Confluent Canal Management
12/05/2017
Calogero Bugea
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
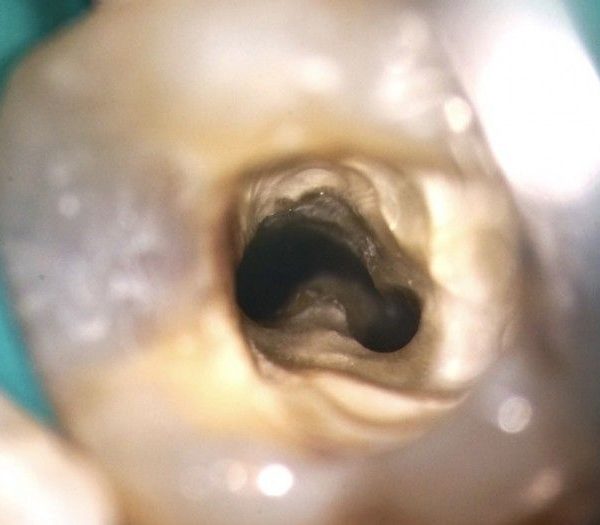
The comprehension of the anatomy of the root canal system is an important factor when using rotary nickel titanium instruments. One of the main risks in rotary instrumentation is the occurrence of instrument fracture: it is widely acknowledged that a cause for fracture is the introduction of a rotary instrument in the meeting area of two canals that merge one into another.

Fig. 1
Weine classified merging canals into 4 types, depending on the configuration of the main root canal of a tooth along its course, from the floor of the pulp chamber to the apex. This classification may be very practical to use in our daily practice when we have to treat two canals into one root

Fig. 2
TYPE 1: one orifice, one root canal, one apical foramen

Fig. 3
TYPE 2: two orifices, two root canals, one apical forame

Fig. 4
TYPE 3: two orifices, two root canals, two apical foramin

Fig. 5
Type 4: one orifice, two root canals, two apical foramina. In types 1 and 3 the existing canals can be cleaned and shaped separately, as if they were in different roots. Due to the complexity of the anatomy, in all situations in which we treat canals with possible confluences, we have to treat each root separately and not together, to prevent over-instrumentation and transportation of the apical foramen, which could occur as a result of cleaning and shaping it twice from two different directions. For example, the mesio-vestibular lower molar canal in a 50% of cases sharing an apex with the mesio-lingual canal. This canal can be enlarged less with less risk of weakening the root and stripping. In type 2 configuration, which is easy to diagnose early, great care must be taken during the cleaning and shaping and the packing procedures. Type 4 is very difficult to diagnose, but every time that we suspect of having this configuration, we could use some some expedients. The early diagnosis of a common apex will also prevent the risk of instrument fracture. Let’s see when it is advisable to really get smart about type 4 configuration diagnosis:
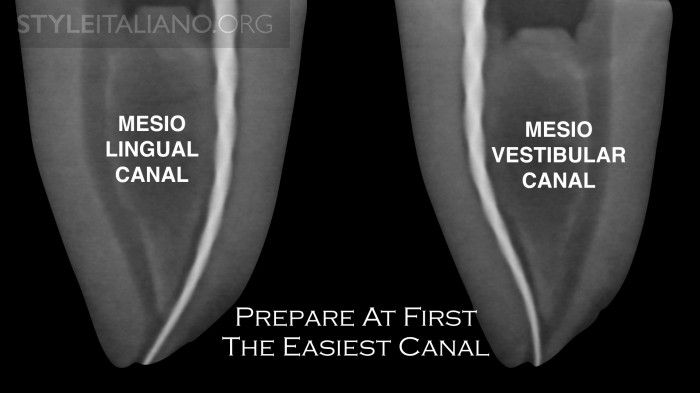
Fig. 6
In general in lower molars the mesio-lingual canal, as it is usually straighter than the vestibular one; for the same reason in upper molars the mesio-buccal canal instead to the mesio-buccal 2 canal. These canals are more centered within the root.

Fig. 7
This image shows a typical apical transportation that occurs when the merging is located in the more apical part or the canals, so shaping from two different directions will create a drop-shaped foramen and parallel walls. Early diagnosis can be done by different methods in different steps of an endodontic treatment. With traditional intra-oral Rx there is no possibility of understanding the anatomical configuration of a tooth. Sometimes patients listed for endodontic treatment might already have a CB-CT scan available (for previous treatments such as implant positioning or wisdom tooth extraction). In these cases clinicians have the possibility to visualize the anatomy prior to performing the treatment.

