Treatment of a dens invaginatus with an apical plug of calcium silicate cement
10/02/2017
The Community
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Introduction
Treatment of young permanent teeth with pulp involvement is an endodontic and restorative challenge. When pulp vitality is lost, the formation of dentin stops, resulting in a tooth with thin dentin walls that is prone to fracture. Traditionally, apexification was performed with calcium hydroxide. It was a lengthy procedure requiring 5-20 months (1) and multiple appointments. During this period, the tooth is restored temporarily and is prone to fracture. In addition, several in vitro studies reported a reduction in the mechanical properties of radicular dentine after exposure to calcium hydroxide for 5 weeks or longer (2).
Mineral Trioxide Aggregate (MTA) was introduced in 1993, and has been studied extensively since that time. It is widely used as an apical barrier in immature, non-vital teeth, as an alternative to calcium hydroxide (3).
It is part of a class of materials known as calcium silicate cements, and is a bioactive material with excellent biocompatibility, antimicrobial properties, with good sealing properties, even in the presence of moisture (4). MTA’s drawbacks include a long setting time, handling properties that some clinicians describe as difficult, and dentin discoloration (3, 4).
Other calcium silicate materials have been developed that can be used for apical barriers. These include Root Repair Material Putty (since 2008 available from Brasseler USA, Savannah, GA as Endosequence RRM Putty, and more recently from FKG Dentaire, Switzerland as TotalFill RRM Putty) and Biodentine (Septanest N, Septodont, France) (5-7). These are also referred to as bioceramics.

Fig. 1
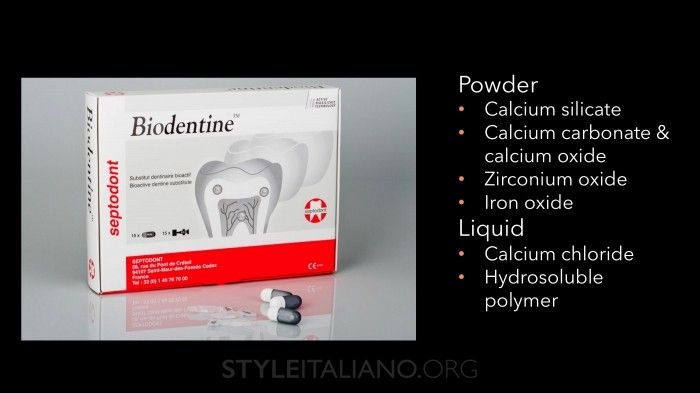
Fig. 2
The new generation bioceramic putties have indications that are similar to MTA, but offer some advantages. In general, they have better clinical handling properties and there have been no clinical reports of staining. Some bioceramic products set faster than MTA. The majority of papers report favorable properties, similar to MTA, including biocompatibility, bioactivity, minimal microleakage and antimicrobial properties (8-10). While in vitro studies are promising, it is not clear if any of these results influence clinical success.
The author’s protocol for placement of an apical barrier of RRM Putty
1. Control the infection with mechanical and chemical debridement of the root canal.
2. Place an inter-appointment dressing of calcium hydroxide.
3. Schedule the patient to return in 3-4 weeks. If the patient is asymptomatic and there are no clinical signs of infection, proceed with treatment.
4. If signs or symptoms remain, or if inflammatory resorption is present, perform additional debridement and irrigation and reapply the calcium hydroxide for another month.
5. If the canal can be dried, place an apical plug.

Fig. 3
6. ERRM Putty is pre-mixed and ready to use. Remove the desired amount of material using a sterile instrument and place the putty on a clean glass slab or dappen dish. The material can be rolled on a glass slab into a firm ball or roll. Immediately after removing the material, place the lid back on the jar so it does not dry out. RRM putty tends to dry out over time. A small amount of BC sealer can be added to the putty to regain its normal consistency.
7. Apply the apical plug in small increments. This can be performed with an MTA carrier, or by taking small increments from the roll with a metal carver and picking them up with a metal plugger.

