A mandibular first molar with 6 root canals:
05/03/2024
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
One of the most important prerequisites for successful endodontic treatment is the adequate knowledge and understanding of root canal anatomy. The mandibular first molar (MFM) seems to be the tooth that most often requires root canal treatment and over the years numerous in vitro and in vivo studies have investigated its root canal morphology (1-3). This tooth usually has two roots (mesial and distal), with two root canals (mesiobuccal-MB and mesiolingual-ML) in the mesial root and one (distal) or two canals (distobuccal-DB and distolingual-DL) in the distal root. Rarely, a middle mesial canal (MM) is present in the developmental groove between the ΜΒ and ML canals at a range of 0-36% depending on the ethnical group (4). A middle distal canal (MD) may also be present at range of 0.2-3% between the DB and DL canals (5). However, the presence of six or more root canals is a rare entity and such teeth are described only in a small number of case reports in the literature (6-10).
A 37-year-old Greek female patient with a non-contributory medical history presented at the private dental office with severe spontaneous pain in the right mandibular region. The patient reported that she had previously initiated a root canal treatment of tooth #46 in another dentist. Clinically, the tooth #46 had a large amalgam restoration along with a temporary filling. Only the tooth #46 was tender to percussion, while the adjacent teeth responded normally to the vitality tests.

Fig. 1
Preoperative Radiograph. Α small radiolucency associated with the mesial root of tooth #46 was reported but no morphological variation was revealed. The diagnosis after clinical and radiographic examination was previously initiated therapy and symptomatic apical periodontitis.

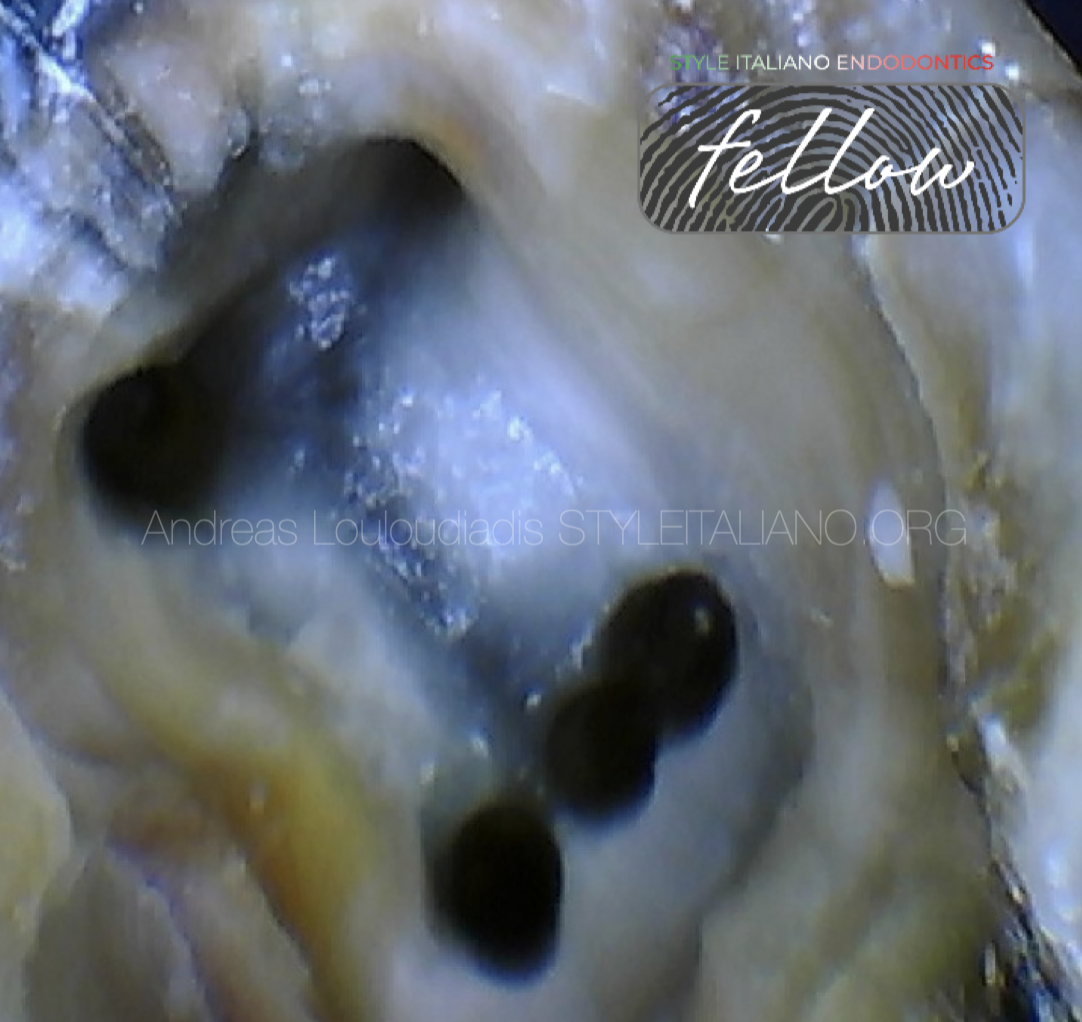
Fig. 2
Access Cavity Preparation. 3 canal orifices were detected initially: MB, ML and DB. The 1st and 2nd laws of symmetry of Krasner and Rankow were applied for the DL canal detection. As the MB and ML orifices were widely separated, troughing of their in-between groove with low speed round carbide burs and exploration using a DG 16 explorer revealed an additional MM canal. The same process was carried out along the isthmus extending between the DL and DB orifices and a MD canal was detected.