Fig. 8
Of course the above mentioned scenario is common, but not as much as we wished it was. So, the best method in the Author’s opinion is the visualization of the confluence with a gutta-percha cone. When the probably confluent canal, let’s say of a lower molar, is ready to receive a small-sized instrument to determine the working length, introduce a gutta percha cone in the already prepared (e.g. mesio-lingual) canal and then a small file(e.g. #10 K-file) in the mesio-buccal canal to measure its length. The file is used with short movements and it is possible to check whether the cone placed in the prepared canal is being displaced.

Fig. 9
The the K-file is then withdrawn from the canal, followed by the gutta-percha cone which should be carefully examined, preferably with a magnifying lens, to search for any grooves, scratches, or folds left by the non-invasive instrumentation of the mesio-buccal canal. This method is very efficient, as it only requires a few minutes to investigate the presence of other canal.

Fig. 10
On the other hand, this method can fail in case of apical confluence or in all the situations in witch the K-file on the confluent canal is somehow unable to scratch the master cone.

Fig. 11
Another method requires the use of an electronic apex locator (EAL). After the first canal has been prepared, the operator checks the working length of the second canal with the use of the EAL. Then repeat the operation leaving the last apical file inserted in the prepared canal at the foramen. If the working length of the second canal this time appears to be shorter by several millimeters, this would indicate that the second canal is sharing the foramen with the first one and the communication is at the same distance from the common foramen. This method can be affected by the presence of irrigants or closed canals. Some clinicians, especially those who only use thermafil obturation system, prefer this method because it is easy and doesn’t require the use of gutta-percha cones. In case of particular anatomies, e.g. the first bicuspid that often has type 3 configuration, the endodontist can evaluate the confluence during simultaneous cone/Thermafil carrier insertion. As it happens in the case of cone Rx-check or of Thermafil during carrier selection.

Fig. 12
Individually, the cones/carrier advance unhindered to the desired maximal depth.
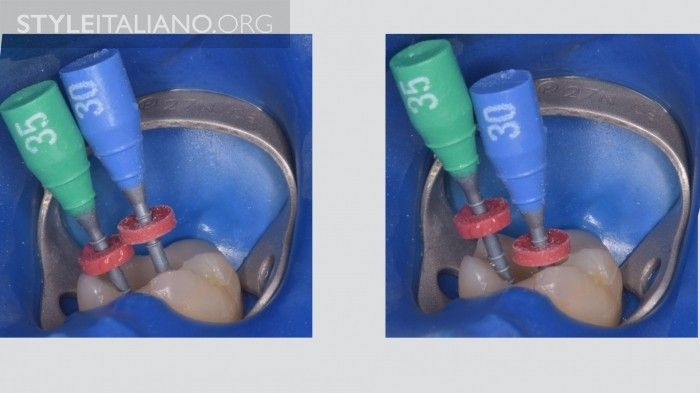
Fig. 13
When they are placed simultaneously in the various canals, they only advance alternately; for example, in a lower molar, if the buccal goes to working length, the lingual stays shorter and viceversa. The same check may be made with a Thermafil carrier, with the same results.

Fig. 14
During irrigation, in order to avoid vapor lock and to change frequently the solution, aspiration of the irrigant solution is recommended. In this manner, when the tip of the needle overtakes the confluence, the solution will be drained from the two canals in the same moment. Aspiration can be done with a normal syringe or by Endovac. This check is advisable to be done, not only to confirm the confluence, but to clean the confluence area that is clear and untouched by rotary instruments.
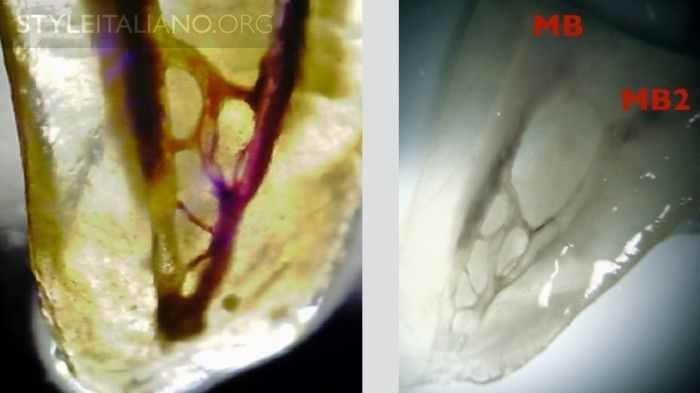
Fig. 15
This image shows a lot of communications between the two canals: this area is "untouched” by rotary instruments, and only an efficient irrigation protocol can clean it and thoroughly disinfect it. Diaphanizations by Dr. A. Iandolo (Italy).

