Single-stage crown lengthening and papilla reconstruction with a sub-epithelial connective tissue graft (SCTG) for subcrestal external cervical resorption (ECR) in the esthetic zone
08/07/2026
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
The joint workshop of the AAP (American Academy of Periodontology) and the EFP (European Federation of Periodontology) reaffirmed that positioning the restorative margin within the fibers of the supracrestal connective tissue attachment represents a significant risk factor for the development of periodontal complications.
It is essential to recall that the supracrestal attachment shows considerable dimensional variability, both inter- and intra-patient, ranging from 0.2 to 6.73 mm. The relatively constant component is the connective attachment, averaging 1–1.5 mm; thus, the portion associated with the junctional epithelium shows the greater variability between the two.
When a dental lesion presents a margin extending apically to the gingival sulcus, it is imperative to assess whether that margin lies within the junctional epithelium space, more deeply within the connective attachment, or even apical to the bone crest. In cases where the lesion invades the connective attachment or is apical to the crest, clinical crown lengthening becomes necessary to expose the margin, ensure proper restorative/prosthetic reconstruction, and reduce the risk of future periodontal damage.
External cervical resorption (ECR) is an insidious form of dental resorption, often asymptomatic and difficult to detect clinically, typically identified on radiographic examination or by the appearance of a pinkish/grayish discoloration at the cervical level.
Historically, the lesion was described using the two-dimensional Heithersay classification (1999), based on the extent of resorptive invasion into the coronal and radicular dentin — four classes, from a superficial cervical lesion to a process extending beyond the coronal third of the root. The limitation of this approach is intrinsic to the radiographic medium: the periapical radiograph tends to underestimate the true extent of the defect.Because periapical radiography underestimates the lesion, the CBCT-based three-dimensional Patel classification (2018) is today preferred. It describes the lesion along three axes:
