Case report Management of Dens Invaginatus type IIIA
02/02/2025
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
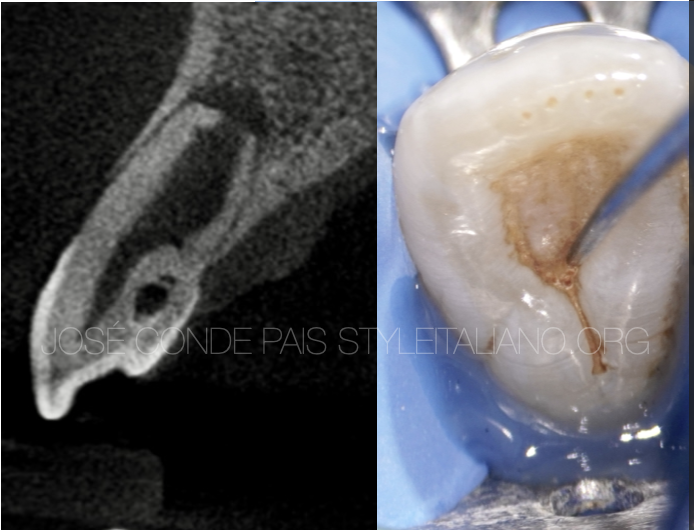
This article showing the Management of Dens Invagenatus of upper lateral incisor with large periapical lesion.
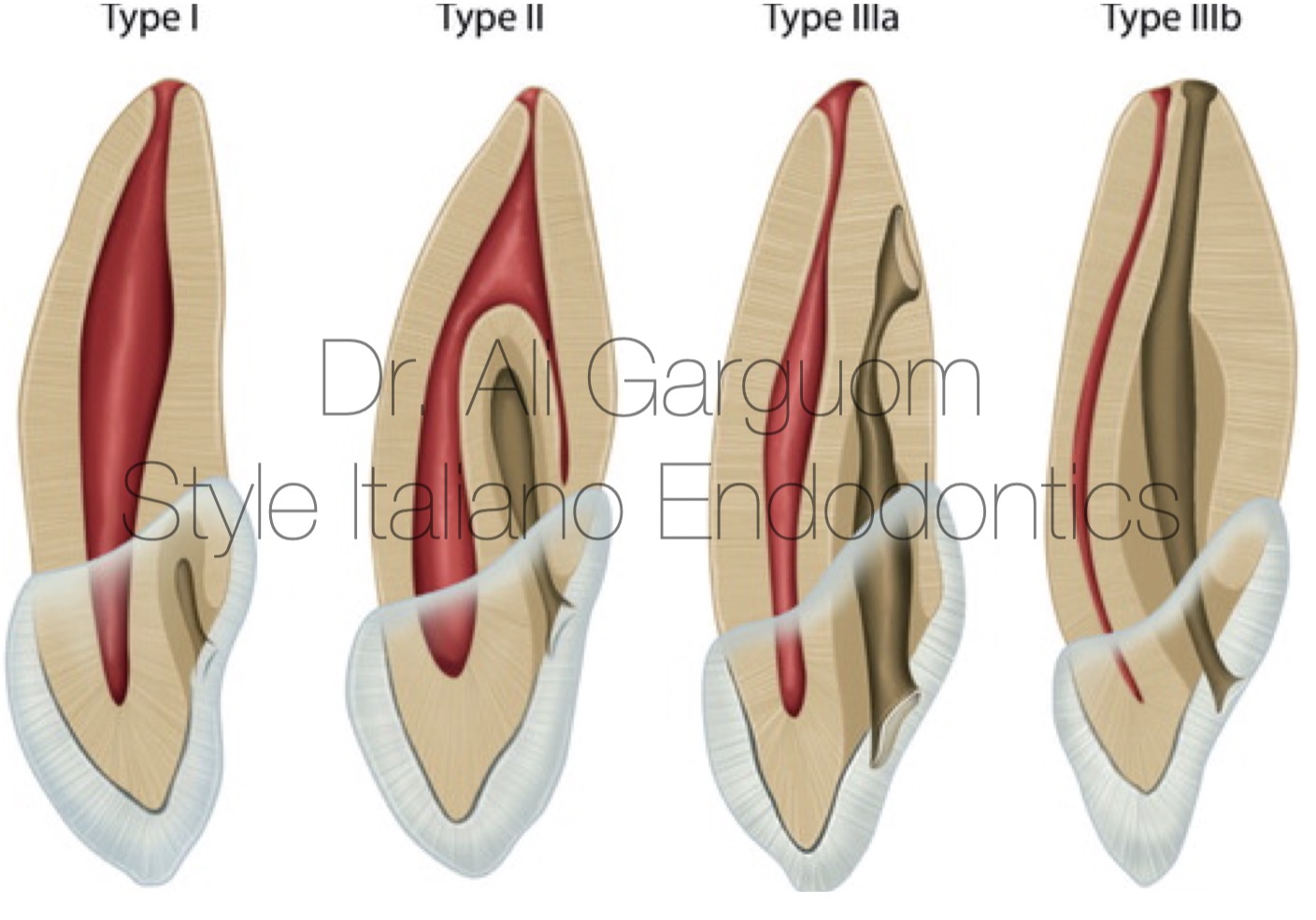
Fig. 1
Oehler (1957) has classified DI into different types based on the extent of involvement as;
Type I: Enamel-line, minor form confined to tooth crown not extending beyond the CE junction.
Type II: Enamel-lined form which invades the root but remains confined as a blind sac. It may or may not communicate with the dental pulp.
Type III A: Invagination extends through root & communicates laterally with PDL space through pseudo-foramen. No communication with pulp.
Type III B: Invagination extends thru root & communicates with PDL at apical foramen. No communication with pulp.

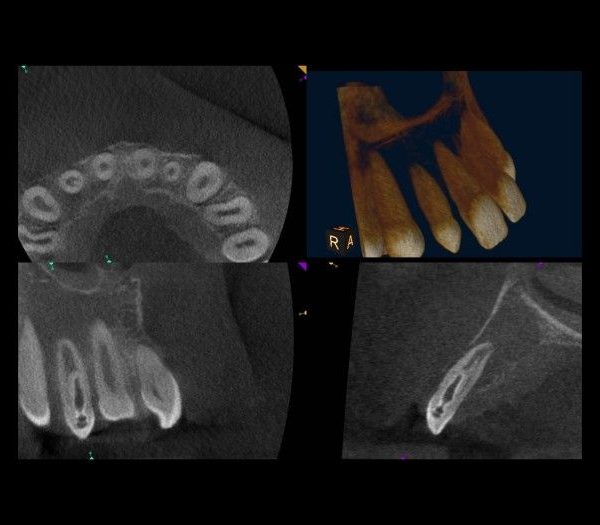
Fig. 2
Preoperative CBCT
A 25 years old female her chief complaint was pain associated swelling related to upper left lateral .
On IOPA abnormal anatomy was noticed and FOV CBCT was asked .
On CBCT dens invagenatus type III A according to oehler classification was found .

Fig. 3
Two separated access was done to preserve the tooth structure
The invagination will be lined with enamel and cementum. Endodontic files are not indicated for use to debride these lesions as they will be ineffective.
-Ultrasonic tips can be used to debride the lesions, and irrigation should be ultrasonically activated to maximize their efficacy and ensure complete detriment .
-The invagination will communicate with the periodontal ligament that is why MTA obturation will promote healing of the peri-radicular tissues
-The pulpal portion of the tooth should be treated conventionally with endodontic files, with thorough irrigation of sodium hypochlorite and full irrigation protocol .
