
A Mandibular First Molar with Radix Entomolaris and Middle Mesial Canal: a case report
02/02/2024
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
The goal of endodontic treatment is to eliminate all bacteria and their byproducts from the root canal system and to prevent reinfection. This is achieved with thorough mechanical and chemical cleansing of the entire root canal system and its complete filling with an inert filling material and an adequate coronal restoration to prevent future ingress of microorganisms. Many teeth do not respond to endodontic treatment because of persistent infection from a missed canal or failure to remove all pulp tissue and microorganisms from the root canal system.
It is of outmost importance that the clinician must have detailed knowledge of the pulp canal anatomy in order to achieve effectively proper cleaning and shaping of the root canal system.
Most mandibular first molars have two roots with two mesial and one or two canals in the distal root. However, studies have shown several variations in the anatomy of the mandibular molars. These variations include a separate distolingual root called radix entomolaris, C-shape anatomy, isthmus between MB and ML canals, and a third canal in the mesial root known as middle mesial.
The prevalence of Radix Entomolaris is < 5% in Caucasian, African, Eurasian, and Indian populations, whereas in those with Mongoloid traits, such as Chinese, Eskimo, and Native American populations the incidence of RE occurs with a frequency of 5% to even 40%.
The reported prevalence of Middle Mesial Canal in mandibular molars also varies among studies in the literature.
An assessment of the prevalence of Middle Mesial canal in mandibular first molar was published recently and included a cross-sectional study with Meta-analysis. The study found that MMC prevalence ranged from 1%-23% and the overall prevalence was 7%.
The anatomy of MM canal has been described in the literature as follows:
1. Fin: The file passes freely between main mesial canal (MB or ML) and MM canal.
2. Confluent: The MM canal originates as separate orifice but apically joins the MB or Ml canal, and
3. Independent: The MM canal originates as a separate orifice and terminates as a separate apical foramen.
The present case report describes the clinical detection and endodontic management of both a RE and MMC on a mandibular first molar.

Fig. 1
A 58 years old female was referred for Endodontic Assessment of 46. The patient had pain on biting and sensitivity to cold. Upon clinical examination the 46 had large amalgam restoration, was very tender to percussion and responded with discomfort on thermal stimuli. No perio pockets or mobility was detected. Patient was informed of possible crack under restoration and questionable prognosis. She was under bisphosphonate treatment, and she wanted to avoid loss of tooth at any cost. A decision to perform endodontic treatment of tooth 46 was made and patient understood that prognosis was questionable.
Pre-op xray reveals sclerotic canals and the presence of Radix is noted. Pulp chamber also looks obliterated indicating presence of pulp stone.
Careful examination and assessment of the pre-op radiographs its essential for the management and outcome of the endodontic treatment.

Fig. 2
Pre-operative photo of tooth 46 revealing large amalgam restoration and buccal composite. Patient was informed of possible crack under amalgam restoration and questionable prognosis of tooth.