Fig. 4
8. When the material has been delivered in the middle or apical part of the canal, use thick paper points as a plugger, and gently tap the material in an apical direction.
9. Check the placement of the apical plug with a radiograph.
10. Remove the remnants of the used material from the canal wall with a micro-brush moistened with water.
11. Insert a moist foam pellet on top of the apical plug, apply calcium hydroxide in the remaining part of the canal and temporize the tooth.
12. In a subsequent visit, place one or more fiber posts in a composite core material, cut the posts back 2 mm under the cavo-surface and cover with an universal hybrid composite (11)
Reinforcement of thin root walls
Immature anterior teeth are at risk for root fracture after root canal treatment. Adhesively bonded composite resin restorations extended into the root canal space have been shown to enhance the strength of immature teeth (12). Additional in vitro studies showed that the use of fiber posts improved the fracture resistance of immature teeth significantly more than composite resin alone (13-15). Backfilling the remaining part of the root canal with gutta-percha and sealer resulted in the weakest roots (13-15). The benefit of fiber posts to increase the fracture resistance of pulpless teeth has been reported in numerous studies and recommended by many authors (13-19).
Clinical case
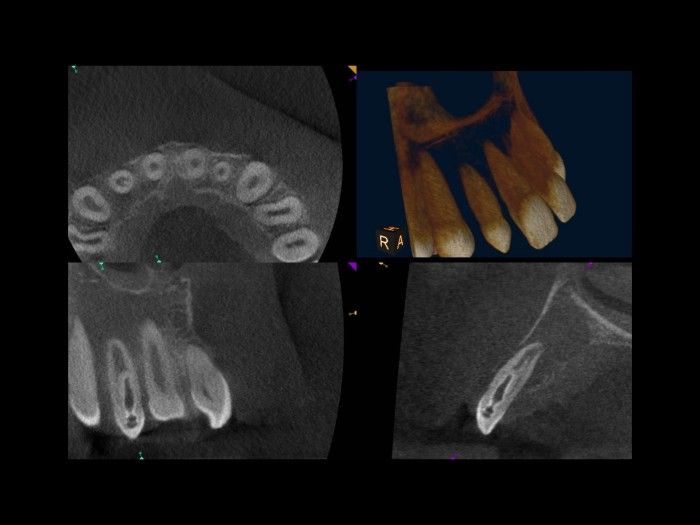
A 12-year old male presented in our office with a swollen face caused by a large submucosal swelling associated with his peg-shaped maxillary right lateral incisor. The medical history was non-contributory. Clinical examination revealed a large swelling that was fluctuant on palpation. Radiographically, the tooth presented as a dens invaginatus Type II according to Oehlers (20) with a peri-apical radiolucency. A cone beam computed tomography (CBCT) scan was ran and revealed the presence of a large radiolucency associated with the tooth. In addition, we had a better three dimensional picture of the aberrant anatomy at out disposal. The diagnosis was acute apical periodontitis. Treatment options were discussed with the patient and his parents, and endodontic treatment was selected.

Fig. 5
At the first emergency treatment session, there was significant drainage of pus after cutting an access opening and removing part of the dens with a diamond bur in a high speed handpiece. Copious irrigation with sodium hypochlorite 5% was carried out and a dressing of calcium hydroxide was placed in the canal.

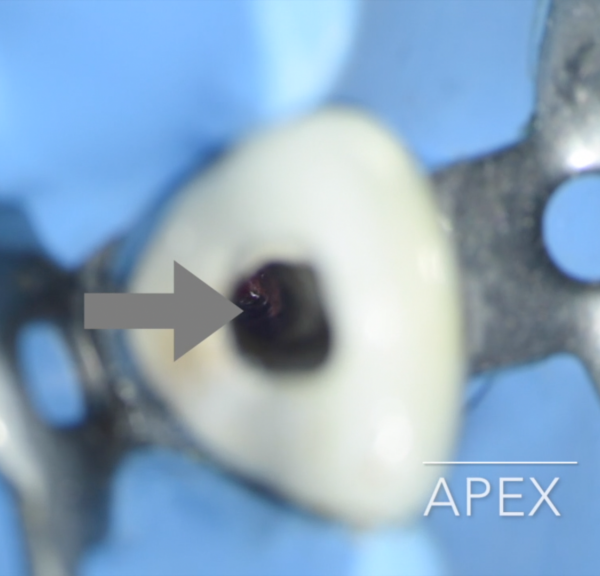
Fig. 6
At the second appointment, one week later, the swelling had disappeared. The remaining part of the dens was removed with Munce Discovery burs, and the canal was gently instrumented with Light Speed instruments. There was still some purulent drainage. We applied calcium hydroxide in the canal and a temporary filling.
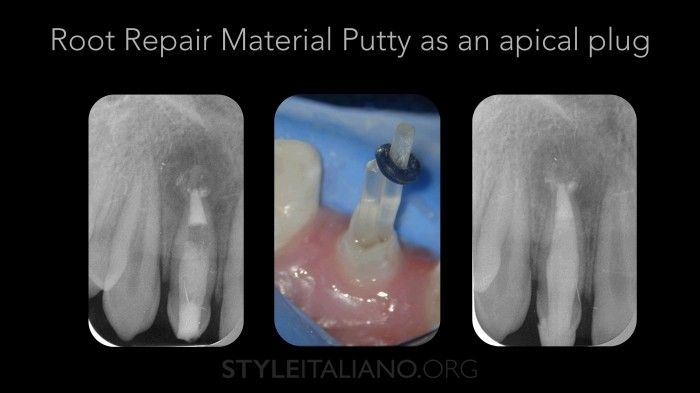
Fig. 7
Six weeks later, the patient was fully asymptomatic. After removing the calcium hydroxide, a dry canal could be obtained and an apical plug of RRM Putty was placed using an MTA carrier and thick paper points. A moist foam-pellet was inserted on top of the putty, and the tooth was temporized again. At the fourth appointment, it was verified if the apical plug of RRM Putty had fully set. To reinforce the thin dentinal walls of the root, 2 fiber posts were placed with a composite core material. Then the patient was referred to a cosmetic dentist for a veneer of composite.