obturation with thermoplastic guttapercha (to ensure that the complex anatomy has been completely sealed)

Fig. 4
Cervical constriction prevent proper condensation of MTA

Fig. 5
Use ultra sonic to remove the construction

Fig. 6
Check the passive insertion of plugger
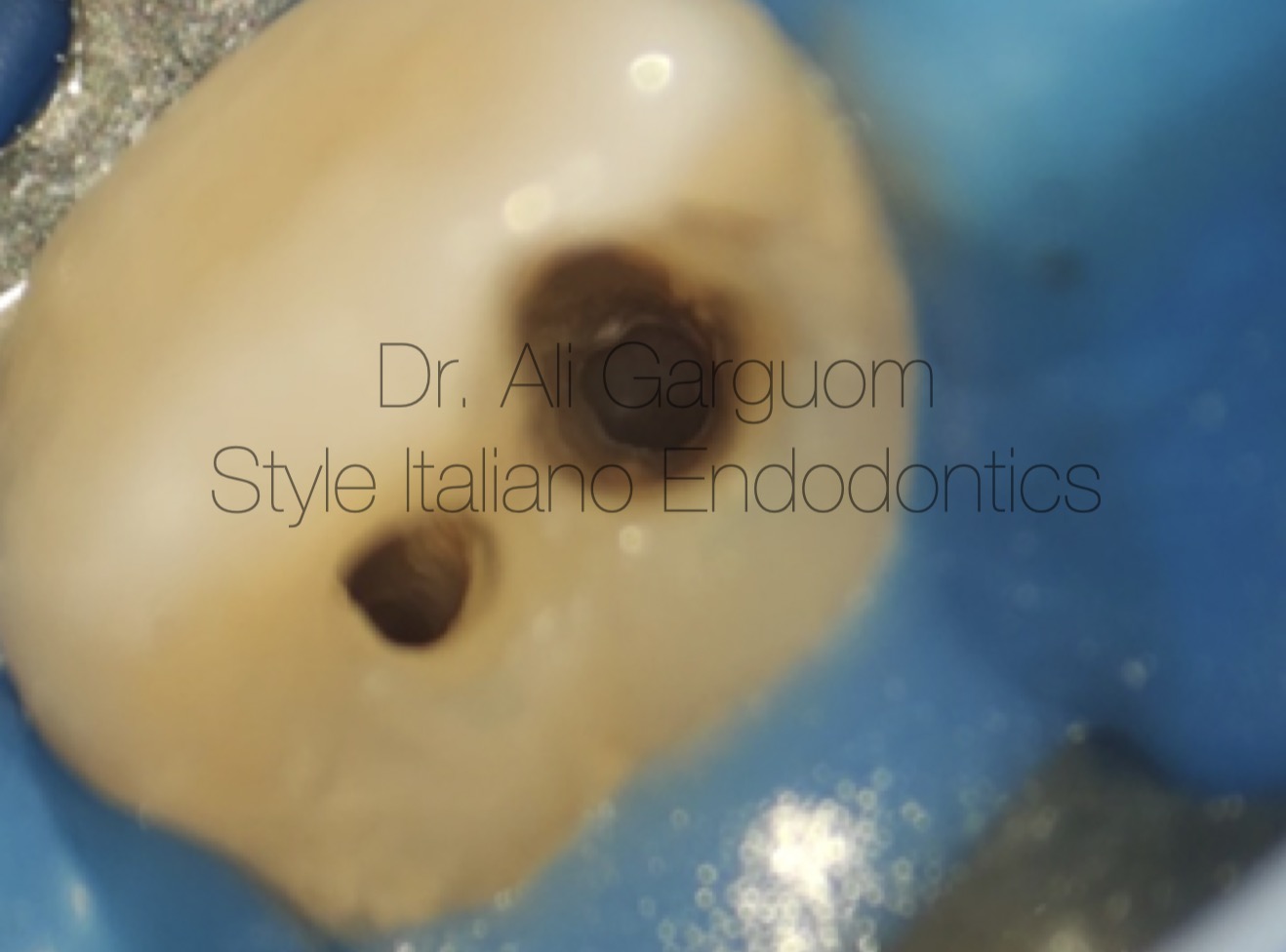
Fig. 7
After cleaning and shaping
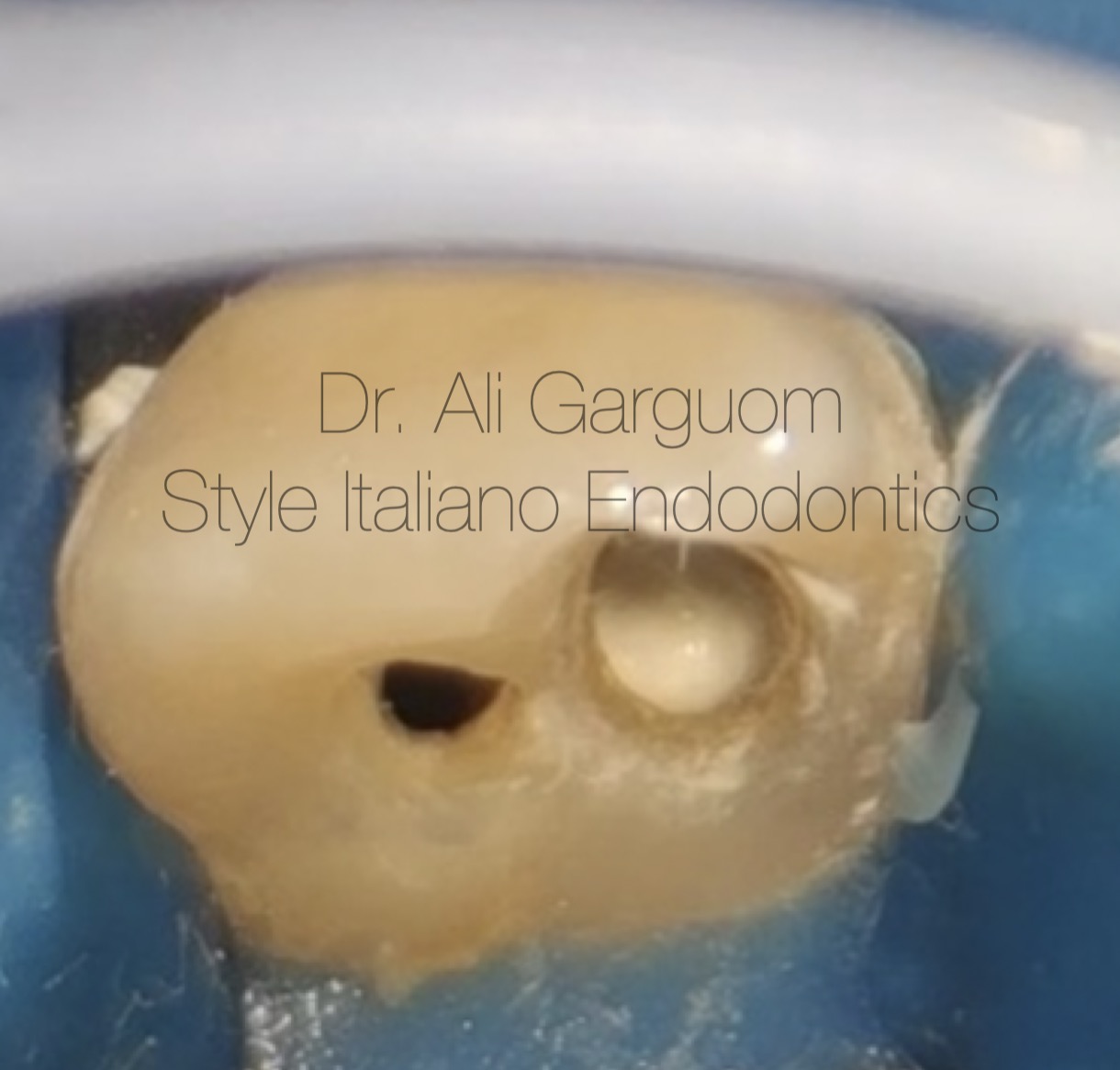
Fig. 8
MTA plug in invagination to obturate the pseudo-foramen