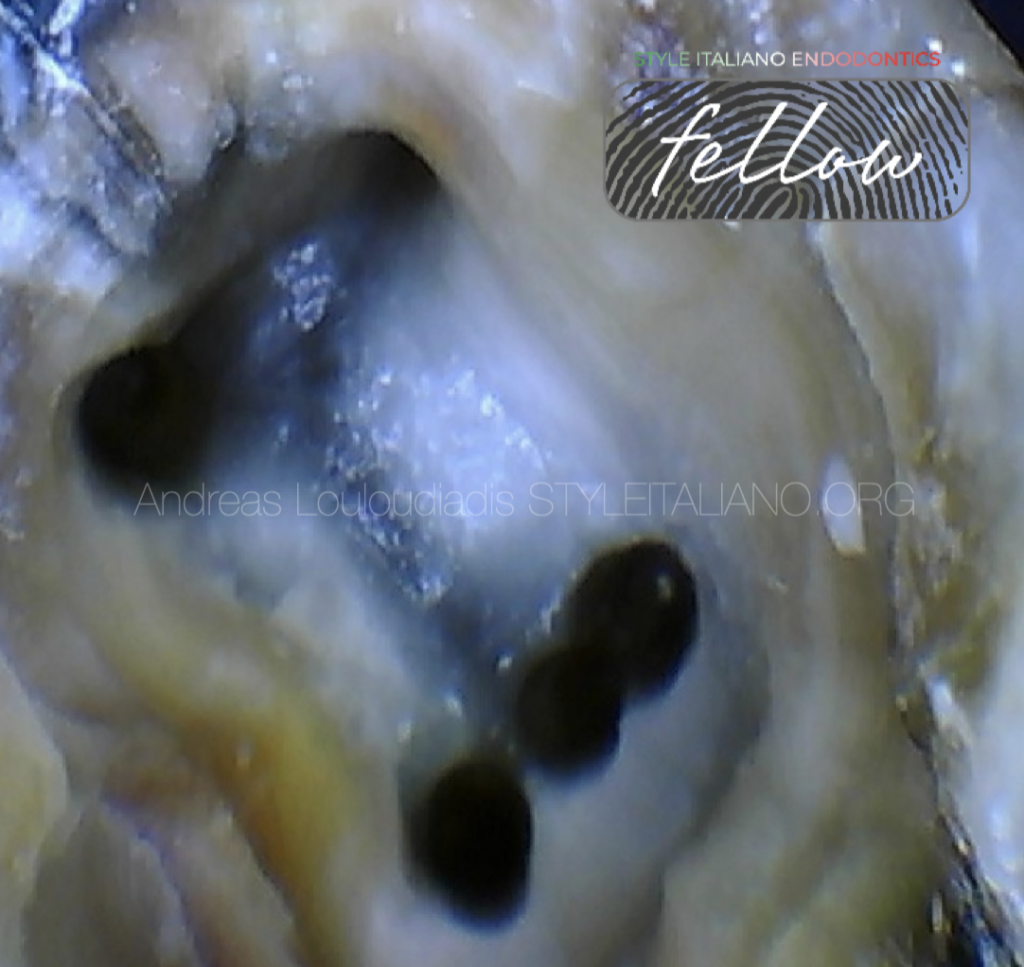
Fig. 3
Removal of amalgam restoration and deroofing pulp chamber with ultrasonics under microscope and noticing the MM canal.

Fig. 4
Working Length determination. The canals were scouted with 08k and 10k stainless –steel hand files. To determine the working length an electronic apex locator was also used. The mesial canals were very sclerotic, and use of D-finders hand files were used to established patency.
The MM canal anatomy was confluent with MB canal. It originated as a separate orifice but apically joined the MB canal.
Achieving apical patency on MMC with D-finder file.
D-finders are almost 50% stiffer compared to conventional K-files.
This property improves the penetration force which is needed to prepare glide path of root canals which are narrowed by calcification.
Copious irrigation with 5,25% sodium hypochlorite and throughout the endodontic treatment.
Irrigation protocol included irrigation with 5,25% Noocl, 17% EDTA and activation of irrigants with the use of Ultra-X
(Eighteeth).
