How To Manage A Ledge - A case report
25/09/2023
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Among all the difficulties we encounter during the reconstruction of an incongruous root canal therapy, a very difficult challenge is always represented by overcoming false paths and ledges mistakenly created during the primary treatment(1).
A 26-year-old patient comes to my attention due to a fracture at element 4.7. The patient reports recurrent episodes of pain when chewing in the indicated area. The objective examination immediately reveals signs of inflammation which manifest themselves with strong tenderness upon percussion of the element, carious infiltration of most of the previous restoration and a favorable fracture of the enamel and subgingival and supracrestal dentin. The radiographic examination confirms the previous diagnostic questions and shows inadequate previous root canal therapy in terms of vertical and three-dimensional filling. Apical lesions of both roots are also noted. The perimeter probing of the tooth does not reveal root fractures.
First of all, therefore, we proceed with the removal of the old adhesive restoration and with the cleaning of the carious lesion and, before starting to retreat the tooth, to be sure of the restorability of the element, we proceed with the relocation of the lingual margin(2).
Then we proceed with the disassembling of the chamber portion and, once the canal entrances have been located, we begin to empty the previous filling. This delicate maneuver is tackled easily thanks to 25/06 files and the use of the reciprocation system(3).
Having failed to obtain patency of the distal canal system and given the little time available due to emergency management, the chamber portion is temporarily closed with photopolymerizable PMMA material (radiolucent).
During the second appointment, manually probing the distal canal, I immediately realized the presence of an iatrogenic ledge near a sharp distal curvature typical of this root. I decide to pre-curve k-files of progressive diameters to overcome the obstacle and engage the canal by manually instrumenting it with a delicate "watch winding" movement up to an adequate diameter (30).
The finishing of the mesial canals, once their confluence was proven, was carried out using 30/06.
5.25% NaCl was used throughout therapy to facilitate chemical disinfection and removal of debris. Before obturation, the hypochlorite was activated with ultrasonic tips and, once cleansing was completed, we proceeded with equally activated 17% EDTA washes to remove the smear layer(4).
The obturation technique used to fill the mesial canals was warm vertical
condensation, while the distal canal, since the cone test was not repeatable due to the step, was obturated with the “Squirting Technique”(5).
The case was finalized with a composite overlay.

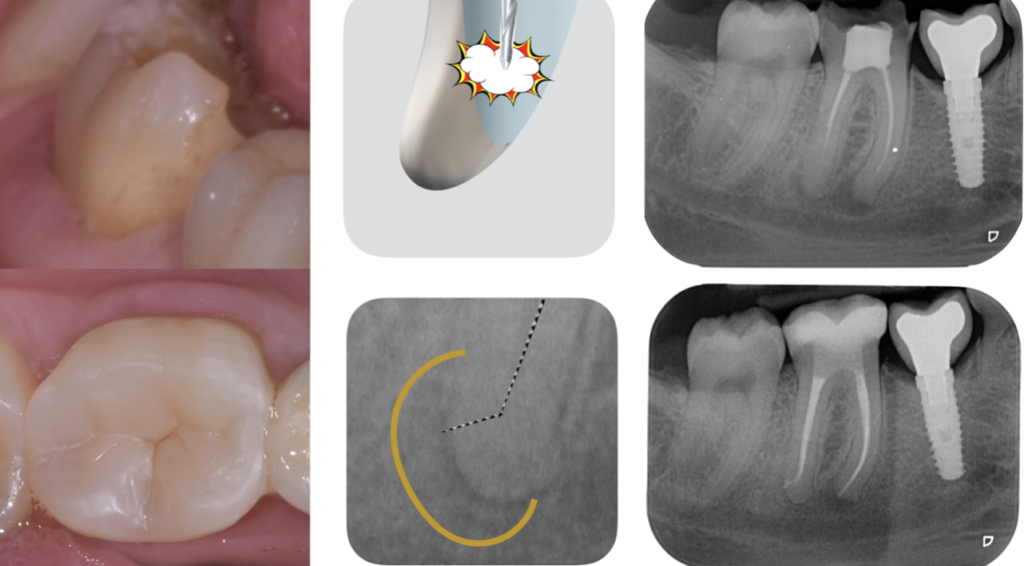
Fig. 1
Clinical View and Preoperative Xray

Fig. 2
Preoperative Xray and After Disassembling Xray
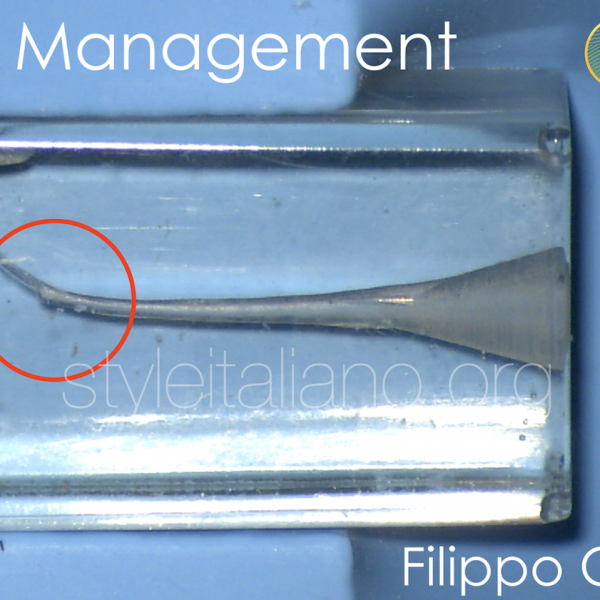
Fig. 3
Formation of the ledge in front of a sharp curve and how to pass it folding a k File