Fig. 9
Modified warm obturation to main canal
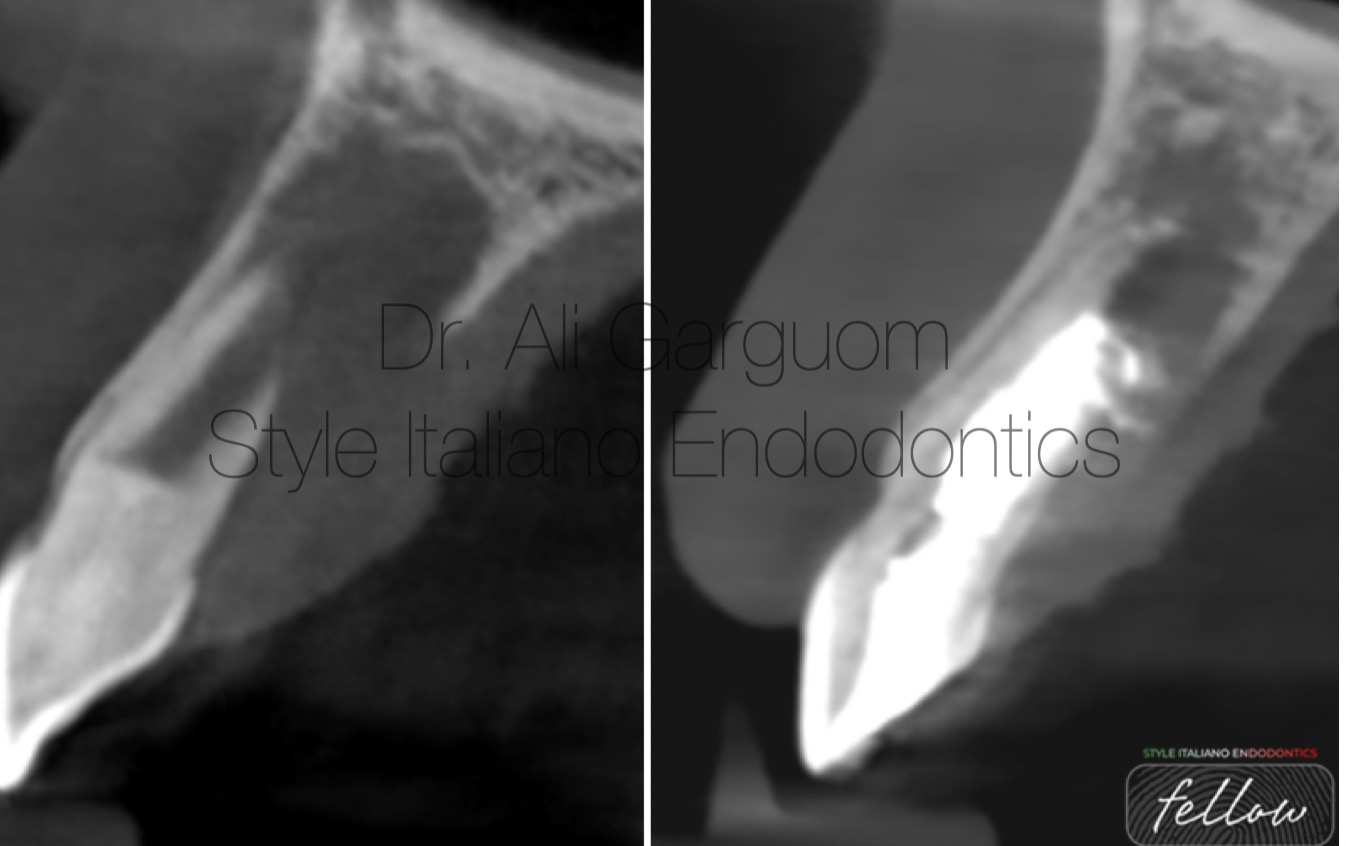
Fig. 10
Follow up one year
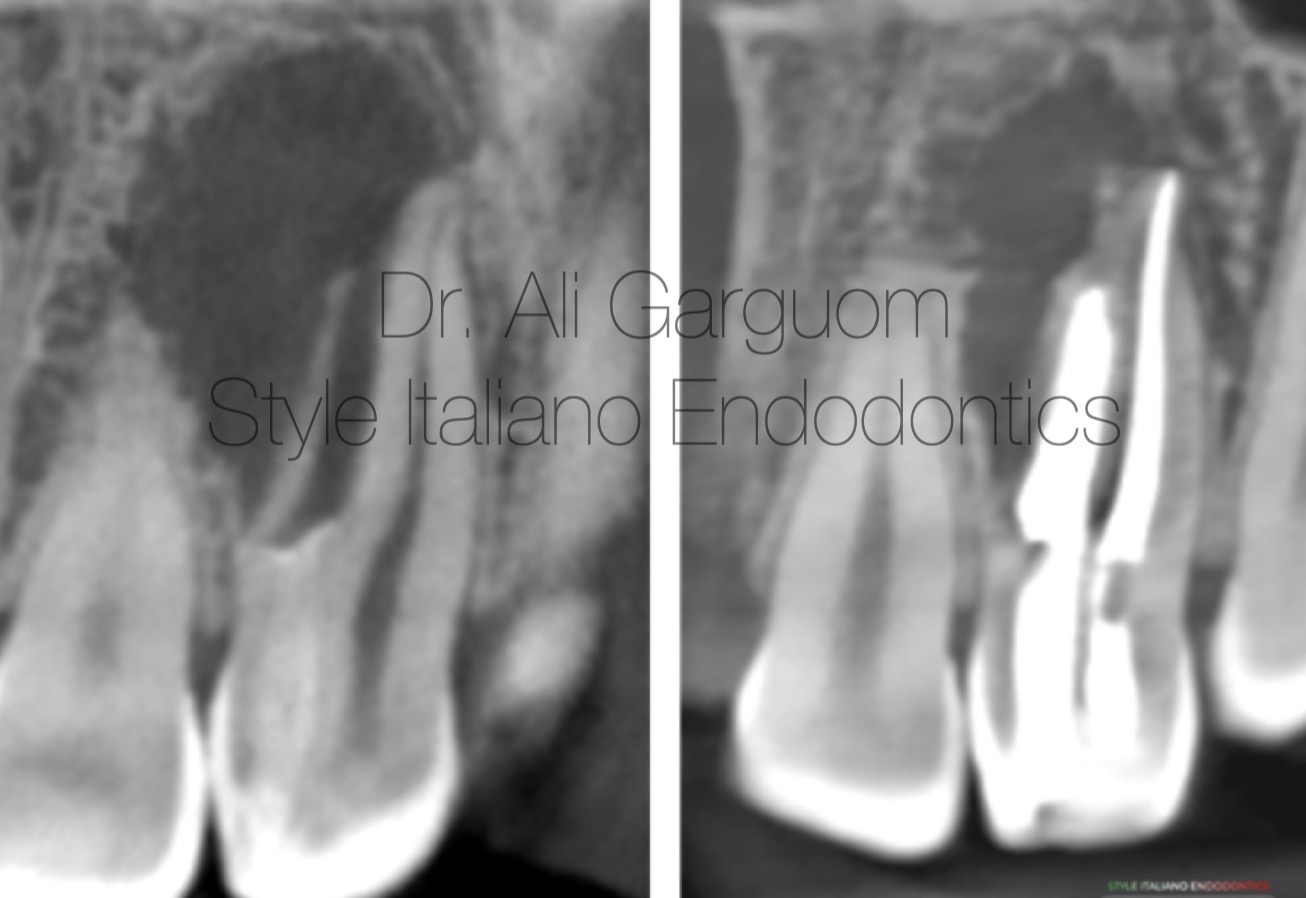
Fig. 11
Follow up one year
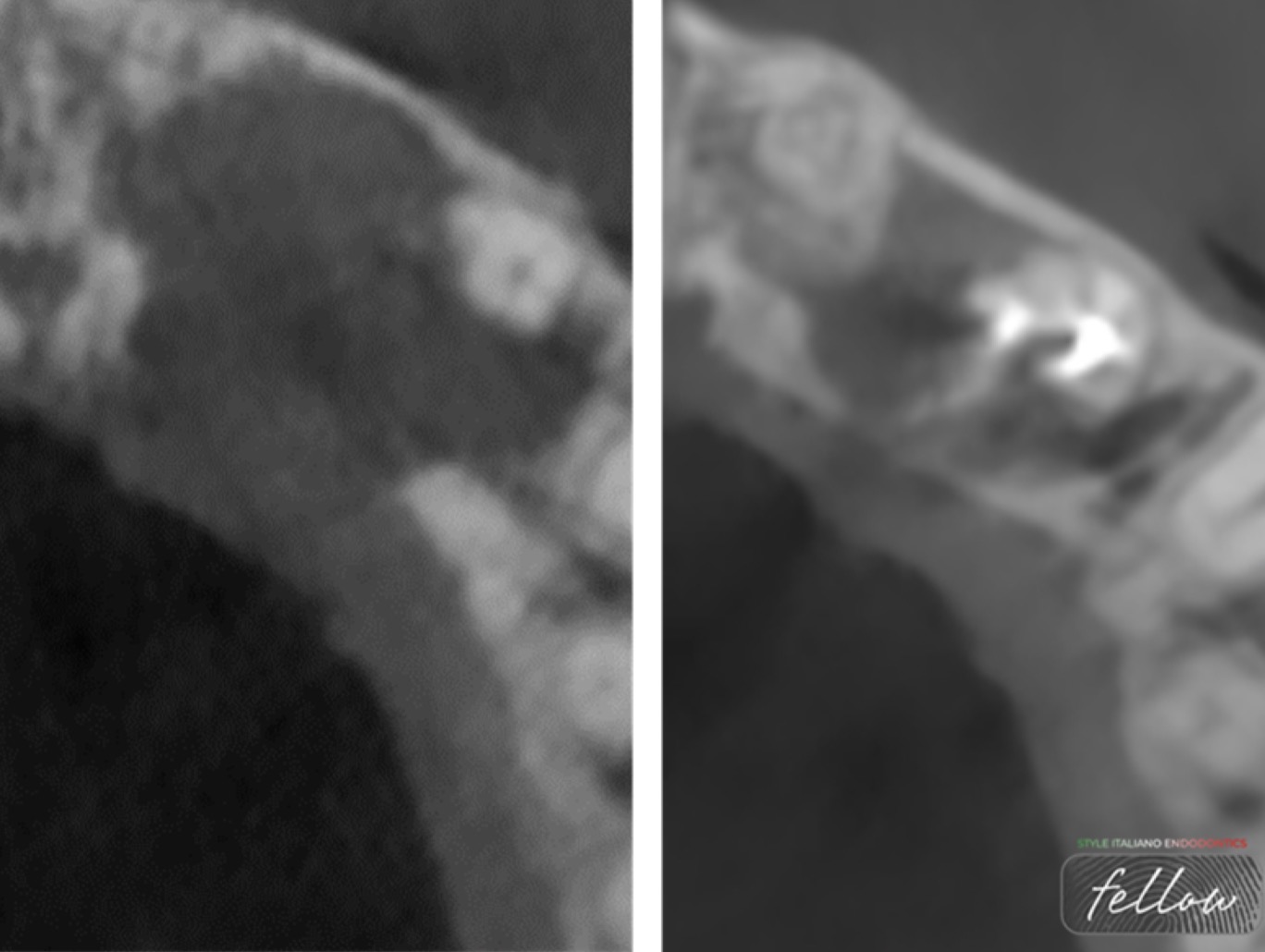
Fig. 12
Follow up one year

Fig. 13
Ali Ayad Gargom. -Graduated in 2012- 2013 from Benghazi University, Faculty of Dentistry. -General practitioner, but most dental work limited to Endodontics especially