Decision making in retreatments, episode 1
12/10/2023
Abdullah AboHalima
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Retreatment isn't about creating longer or better looking white lines , it's about understanding causes of failure and how to overcome them, Usually the cause of failure is due to not abiding to the following parameters such as proper diagnosis including preoperative periapical radigraphs, isolation of the field, full chemo-mechanical preparation of the canals and three-dimensional obturation of the root canals.
There are two critical factors to develop a solid protocol for retreatments are decision makinG and treatment sequence.
Pointing out the main cause of pain and failure is our primary goal to be “patient centered” to relief the patients symptoms and to do that determining the actual cause is the objective.
In this article we have a tooth that was treated three times previously and referred to remove the broken instrument assuming that it's the cause of pain while actually it was not the causative factor of pain as it was multifactorial including poor disinfection, missed anatomy and aggressive apical violation.
therefore our treatment sequence started with the complete disinfection first then removing the file and taking the decision to seal the apex with MTA apical plugs rather than the conventional technique.

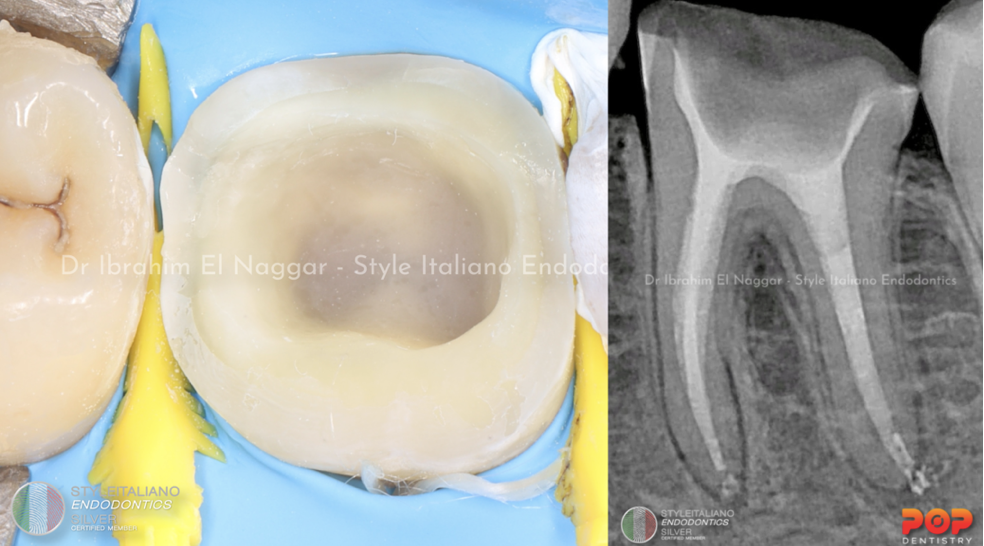
Fig. 1
Referred case with Symptomatic Apical Periodontitis (SAP) with Missed anatomy, Separated file, Heavily infected anatomy, Very wide apex "Violation of the apex”
We have to know the exact cause of failure before we start to minimize the pain at the first visit, is it from the Separated file as the patient told me ?
