Retreatment of a central incisor with Essential Kit
15/02/2023
Francesca Cerutti
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Aim of endodontic therapy is to maintain or restore the periapical health of teeth through shaping, cleaning and filling tridimensionally the root canal system. Root canal treatment has proven to be a predictable procedure with a high success rate.
Nevertheless, failures occur in 14-16% of primary endodontic treatments and retreatments account for approximately 30% of the demand for endodontists. The presence of clinical symptoms, non-healing or progression of periapical radiolucency and signs of resorption are parameters that lean towards endodontic failure. Moreover, poor technical quality of previous endodontic procedures and loss of coronal sealing are considered when making decisions on endodontic retreatment.
A German CBCT study reported that, among failed teeth, one third presented root fillings that were more than 2 mm short from the apex. This finding is in accordance with the definition of satisfactory root canal filling as a well-condensed material along a working length of 0 to 2 mm from the radiographic apex.
Within this context, persistent microbial infection is one of the major causes of failure.
In case of periapical lesion one might choose between retreatment and micro endodontic surgery taking into account the clinical situation, but also the patient general health and preferences.
A case will be shown in which, due to the necessity of a prosthetic rehabilitation of a tooth with a poor endodontic treatment, it was decided to perform a non surgical retreatment as a first step.

Fig. 1
A young patient that had a central incisor fracture due to a trauma eight years ago came to our clinic complaining about a chipping of the ceramic veneer.

Fig. 2
The intraoral examination shows the cervical and buccal chipping of the veneer

