Retreatment and modern post endo resto
07/09/2023
Ibrahim El Naggar
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
In this article i am highlighting the way i’ve dealt with this syptomatic lower 1st molar from the Retreatment to the final Restoration.
Lack of knowledge in the endodontic field may lead to some errors during the treatment if we are not having the right techniques combined with the right tools and it is so important to to save the tooth to the last chapter by providing a good, functional and durable restoration.

Fig. 1
Pre - Op Radiograph , showing a lower 1st molar with a GP that is reaching the WL with lesion on both roots after old treatment.

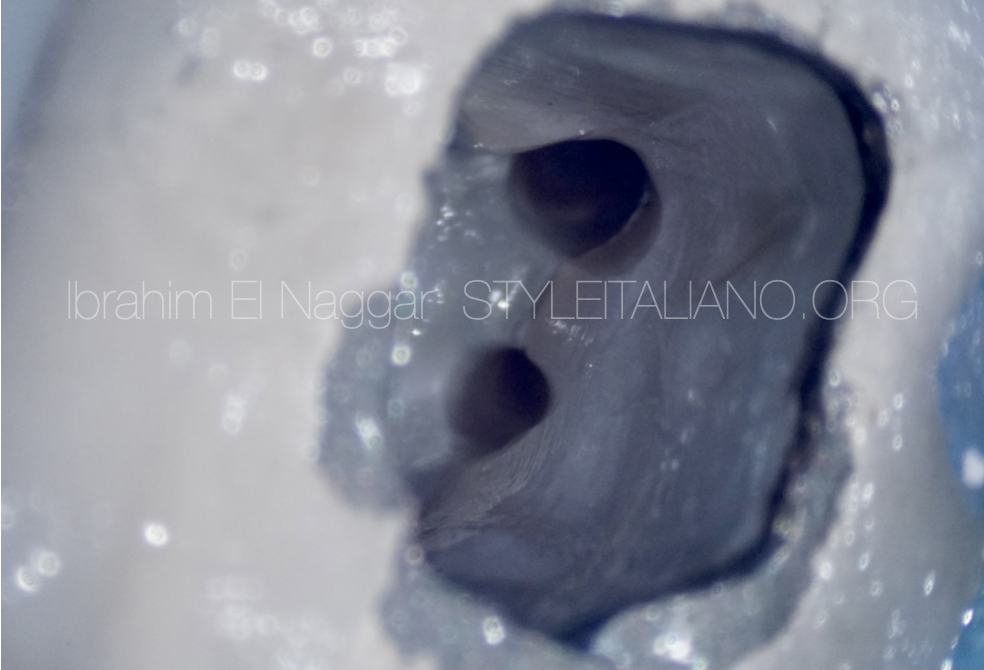
Fig. 2
The first line of the treatment was to remove any filling inside the canal, followed by the placement of an intra - canal medication to raise the pH inside, since the root canal was still wet.

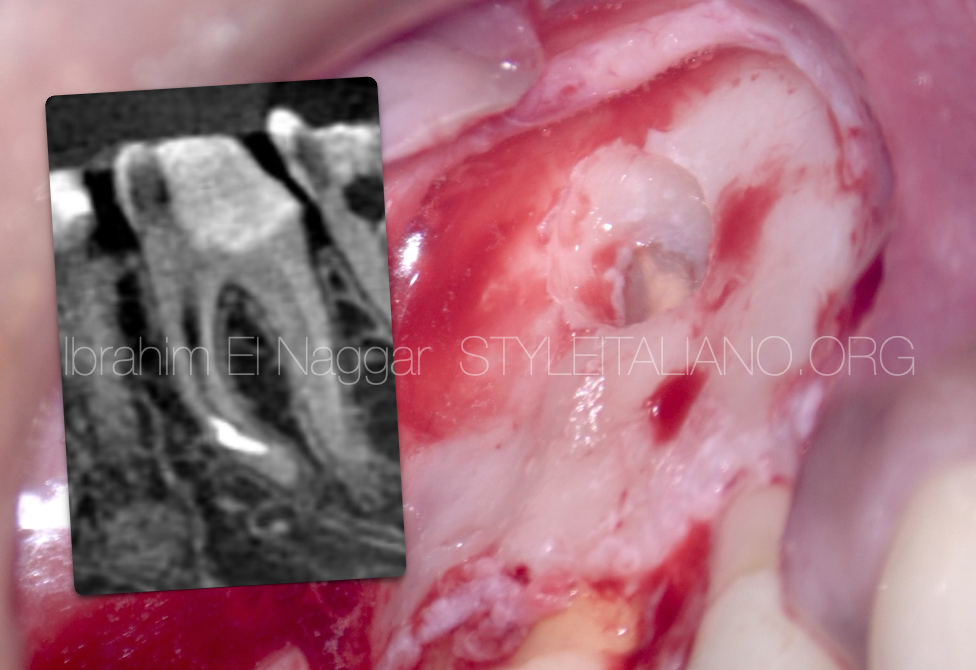
Fig. 3
The patient left for 3 months and didn’t show up. When she came back and we took an X-ray , we found that a lesion healed after long term placement of the medication.