Height — 1: at CEJ or coronal to the bone crest (supracrestal); 2: coronal third, apical to the crest (subcrestal); 3: middle third; 4: apical third.
Circumferential spread — A: ≤90°; B: ≤180°; C: ≤270°; D: >270°.
Proximity to the root canal — d: confined to dentin; p: probable pulpal involvement.
The height parameter is particularly significant from a periodontal standpoint: it directly maps the relationship of the lesion to the bone crest, and it is precisely this datum that guides the decision to perform crown lengthening.Clinical crown lengthening is, by definition, a resective procedure: by repositioning the bone crest apically, the space required for re-establishment of the supracrestal connective attachment is created, bringing the margin of the lesion/restoration coronal to it. The typical biological price of this maneuver, in the esthetic zone, is flattening of the interdental papilla and the risk of “black triangles,” as a consequence of the increased distance between the contact point and the bone crest — a parameter that, as is known, conditions the filling of the interproximal space (Tarnow).
The element of originality of this case lies in reversing the sign of the procedure at the same site: after resective surgery respects the biology of the connective attachment, a reconstructive approach is undertaken with a de-epithelialized connective tissue graft sutured to the periosteum, to restore volume and structure to the papilla. Two distinct compartments of the supracrestal attachment are addressed — the connective component (constant) is respected through osseous resection, and a zone pertaining to the junctional epithelium and interproximal soft tissue is reconstructed with soft tissues. Resection and reconstruction thus coexist in a single esthetic-therapeutic strategy, in one surgical stage.
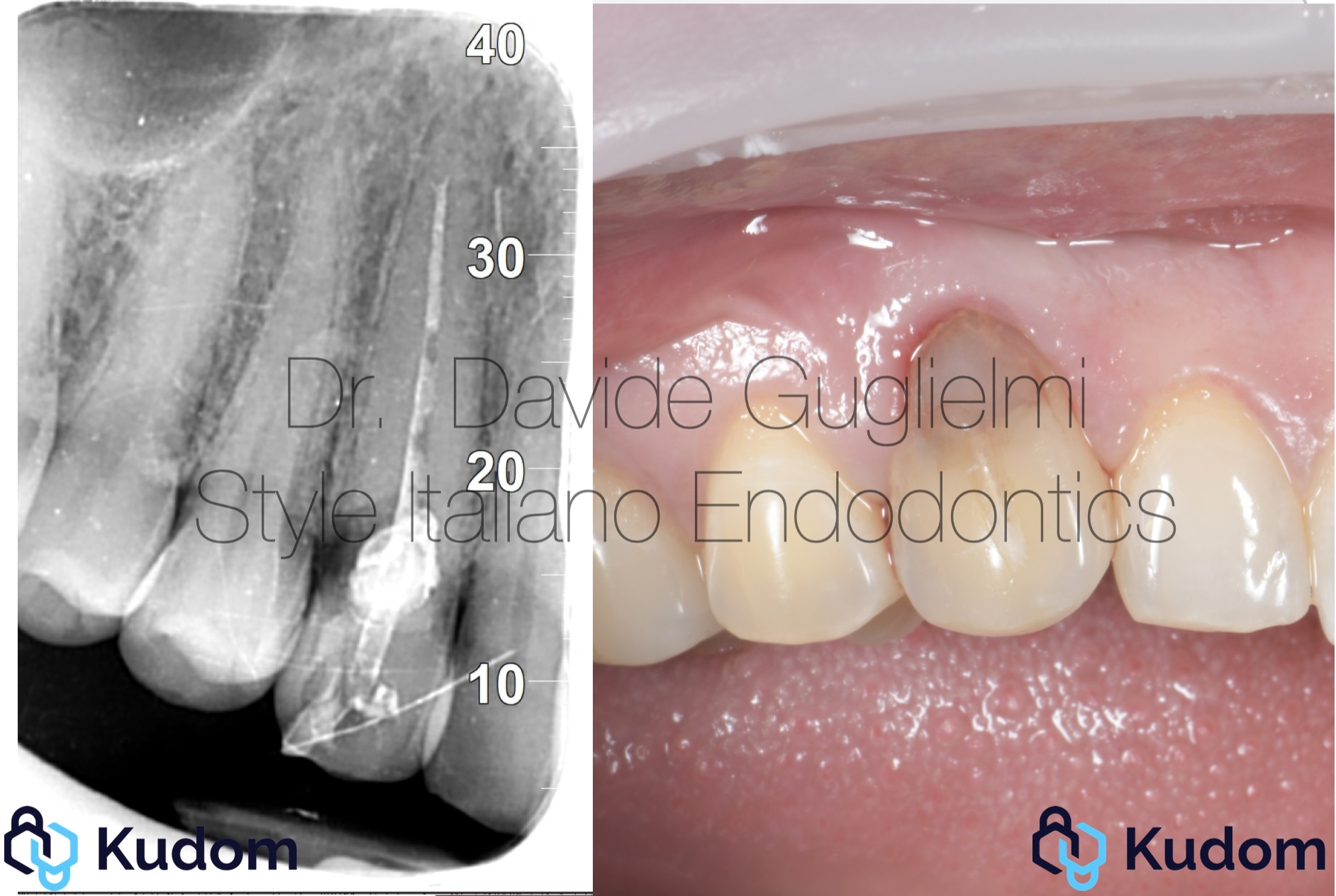
Fig. 1
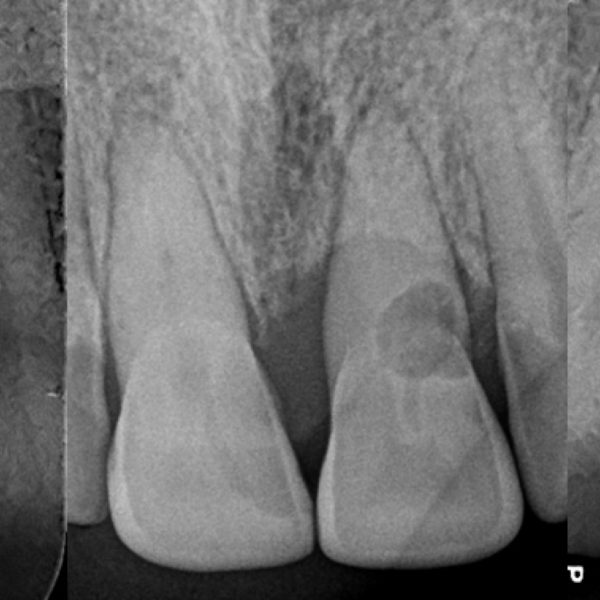
Initial situation of tooth 1.3: buccal view and periapical radiograph. The characteristic pinkish-grayish discoloration of the cervical third is appreciable, suggestive of external cervical resorption, with the lesion margin located subgingivally.