Fig. 8
The 2-year recall radiograph shows a healthy, asymptomatic tooth in full function.
Conclusions
This case shows that placement of an apical plug of RRM Putty followed by an adhesive build-up with fiber posts in a dens invaginatus with a necrotic pulp resulted in a successful treatment outcome with elimination of clinical symptoms and bone healing.
Bibliography
Sheehy EC, Roberts GJ. Use of calcium hydroxide for apical barrier formation and healing in non-vital immature permanent teeth: a review. Br Dent J. 1997 Oct 11;183(7):241-6.
Yassen GH, Platt JA. The effect of nonsetting calcium hydroxide on root fracture and mechanical properties of radicular dentine: a systematic review. Int Endod J. 2013 Feb;46(2):112-8.
Parirokh M, Torabinejad M. Mineral trioxide aggregate: a comprehensive literature review Part III: Clinical applications, drawbacks, and mechanism of action. J Endod. 2010 Mar;36(3):400-13.
Parirokh M, Torabinejad M. Mineral Trioxide Aggregate: a comprehensive literature review Part I: Chemical, physical and antibacterial properties. J Endod 2010 Jan; 36(1): 16-17.
Guven Y, Tuna EB, Dincol ME, Ozel E, Yilmaz B, Aktoren O. Long-Term Fracture Resistance of Simulated Immature Teeth Filled with Various Calcium Silicate-Based Materials. Biomed Res Int. 2016;2016:2863817.
Caronna V, Himel V, Yu Q, Zhang JF, Sabey K. Comparison of the surface hardness among 3 materials used in an experimental apexification model under moist and dry environments. J Endod. 2014 Jul;40(7):986-9.
Bani M, Sungurtekin-Ekçi E, Odaba? ME. Efficacy of Biodentine as an Apical Plug in Nonvital Permanent Teeth with Open Apices: An In Vitro Study. Biomed Res Int. 2015:359275.
Ree MH, Schwartz R. Clinical applications of bioceramic materials in endodontics: Endod Pract, 2014 (7):3240
Rajasekharan S, Martens LC, Cauwels RG, Verbeeck RM. Biodentine material characteristics and clinical applications: a review of the literature. Eur Arch Paediatr Dent. 2014 Jun;15(3):147-58.
Prati C, Gandolfi MG. Calcium silicate bioactive cements: Biological perspectives and clinical applications. Dent Mater. 2015 Apr;31(4):351-70.
Ree M, Schwartz RS. The endo-restorative interface: current concepts. Dent Clin North Am. 2010 Apr;54(2):345-74.
Desai S, Chandler N. The restoration of permanent immature anterior teeth, root filled using MTA: a review. J Dent. 2009 Sep;37(9):652-7.
Schmoldt SJ, Kirkpatrick TC, Rutledge RE, Yaccino JM. Reinforcement of simulated immature roots restored with composite resin, mineral trioxide aggregate, gutta-percha, or a fiber post after thermocycling. J Endod. 2011 Oct;37(10):1390-3. Aug;41(8):685-92.
Brito-Júnior M, Pereira RD, Veríssimo C, Soares CJ, Faria-e-Silva AL, Camilo CC, Sousa-Neto MD. Fracture resistance and stress distribution of simulated immature teeth after apexification with mineral trioxide aggregate. Int Endod J. 2014 Oct;47(10):958-66.
Nikhil V, Jha P, Aggarwal A. Comparative evaluation of fracture resistance of simulated immature teeth restored with glass fiber posts, intracanal composite resin, and experimental dentine posts. ScientificWorldJournal. 2015;2015:751425.
Tanalp J, Dikbas I, Malkondu O, Ersev H, Güngör T, Bay?rl? G. Comparison of the fracture resistance of simulated immature permanent teeth using various canal filling materials and fiber posts. Dent Traumatol. 2012 Dec;28(6):457-64.
Cauwels RG, Lassila LV, Martens LC, Vallittu PK, Verbeeck RM. Fracture resistance of endodontically restored, weakened incisors. Dent Traumatol. 2014 Oct;30(5):348-55.
Dikbas I, Tanalp J, Koksal T, Yaln?z A, Güngör T. Investigation of the effect of different prefabricated intracanal posts on fracture resistance of simulated immature teeth. Dent Traumatol. 2014 Feb;30(1):49-54.
Sivieri-Araujo G, Tanomaru-Filho M, Guerreiro-Tanomaru JM, Bortoluzzi EA, Jorge ÉG, Reis JM. Fracture resistance of simulated immature teeth after different intra-radicular treatments. Braz Dent J. 2015 May-Jun;26(3):211-5.
Oehlers FA. Dens invaginatus (dilated composite odontome). I. Variations of the invagination process and associated anterior crown forms. Oral Surg Oral Med Oral Pathol. 1957 Nov;10(11):1204-18