large lesions related to root apices, perforations, and separated instruments. -Demonstrator in Conservative & Endodontic department, Benghazi University, Dental Faculty since 2016. -Master Degree student in Endodontics. -Former teaching staff in Arab diploma from 2019 to 2021. - Endodontic courses instructor: Basic and advanced ones. -Fellow at Style ItalianoEndodontics.
Conclusions
The issue in teeth affected with dens invaginatus lesions are complex treatment due to the unpredictable internal anatomy of teeth affected with these lesions. However CBCT, modern endodontics and surgical endodontics have improved the management of such anomalies.
Bibliography
1)Alani A, Bishop K. Densinvaginatus. Part I: classification, prevalence and aetiology. Int Endod J 2008;41(12):1123-36.
2)Pindborg JJ. Pathology of the Dental Hard Tissues. Philadelphia:Sauders;1970.
3)Rotstein I, Stabholz A et al. Consideration in the treatment of dense invaginatus. Endod Dent Traumatol 1987;3:249-54.
4)Hulsmann M. Dens invaginatus: Aetiology, Classification, Prevalence, diagnosis and treatment consideration. Int Endod J 1997;30
5)Oehlers FA. Dens invaginatus (dilated composite odontome). I. Variations of the invagination process and associated anterior crown forms. Oral Surg Oral Med Oral Pathol 1957;10(11):1204-18.