Fig. 3
The tooth 1.1 also results longer than the other incisor
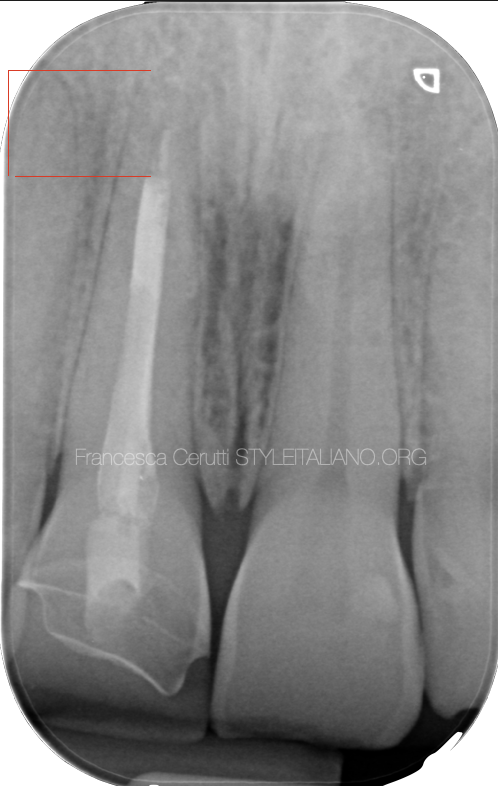
Fig. 4
The pre operative X-ray shows an incorrect root canal therapy, with a large preparation that abruptly stops 3 mm short from the apex.
Considering the need to rehabilitate the tooth with a crown, it was decided to retreat the tooth as a first step.
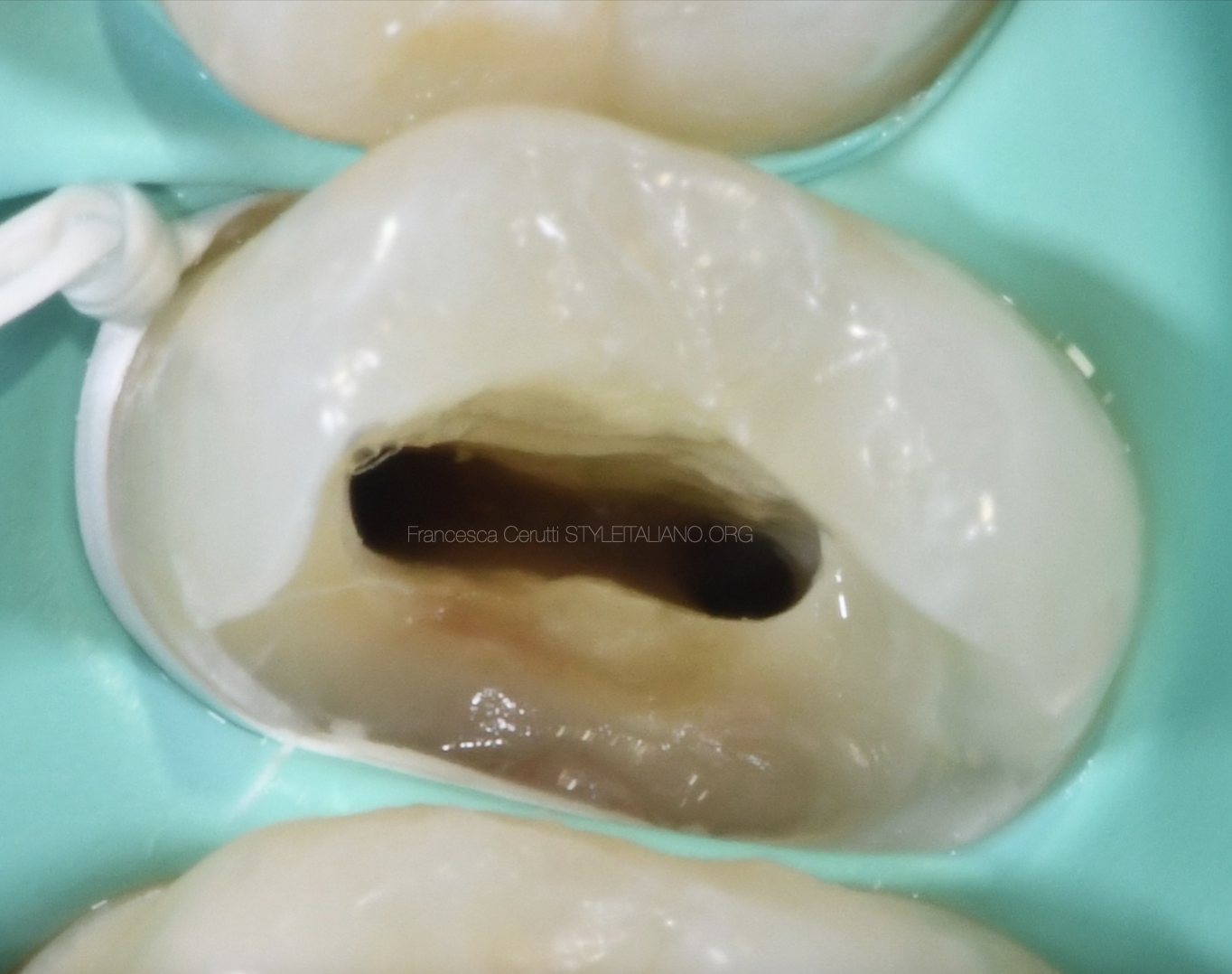
The patient came for the retreatment and I did a multiple isolation in order to have a better control on the axis of the tooth and with the idea of doing the endodontic and restorative treatment in the same appointment
I did the access cavity with a diamond coated bur, then I did the second phase with a ultrasonic tip
The tooth was filled with a carrier based system, so I treated the carrier as if it was a broken tool. With a this ultrasonic tip I did 1 mm of space all around the carrier, then I catched and removed it with a loop device.
After that I removed the remaining gutta percha with a ultrasonic tip and water
At this point I shaped the root canal system with the AF-F One Essential Kit by Fanta Dental.
I set the rows per minute at 400 and the torque at 2.5N. Considering it was a straight canal, I followed the "wide and easy" protocol.
A little extra care was taken while treating the last 3 mm of the root, since the previous therapy had stoped there.
There only was a block that was easy to pass with rotaries, so no particular technique was required to get to the apex.
I used the complete sequence of AF-F files because I wanted to be conservative but at the same time I needed to shape the canal to a sufficient diameter.
I checked the apical gauging and the fit of the gutta percha point
The tooth was directly restored with composite and the patient was referred to the prosthodontist for a crown

Fig. 5
The post endodontic x-ray shows the complete shaping of the root canal system with the preservation of radicular dentine.
Conclusions
When we shape the root canal system we want to be effective and conservative at the same time.
In retreatments we need to adapt to the previous shaping, but we can try to reduce dentine loss by adopting techniques and tools that allow us performing minimally invasive therapies.
Bibliography
Bürklein S, Schäfer E, Jöhren HP, Donnermeyer D. Quality of root canal fillings and prevalence of apical radiolucencies in a German population: a CBCT analysis. Clin Oral Investig. 2020 Mar;24(3):1217-1227. doi: 10.1007/s00784-019-02985-y. Epub 2019 Jul 15. PMID: 31312970.
Pirani C, Camilleri J. Effectiveness of root canal filling materials and techniques for treatment of apical periodontitis: A systematic review. Int Endod J. 2022.
Azim AA, Griggs JA, Huang GT. The Tennessee study: factors affecting treatment outcome and healing time following nonsurgical root canal treatment. Int Endod J. 2016;49(1):6-16.
Basmadjian-Charles CL, Farge P, Bourgeois DM, Lebrun T. Factors influencing the long-term results of endodontic treatment: a review of the literature. International dental journal. 2002;52(2):81-6.
Bergenholtz G. Assessment of treatment failure in endodontic therapy. Journal of oral rehabilitation. 2016;43(10):753-8.