Fig. 2
Periodontal and clinical probing of the defect to assess its extent and its relationships with the surrounding tissues.

Fig. 3
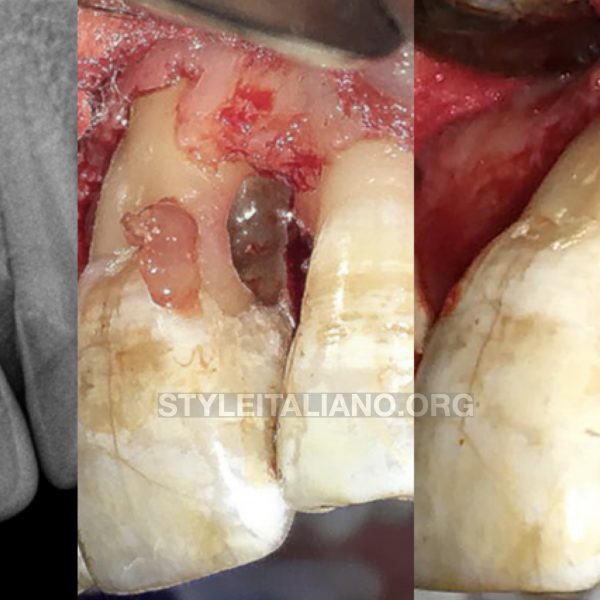
Elevation of a split-full-split thickness envelope flap: exposure of the resorptive defect on the buccal root surface.

Fig. 4
Bone sounding at various points to define the distance between the apical margin of the lesion and the bone crest, planning the extent of crown lengthening needed to create space for the supracrestal connective attachment.

Fig. 5
Appearance of the cervical defect after the papilla elevation: the resorptive cavity is clearly evident with the presence of a bone-like tissue.

Fig. 6
Ostectomy: remodeling of the bone profile to recontour the crest.

Fig. 7
Ostectomy and osteoplasty: reduction of the bone crest height to create the space intended for the supracrestal connective attachment.

Fig. 8
Verification, by means of repeated bone sounding, of the space created for the supracrestal connective attachment relative to the margin of the future restoration.
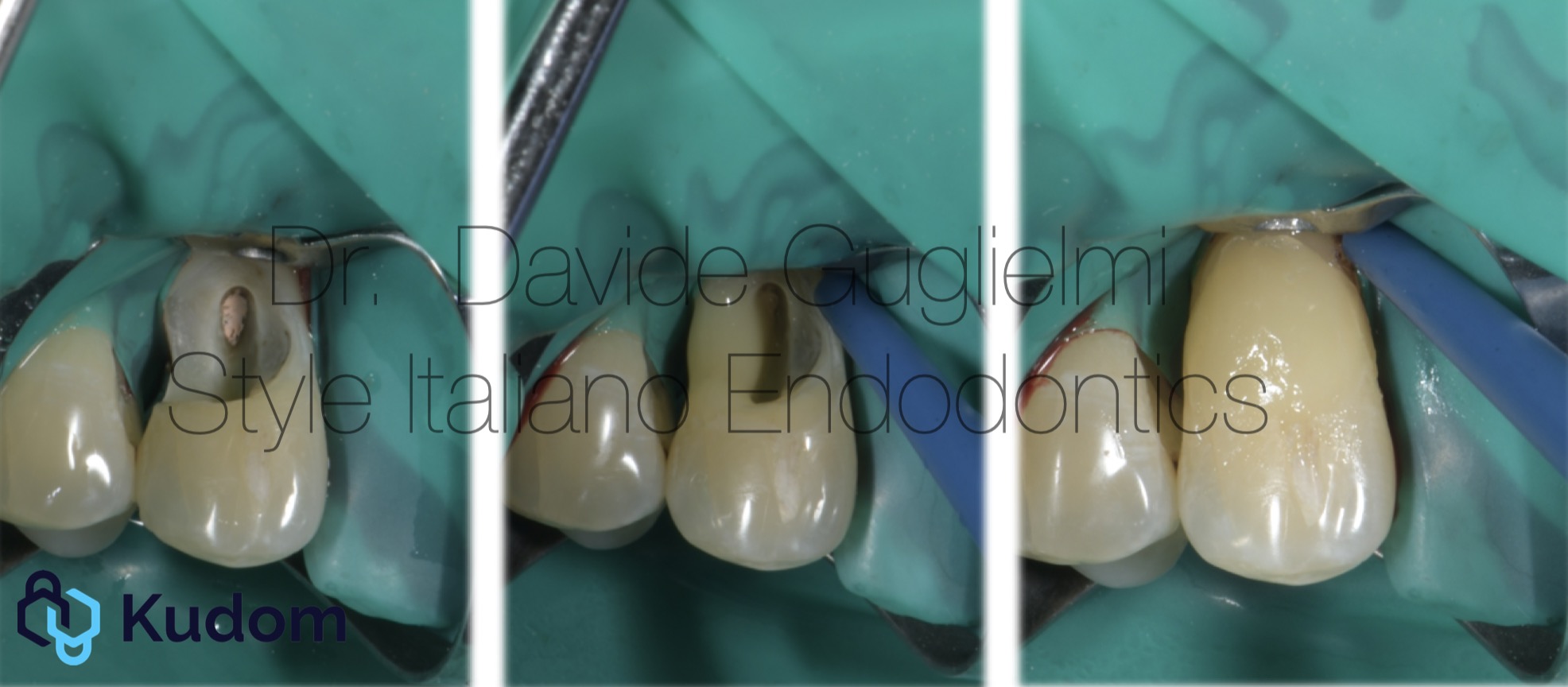
Fig. 9
Open flap isolation of the operative field with rubber dam and adhesive reconstruction of the cervical defect with flowable composite and composite (progressive stages). Endodontic retreatment, indicated by the probable pulpal involvement of the lesion (Patel “p” parameter), was performed at a subsequent appointment.