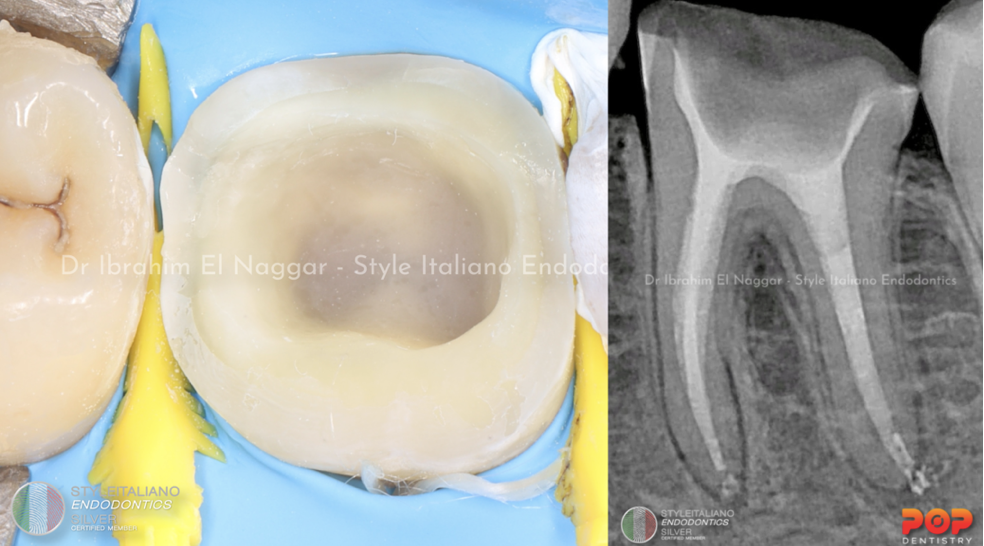
Fig. 4
Both mesial and distal canals were filled with squirting technique

Fig. 5
IDS, “IMMEDIATE DENTIN SEALING’ was done immediately after the obturation in conjunction with the overlay preparation.

Fig. 6
Picture of the preparation with IDS and multiple isolation

Fig. 7
Overlay cementation

Fig. 8
Overlay cementation
Conclusions
The clinician must have enough knowledge about the root canal anatomy, techniques and to know how to deal with errors if happened as well to provide the patient with a good, sealed long term restoration.
Bibliography
1. Endodontic Facts, American Association of Endodontists. Available at: http://www. aae.org/about-aae/news-room/endodontic-facts.aspx. Accessed June 1, 2015.
2. Borges AH, Bandeca MC, Tonetto MR, et al. Portland cement use in dental root perforations: a long term followup. Case Rep Dent 2014;2014:637693.
3. TsesisI,FussZV.Diagnosisandtreatmentofaccidentalrootperforations.Endodontic Topics 2006;13:95–107.
4. Tsesis I, Rosenberg E, Faivishevsky V, et al. Prevalence and associated periodontal status of teeth with root perforation: a retrospective study of 2,002 patients’ medical records. J Endod 2010;36:797–800.
5. Gorni FG, Gagliani MM. The outcome of endodontic retreatment: a 2-yr follow-up. J Endod 2004;30:1–4.
6. Clauder T, Shin S-J. Repair of perforations with MTA: clinical applications and mechanisms of action. Endodontic Topics 2006;15:32–55.
7. Kvinnsland I, Oswald RJ, Halse A, Gronningsaeter AG. A clinical and roentgenological study of 55 cases of root perforation. Int Endod J 1989;22:75–84.