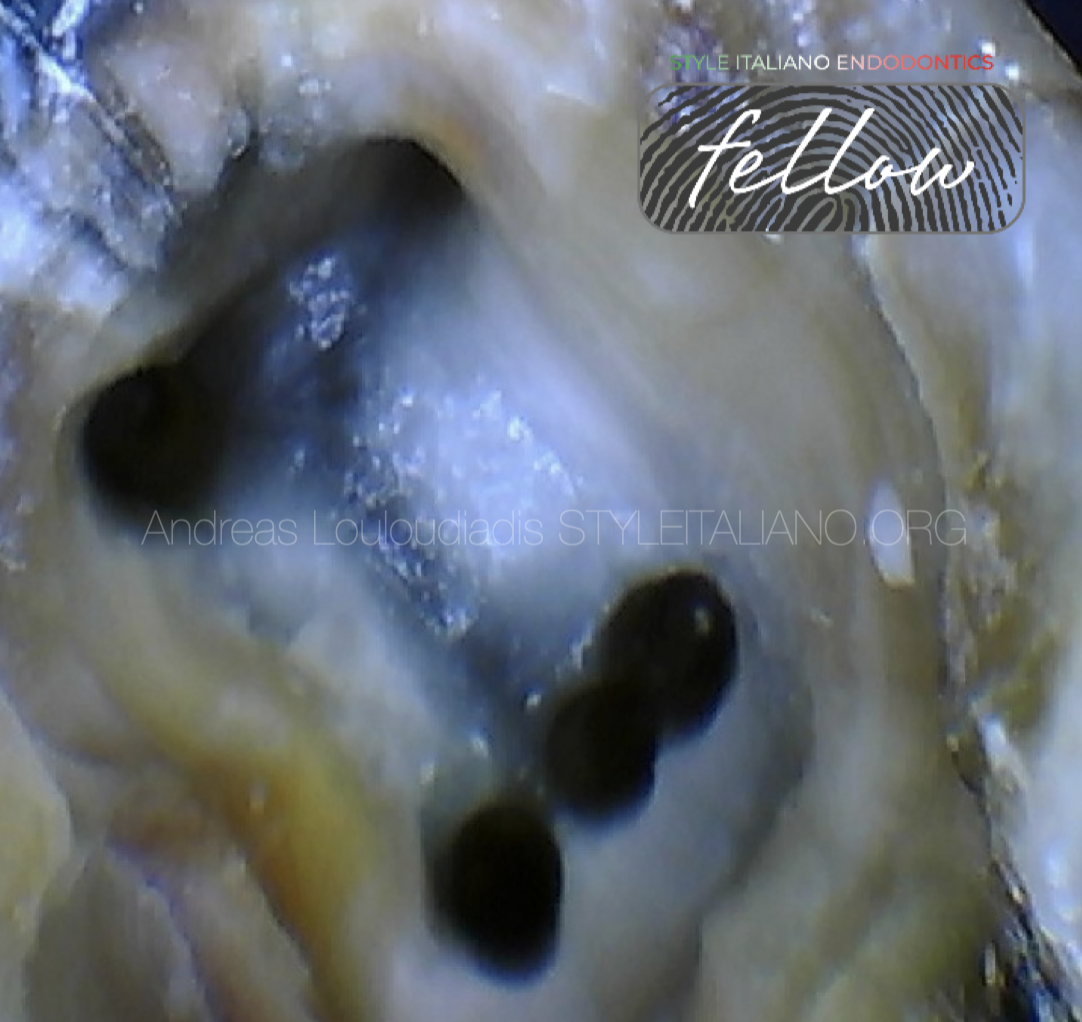
Fig. 5
All the canals were shaped with Hyflex EDM 15/03, 10/05, 20/05 and 25 One File ( Coltene).
Notice the crack on the distal wall.
Patient was informed about its presence and the questionable prognosis of the tooth.
Patient was on Bisphosphonate treatment and did not want to lose the tooth due to risk of osteonecrosis, but she was realistic about her expectations and decided to proceed with the Endodontic treatment of the tooth despite the questionable prognosis.
Placement of AH-plus Bioceramic sealer on Radix Entomolaris canal and Modified Warm vertical compaction using Fast Pack (Eighteeth).