It’s obvious that This case shows aggressive shaping with violated apex and obdurated with large taper single cone
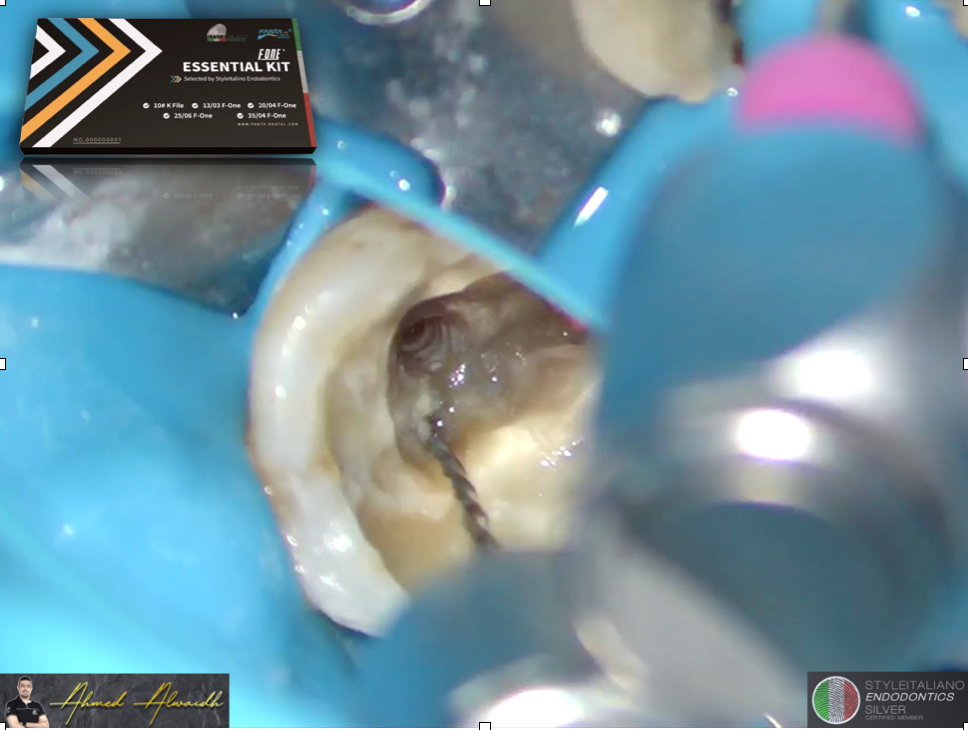
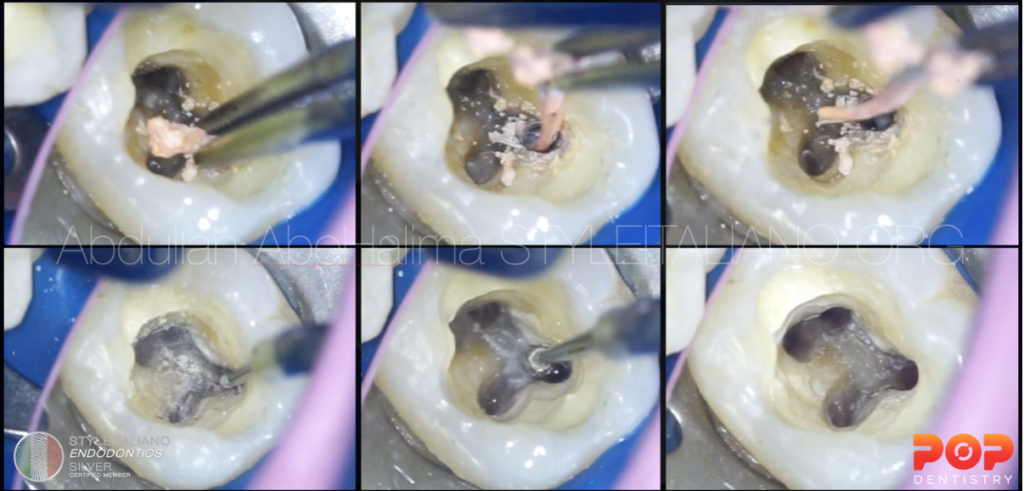
Starting with access modification in order to get straight line access to all the canals, removal of poorly sealed GP “single cone”, using dynamic files to remove all the remaining GP on the walls , then adequate disinfection to all the canals
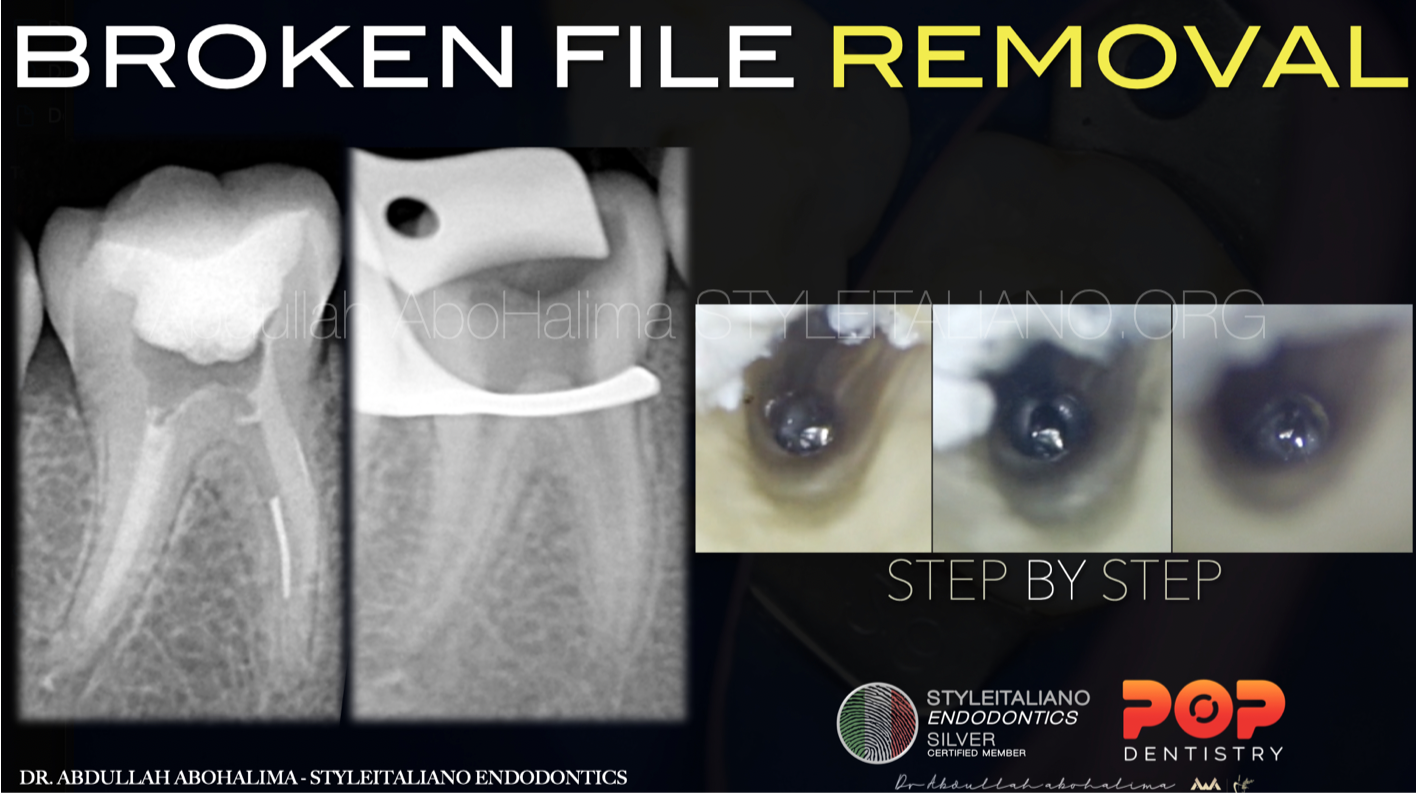
Fig. 2
Separated file removal using US tip, in next articles we will discuss all steps of separated files management in details .

Fig. 3
We all know that in retreatment all steps are important but here this is the most crucial step “APICAL SEAL”
according to aggressive violation of the apex we found that the apical foramen was larger than file 70 ISO during the apical gauging step to select a perfect master cone
When it comes to sealing ability in a large foramen MTA is evidently proved to be the best choice in terms of sealing and histological tolerance
MTA apical plug using customized GP as a plugger.