Fig. 4
K file progression
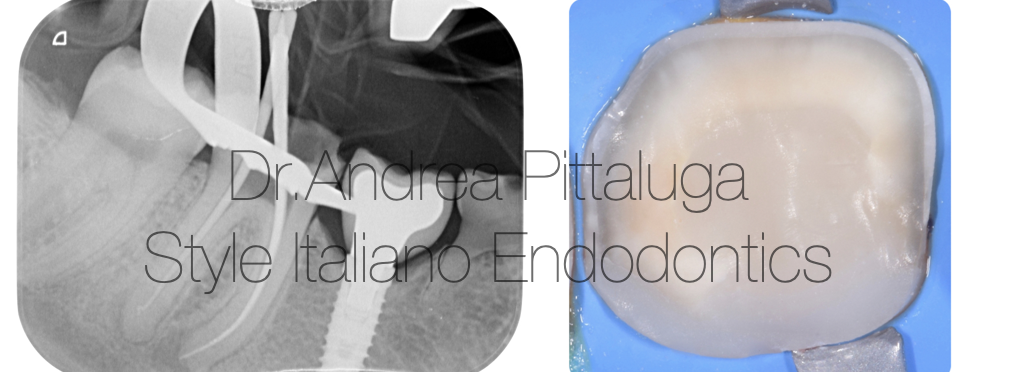
Fig. 5
Working length and Build Up

Fig. 6
Overlay Bonding

Fig. 7
Final Result

Fig. 8
Dr. Andrea Pittaluga, graduated in 2015 from the Alfonso X El Sabio University in Villanueva de la
Canada (Madrid) with the thesis "Anatomical and surgical revision of the sinus lift".
In 2016 he began working in dental practices in Milan and its province and attended postgraduate
courses with the best Italian professionals and speakers. Among these, the names of Dr. Federico
Ferraris, Dr. Stefano Gracis, Dr. Prof. Fabio Gorni and Dr. Prof. Tiziano Testori stand out.
From 2017 to 2018 he attended the Oral Surgery department of San Raffaele directed by Prof.
Raffaele Vinci (rector Dr. Prof. E. Gherlone).
Starting from 2019, he carries out tutoring activities in the post-graduate courses of Dr. Prof. Fabio
Gorni in orthograde, microscopic and surgical clinical endodontics. In the same period he was the
director of the dentistry department of the Auxological Institute of Milan.
Speaker in Italy and abroad, "Lecturer" at the Lake Como Institute, Fellow Member of Styleitaliano
Endodontic, Co-Author of the book "Tooth or Implant? The recovery or replacement of heavily
compromised natural teeth” by Edra (2023).
He currently dedicates himself exclusively to private practice, working as a specialist in
microscopic endodontics in the private practice of Dr. M. Imelio, as a specialist in conservative
dentistry, endodontics and prosthetics in the practice of Dr. Prof. Tiziano Testori and in his private
practice located in Sesto San Giovanni.
Conclusions
Ledges represent a very common obstacle in retreatment and are often difficult to manage: a reasoned approach and knowledge of the canal anatomy represent the key to success in this type of cases
Bibliography
1.Ledge formation: review of a great challenge in endodontics
Hamid Jafarzadeh et al. J Endod. 2007 Oct.
J Endod. 2007 Oct;33(10):1155-62.
doi: 10.1016/j.joen.2007.07.015. Epub 2007 Sep 4.
2.Cervical margin relocation in indirect adhesive restorations: A literature review
Jelena Juloski et al. J Prosthodont Res. 2018 Jul.
J Prosthodont Res. 2018 Jul;62(3):273-280.
doi: 10.1016/j.jpor.2017.09.005. Epub 2017 Nov 15.
3.Effectiveness of reciprocating and rotary retreatment files in the removal of endodontic filling material
Érica Reginato Cardoso et al. Gen Dent. 2022 Jan-Feb.
Gen Dent. 2022 Jan-Feb;70(1):22-25.
4.Irrigation in endodontics
M Haapasalo et al. Br Dent J. 2014 Mar.
Br Dent J. 2014 Mar;216(6):299-303.
doi: 10.1038/sj.bdj.2014.204.
5.A comparison of thermoplastic obturation techniques: adaptation to the canal walls
R N Weller et al. J Endod. 1997 Nov.
J Endod. 1997 Nov;23(11):703-6.
doi: 10.1016/S0099-2399(97)80406-2.