MB3 in second maxillary molar
28/10/2023
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
The prevalence of MB2 canal has been widely discussed, and it is now considered to be a frequent occurrence.
A third MB canal in upper first and second molars is still considered a rare anatomical variation. This case presentation describes the instrumentation , irrigation and obturation of a maxillary second molar with 3 mesio buccal canals.

Fig. 1
Patient, male, in his late 40’s, was referred to our clinic for endodontic assessment and treatment of his upper right second molar.
The patient complained of the fact that the UR7 (17) has fractured and was painful for a while. His general dentist dressed the tooth and the pain settled.
Upon examination the UR7 was restored with glass ionomer restoration. The tooth was not tender to percussion, there were no deep periodontal pocketing and no mobility. The UR7 was non-responsive to cold testing.
Periapical radiograph shows a deep restoration present and no periapical radiolucency.
A diagnosis of pulp necrosis was placed, and treatment options were presented to the patient- do nothing, extraction or root canal treatment. The patient decided to have root canal treatment done.

Fig. 2
After adequate local anaesthesia and rubber dam placement, the UR7 was accessed, and 4 canals were located.
In between the MB1 and MB2 there was a groove, as seen in the photo.
I decided to explore the groove with a 10 and 08 K files. An entire canal was discovered, that was connected apically to the other canals.
All canals were instrumented using rotary files.
The irrigation protocol consisted of copious 5.25% sodium hypochlorite and 17% EDTA. Passive sonic activation was used in order to activate the irrigation solution.
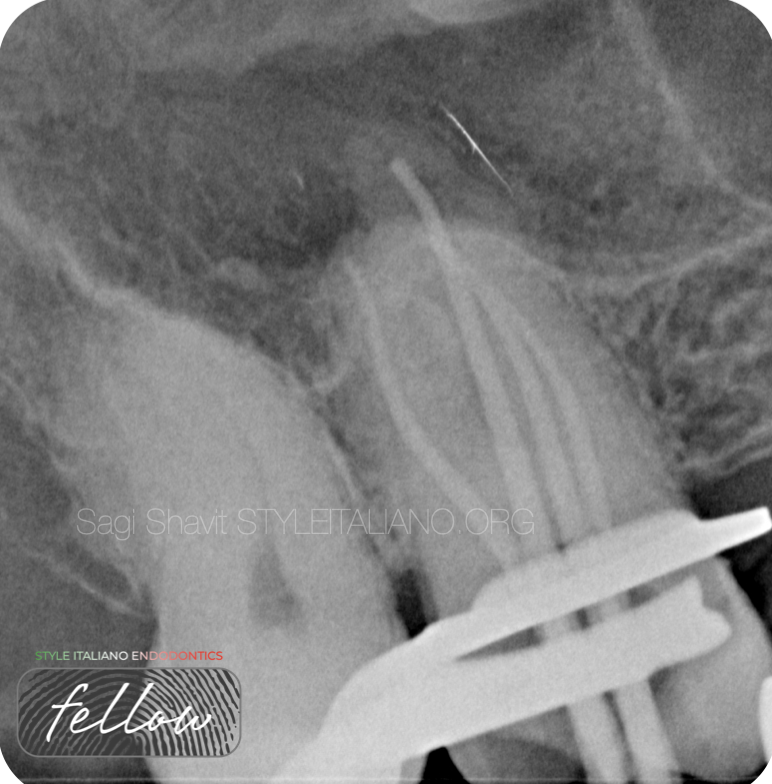
Fig. 3
An intra-operative radiograph with GP points shows that the canals are indeed merged apically.
The canal were obturated with bioceramic sealer in a single cone technique, as seen in the video.

Fig. 4
The Post operative radiograph and photo shows adequate obturation of the root canal systems.

Fig. 5
About the author:
Sagi Shavit
Graduated as DMD Bucharest 2009 - UMF “Carol Davila” Bucharest, Romania
MSc in Endodontology - Chester University
PG diploma in implantology - City of London Dental School
Conclusions
Missed anatomy is one of the main reasons for endodontic failure. Leaving uncleaned canals means leaving bacteria behind.
One of the most notorious missed canals is the elusive MB2, which is present in up to 90% of upper first molars, and 40% of upper second molars.
MB3 is a rare clinical finding, especially in the second molars, but it is important, nevertheless.
Keeping in mind the possibility of their presence, clinicians should explore every groove to try and locate them.
Bibliography
- Ordinola-Zapata, R., Martins, J. N. R., Plascencia, H., Versiani, M. A., & Bramante, C. M. (2020). The MB3 canal in maxillary molars: a micro-CT study. Clinical oral investigations, 24(11), 4109–4121. https://doi.org/10.1007/s00784-020-03284-7.
- Tabassum, S., & Khan, F. R. (2016). Failure of endodontic treatment: The usual suspects. European journal of dentistry, 10(1), 144–147. https://doi.org/10.4103/1305-7456.175682.