even the deepest areas of my reconstruction would polymerize. During the extrusion of the composite one should pay attention to always keep the tip of the syringe immersed in the cement, this will allow us not to create bubbles
Once the build up is complete it is time to prepare the dental element.
The first step consists in the preparation of the cusp residues with a diamond bur. The cusps are cut down, usually by 2/3mm: this allows to protect them and to prevent future fractures with the onlay cementation. Once the cusps have been prepared, it is time to prepare the occlusal aspect of the cavity. One must pay attention to eliminate any kind of undercuts, because the cavity design must allow a passive insertion of the onlay. Keep in mind that if you take a digital impression the margin of the preparation should be rounded.
It is useful to refine the preparation margin with a silicon bur.
When preparing the cavity for an adhesive rehabilitation it is not necessary to create retentive geometries, but we need only to cut-down the structures that have to be protected by the masticatory load and connect the various surfaces.
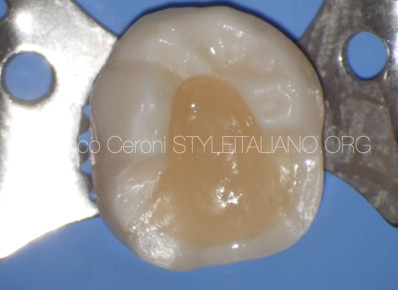
Fig. 2
The tooth after the preparation
Conclusions
Adhesive dentistry allows us to solve complex cases with a very conservative approach.
The analysis of the residual structures of the tooth will be fundamental in order to understand what the right treatment plan may be.
Presence of enamel, residual thickness of the cusps, quality of dentin, position and functional load are all details that must be carefully analyzed.Aalways remember that if we decide to perform an adhesive restoration we will have to be very precise in carrying out the adhesive maneuvers, respecting the times and steps, only in this way will we guarantee the success of our restoration.
Bibliography
1 Lopez LMP, Leitao JG, Douglas WH. Effect of a new resin inlay/ onlay restorative material of cuspal reinforcement. Quintessence Int 1991;22:641—5.
2 Morin D, Delong R, Douglas WH. Cusp reinforcement by the acid- etch technique. J Dent Res 1984;63:1075—8.
3Dietschi D. Spreafico R. Current clinical concepts for adhesive cementation of tooth-colored posteriors restorations. Pract Periodontics aesthet Dent 1998;10:47-54
4 Perdigao J. Dentin bonding as a function of dentin structure . Dent Clin North Am 2002;46:277-301
5 Dietschi D, Duc O, Krejci I, Sadan A. Biomechanical considerations for the restoration of endodontically treated teeth: a systematic review of the literature. Part II: evaluation of fatigue behavior, interfaces, and in vivo studies. Quintessence Int 2008;39:117—29.
6 Vanini L. Light and color in anterior composite restorations. Pract Periodontics Aesthet Dent. 1996 Sep;8(7):673-82