Fig. 10
Restoration completed; the flap, still elevated, reveals the interproximal site intended for papillary reconstruction.

Fig. 11
Placement of the de-epithelialized connective tissue graft — harvested from a molar site — in the interproximal position, to restore volume and structure to the papilla.
Stabilization of the graft: horizontal mattress suture at the palatal flap and 2 simple periosteal buccal sutures, in resorbable 7-0 (Stoma) thread. To be noticed the de-epithelialization of the anatomical papilla.

Fig. 12
Buccal view at the end of surgery, with modified suspended sutures in place.

Fig. 13
Harly healing, at the time of suture removal.

Fig. 14
One-month follow-up: maturation of the soft tissues and progressive filling of the papillary space.
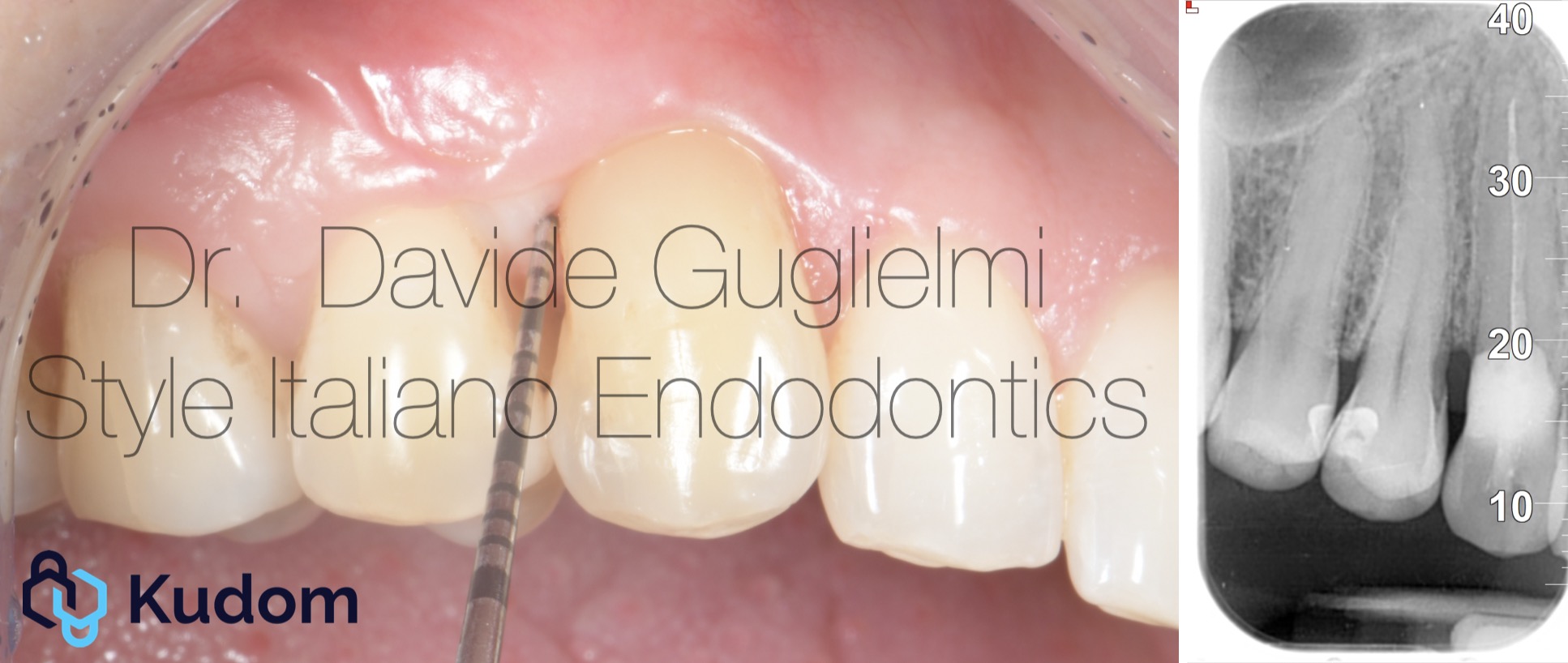
Fig. 15
Twelve-month follow-up: reconstructed papilla, stable margin, physiological probing; the control radiograph confirms the stability of the result over time.
Conclusions
In the esthetic management of subcrestal external cervical resorption, combining resective crown lengthening — to respect the supracrestal connective attachment — with a de-epithelialized connective tissue graft that reconstructs the papilla within the same surgical stage reconciles periodontal biology with esthetics, while limiting the bone sacrifice imposed by the classic resective protocol.
Bibliography
1. Patel S, Foschi F, Mannocci F, Patel K. External cervical resorption: a three-dimensional classification. Int Endod J. 2018;51(2):206-214.
2. Heithersay GS. Invasive cervical resorption: an analysis of potential predisposing factors. Quintessence Int. 1999;30(2):83-95.