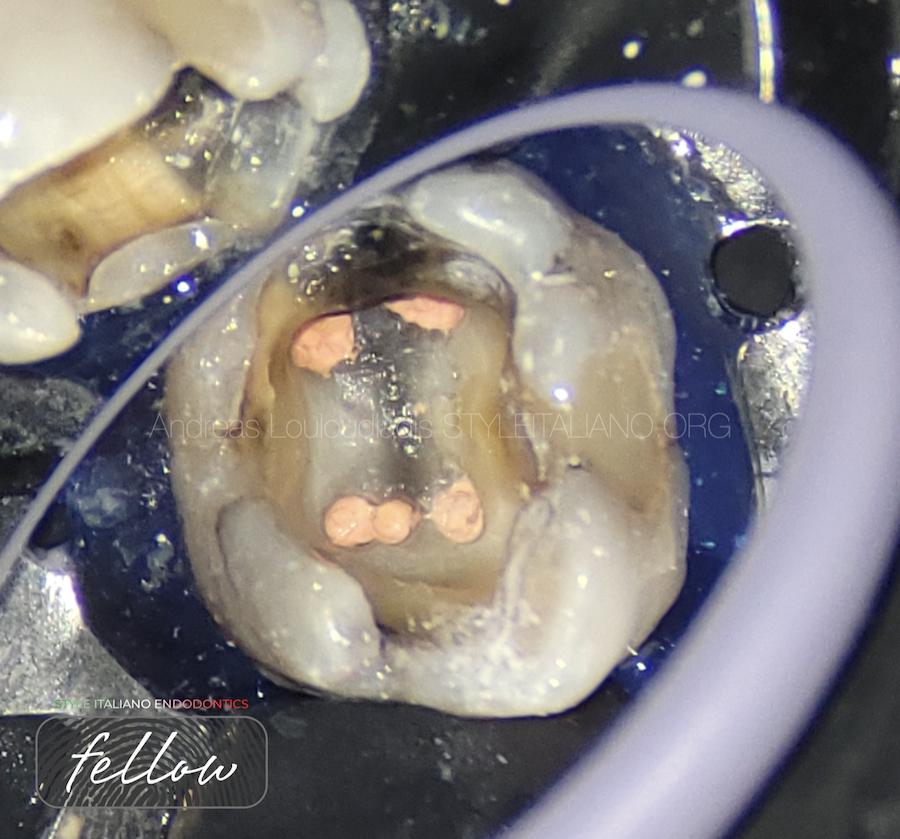
Fig. 6
Obturation done with AH-plus Bioceramic sealer ( Dentsply) and modified Warm Vertical Compaction.
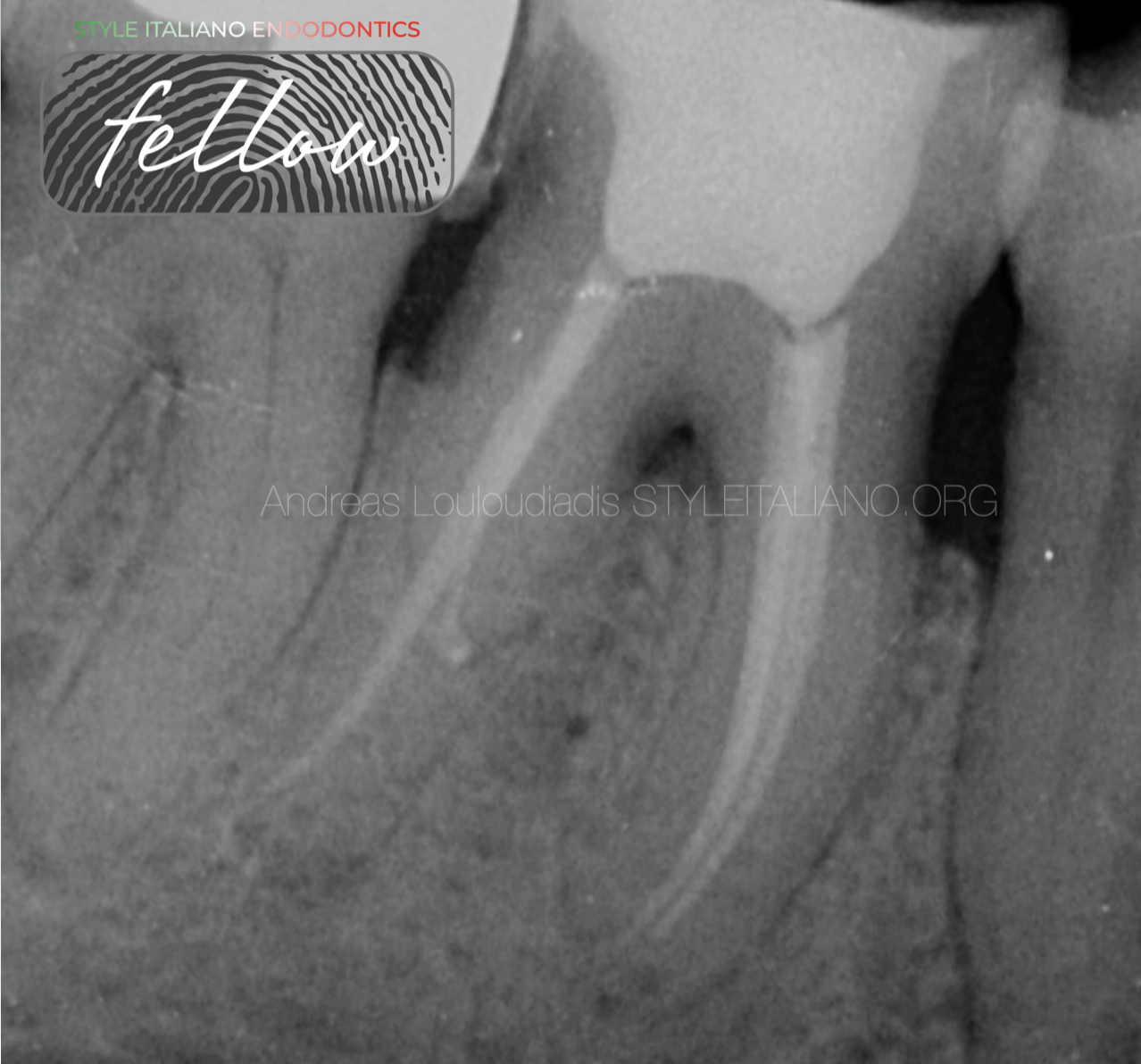
Fig. 7
Final X-ray of tooth 46.
The MM is converging with MB canal at the apical 1/3.