Fig. 3
Working length Determination With An Electronic Apex Locator (ENDY 6200, IONYX). Apical patency was achieved using C-Pilot 08, 10 stainless steel hand files (VDW). Cleaning and shaping of the root canals were done with rotary instruments (RACE EVO, FKG) until size 30.04 under copious irrigation with 3% NaOCl.

Fig. 4
Intraoperative Radiograph For Working Length Confirmation. The MM and MD canals were merging with the MB and DB canals in their middle third, respectively. All the mesial and distal canals joined apically.

Fig. 5
Intraoperative Radiograph With Fitted Gutta-percha Master Cones. The root canals were then dried with paper points and obturation was carried out using an epoxy resin sealer (DIA-PROSEAL, DIADENT) and the continuous wave of condensation technique.

Fig. 6
A temporary filling (Cavit G, 3M ESPE) was placed and three postoperative radiographs were taken from straight, mesial and distal horizontal angulations in order to assess the quality of obturation.

Fig. 7
About The Author: Dr. Ourania Tsiouma
2016: Award of Excellence in the Physiology course from the Laboratory of Experimental Physiology, Medical School, National and Kapodistrian University of Athens.
2015-2019: <<Antonios Papadakis>> scholarship holder during her undergraduate studies.
2019: 1st "Ioannis Karkatzoulis" Prize for the best Oral Presentation in the 19th Pampeloponnesian Dental Congress.
2020: Graduated second with honours from the Dental School of the National and Kapodistian University of Athens, Greece.
2020–2022: Research Associate in the Department of Endodontics, Dental School, National and Kapodistrian University of Athens.
2023: Master in Clinical and Surgical Microendodontics, University of Turin, Italy.
Author of scientific articles published in national and international peer-reviewed journals.
Fellow Member of Style Italiano Endodontics.
Private practice focused on Endodontics and Restorative Dentistry in Athens, Greece.
Conclusions
Adequate knowledge of the root canal system anatomy is an indispensable prerequisite to perform endodontic treatment. Although the presence of MFMs with 6 or more root canals is a rare entity, clinicians should be aware of this anatomical variation to avoid treatment failures. The laws of symmetry by Krasner and Rankow and access cavity modifications (from triangular to rectangular or rhomboidal) should be considered for detecting additional canals in both the mesial and distal roots of MFMs. The MM and MD orifices may initially not be visible due to the overlying internal triangular dentin which often conceals them and is lighter in color than the pulp chamber floor. Multiple canals should always be anticipated when an isthmus is clinically evident and there is a big distance between the orifices of the two main canals. The isthmus should be troughed with ultrasonic scalers or low speed burs and inspected for a potential sticky point. All possible attempts should be made to locate and treat the variable root canal configurations of MFMs to achieve a higher success rate.
Bibliography
- Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol 1984;58:589–99.
- Al-Qudah AA, Awawdeh LA. Root and canal morphology of mandibular first and second molar teeth in a Jordanian population. Int Endod J. 2009 Sep;42(9):775-84. doi: 10.1111/j.1365-2591.2009.01578.x. Epub 2009 Jun 22. PMID: 19549153.
- Gulabivala, K., et al. "Root and canal morphology of Burmese mandibular molars." International endodontic journal 34.5 (2001): 359-370.
- Nosrat A, Deschenes RJ, Tordik PA, Hicks ML, Fouad AF. Middle mesial canals in mandibular molars: incidence and related factors. J Endod. 2015 Jan;41(1):28-32. doi: 10.1016/j.joen.2014.08.004. Epub 2014 Sep 27. PMID: 25266468.
- Kottoor J, Sudha R, Velmurugan N. Middle distal canal of the mandibular first molar: a case report and literature review. Int Endod J. 2010 Aug;43(8):714-22. doi: 10.1111/j.1365-2591.2010.01737.x. Epub 2010 May 19. PMID: 20491988.
- Ghoddusi, Jamileh, et al. "Mandibular first molar with four distal canals." Journal of endodontics 33.12 (2007): 1481-1483.
- Martínez-Berná, Arturo, and Pedro Badanelli. "Mandibular first molars with six root canals." Journal of endodontics 11.8 (1985): 348-352.
- Reeh ES. Seven canals in a lower first molar. J Endod. 1998 Jul;24(7):497-9. doi: 10.1016/S0099-2399(98)80055-1. PMID: 9693579.
- Ryan JL, Bowles WR, Baisden MK, McClanahan SB. Mandibular first molar with six separate canals. J Endod. 2011 Jun;37(6):878-80. doi: 10.1016/j.joen.2011.03.005. Epub 2011 May 6. PMID: 21787510.
- 10.Kontakiotis EG, Tzanetakis GN. Four canals in the mesial root of a mandibular first molar. A case report under the operating microscope. Aust Endod J. 2007 Aug;33(2):84-8. doi: 10.1111/j.1747-4477.2007.00068.x. PMID: 17697250.