3. Marzadori M, Stefanini M, Sangiorgi M, Mounssif I, Monaco C, Zucchelli G. Crown lengthening and restorative procedures in the esthetic zone. Periodontol 2000. 2018;77(1):84-92.
4. Schmidt JC, Sahrmann P, Weiger R, Schmidlin PR, Walter C. Biologic width dimensions — a systematic review. J Clin Periodontol. 2013;40(5):493-504.
5. Tarnow DP, Magner AW, Fletcher P. The effect of the distance from the contact point to the crest of bone on the presence or absence of the interproximal dental papilla. J Periodontol. 1992;63(12):995-996.
6. Zucchelli G, De Sanctis M. Treatment of multiple recession-type defects in patients with esthetic demands. J Periodontol. 2000;71(9):1506-1514.
7. Smith SC, Goh R, Ma S, Nogueira GR, Atieh M, Tawse-Smith A. Periodontal tissue changes after crown lengthening surgery: a systematic review and meta-analysis. Saudi Dent J. 2023;35(4):294-304.
8. Pittaluga A, Minoli M, Diana C, Bovio M, Guglielmi D. Rilocazione del margine e allungamento di corona clinica. Parte 1. Quintessenza Int. 2024;38(1):34-42.
9. Parma-Benfenati S, Fugazzotto PA, Ruben MP. The effect of restorative margins on the postsurgical development and nature of the periodontium. Part I. Int J Periodontics Restorative Dent. 1985;5(6):30-51.
10. Ghezzi C, Brambilla G, Conti A, Dosoli R, Ceroni F, Ferrantino L. Cervical margin relocation: case series and new classification system. Int J Esthet Dent. 2019;14(3):272-284.
11. Fichera G, Mazzitelli C, Picciariello V, Maravic T, Josic U, Mazzoni A, Breschi L. Structurally compromised teeth. Part I: clinical considerations and novel classification proposal. J Esthet Restor Dent. 2024;36(1):7-19.