Access cavity was restored with composite resin and patient was referred back to her dentist for an indirect cast restoration.

Fig. 8
Final X-ray of tooth 46.
Mesial shift
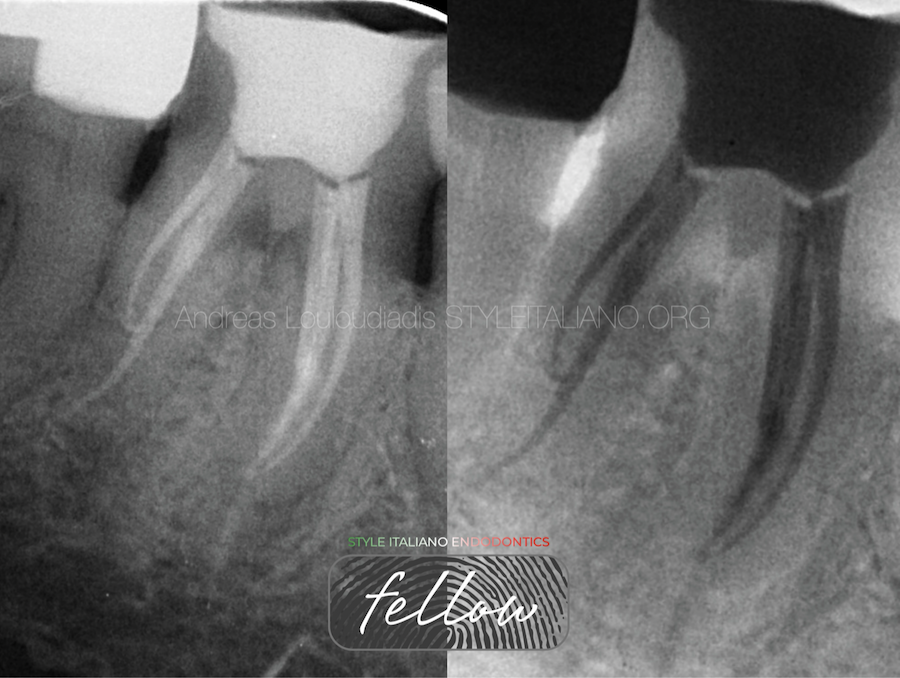
Fig. 9
Final X-ray of tooth 46.