Fig. 16
Even in case of multiple canals, the rules about identification, shaping, cleaning and obturation are the same that other configurations.
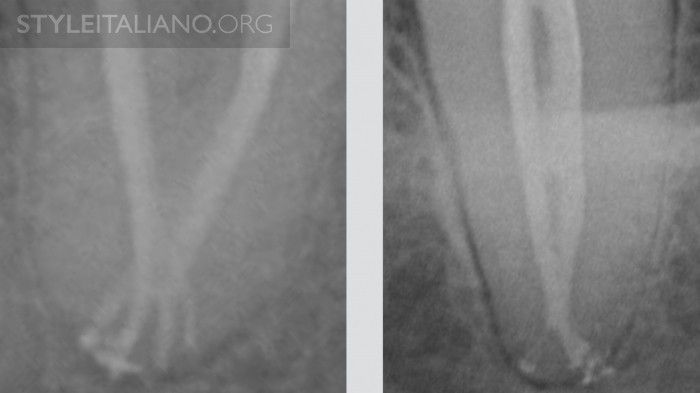
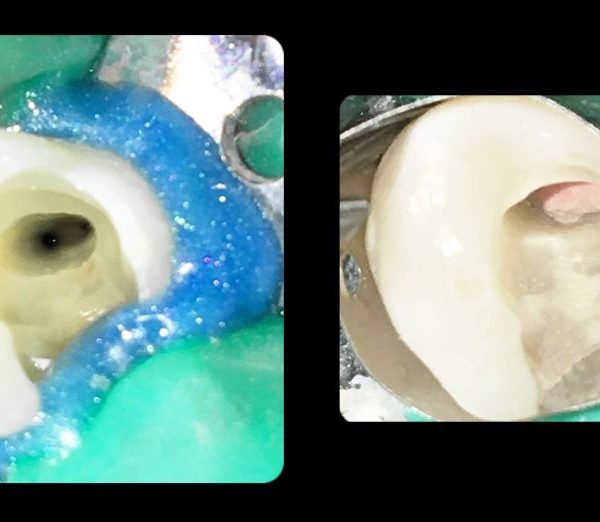
Fig. 17
Confluences may hide a particular anatomy, for this reason it's important, after carrying out the cleaning protocol, to obturate in a 3D manner this kind of anatomy. During obturation of these of roots, it is advisable to place gutta-percha cones with sealer simultaneously and then pack each; in case of carrier based obturation, place a plastic carrier to block the passage of the gutta-percha from the other canal and then obturate the confluent canal with your favorite method.
Conclusions
It is very important to understand the anatomy and to respect the root canal configuration in order not to transport the foramen, not to strip and weaken the root, and not to fracture an endodontic instrument.
Early diagnosis is the solution to face this kind of situations in a safe, predictable way.
Bibliography
Weine FS, Healey HJ, Gerstein H, Evanson L. Canal configuration in the mesiobuccal root of the maxillary first molar and its endodontic significance.Oral Surg Oral Med Oral Pathol. 1969 Sep;28(3):419-25.
Weine FS.Initiating endodontic therapy in posterior teeth. Part II. Maxillary molars. Compend Contin Educ Dent. 1982 Nov-Dec;3(6):455-64.
Berutti E.Respecting apical foramina in the endodontic treatment of confluent canals. G Endodonzia. 1990;4(1):6-21.
Hess W, Zürcher E. The anatomy of the root canals of the teeth of the permanent and deciduous dentitions, New York: William Wood & Co, 1925.
Burns RC, Buchanan LS. Tooth Morphology and Access Openings. In Cohen S, Burns RC, editors: Pathways of the Pulp, 6th ed., Mosby Yearbook Co., 1994.
Ruddle CJ.The Mesial-Buccal Root of the Maxillary First Molar: Treatment Considerations, The Endodontic Report, Fall/Winter, 1986.
Ruddle JC.Endodontic Canal Preparation : Breakthrough cleaning and shaping strategies , Dentistry Today, February 1994