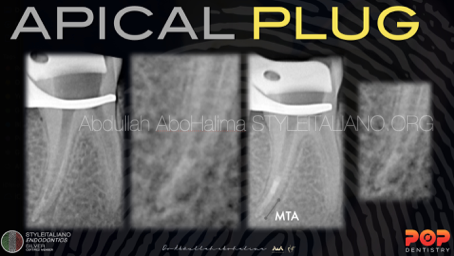
Fig. 4
MTA apical placement
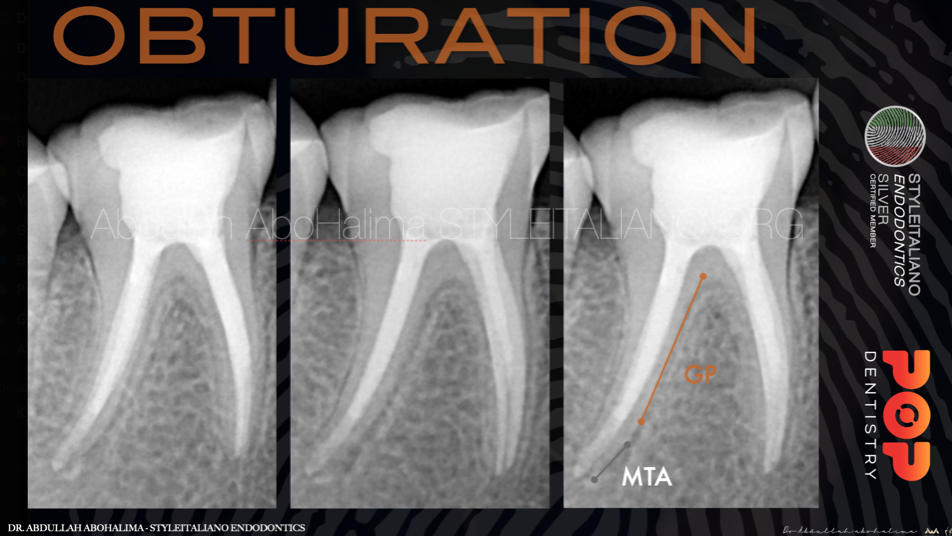
Fig. 5
Back filling using thermoplasticized GP
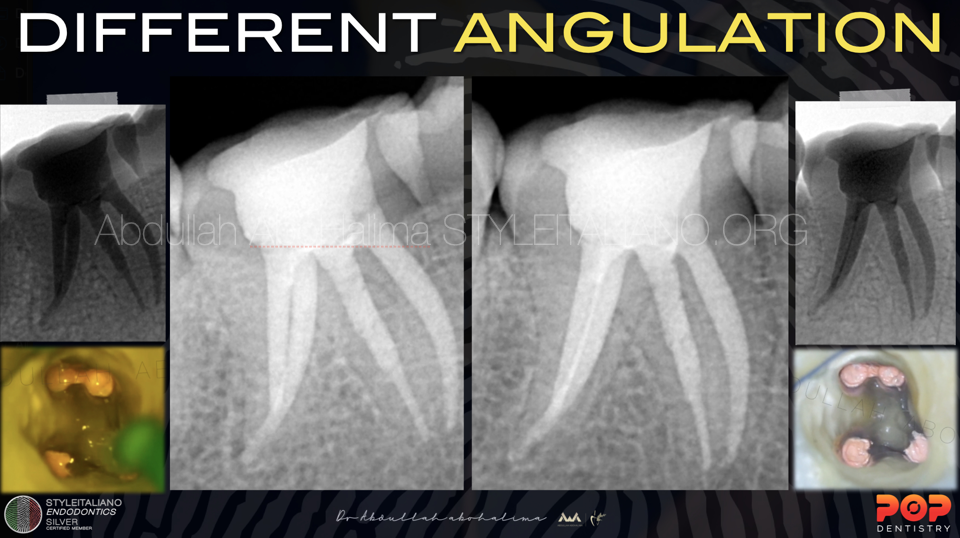
Fig. 6
Shifted X-ray showing perfect apical seal to all the canals followed by immediate coronal seal.
Conclusions
in conclusion, a Precise Decision making is built on Proper diagnosis from the beginning to assess the main cause of failure with a proper treatment sequence to achieve the highest level of success
Bibliography
1- Schilder H. Filling root canals in three dimensions. Dent Clin North Am. 1967; : 723-74Reit C. Grondahl H.G. Management of periapical lesions in endodontically treated teeth:ùstudy on clinical decision making. Swed Dent J. 1984; 8: 1-7
2-Endodontic Facts, American Association of Endodontists. Available at: http://www. aae.org/about-aae/news-room/endodontic-facts.aspx. Accessed June 1, 2015.
3-Bergenholtz G. Assessment of treatment failure in endodontic therapy. Journal of oral rehabilitation.
4-Farzaneh, M., Abitbol, S. & Friedman, S. 2004, Treatment Outcome in Endodontics: The Toronto Study. Phases I and II: Orthograde Retreatment;