Distal shift
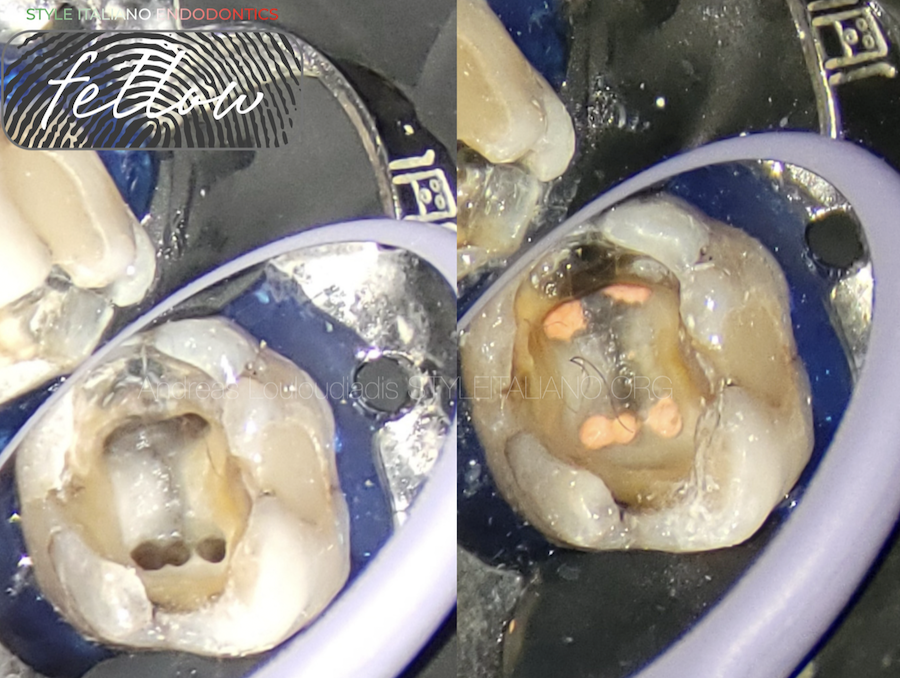
Fig. 10
Before and after obturation of tooth 46.

Fig. 11
About the author: Andreas Louloudiadis
DMD 2001 University of Alabama USA
PGDip in Endodontics 2005 Aristotle University Greece
MSc in Advanced Endodontics 2023 Siena Italy
Certified Member of European Endodontic Society
Member of British Endodontic Society
Member of Hellenic Association of Endodontists
Fellow of SIE
Conclusions
Clinicians should be aware of the unusual anatomical features and variations in the mandibular first molars. A detailed knowledge of the pulp canal anatomy, multiple angulated radiograph and close inspection of the chamber floor at higher magnification with the help of operating microscope is key to locating and treating unusual anatomy.
Variations of anatomy do exist more often than we think, so as long as we have the knowledge, the right armamentarium and good clinical skills we can prepare, clean, disinfect and obturate any of them efficiently and successfully.
Bibliography
Nosrat A, Deschenes R, Tordik P, Hicks L, Fouad A. Middle mesial Canals in Mandibular Molars: Incidence and related Factors. J Endod 2015 Jan;41(1):28-32.
Hatipoglu F, Magat M, Hatipoglu O, Bhati U, Palma P, Martins J. Assessment of the prevalence of Middle Mesial Canal in Mandibular First Molars: A Multinational Cross-sectional Study with Meta-analysis. J Endodd 2023 May;49 (5) 549-558.
Campos F. Three canals in the mesial root of mandibular first permanent molars: a clinical study. Int Endod J. 1989;22:39-43.
De Moor R.J, Deroose JG, Calberson F. The radix entomolaris in mandibular first molars: an endodontic challenge. Int Endod J. 2004;37:789-799.
Abella F, Mercafde M, Sindreu F, Roig M.Managing severe curvature of radix entomolaris: three-dimensional analysis with cone beam computed tomography. Int Endodd J. 2011;44:876-885.
Baugh D., Wallace J. Middle mesial canal of the mandibular first molar: a case report and literature review. J. Endod. 2004;30:185–186.
Pomeranz HH, Eidelman DI, Goldberg MG. Treatment considerations of the middle mesial canal of mandibulars first and second molars. J Endod 1981;7:565-8.



