Practical Minimal Invasive Endodontics
24/08/2020
Warning: Undefined variable $post in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
"Minimally Invasive Endodontics" concept should be case dependent to achieve better outcome. We aim to preserve tooth structure but at the same time we should be able to do that in a repeatable and teachable manner.
Minimally Invasive Endodontics (MIE) concept is becoming popular in the last years, where all of the dentists’ concern is aiming at preservation of tooth structure. Moreover, Single visit root canal treatment (RCT) is becoming more popular and achievable among patients nowadays. Lots of reasons lie behind, such as: new advances in instruments, tools and devices used for RCT, advanced techniques in activation of irrigation for proper disinfection which is considered one of the most crucial steps.
This case report shows how MIE can be achieved easily while keeping in mind that the disinfection of the root canal shouldn’t be compromised even in complex cases.

Fig. 1
A 40 years old male came to our dental clinic seeking for a smile makeover due to protruded upper and anterior teeth. The patient was advised to for orthodontic treatment at first but he refused due to special reasons. The patient decided to go for aesthetic treatment which will be crowning the upper and lower anterior teeth. After one month from doing the smile makeover, the prosthodontist referred the case to my clinic as the patient had severe pain in the lower right quadrant.
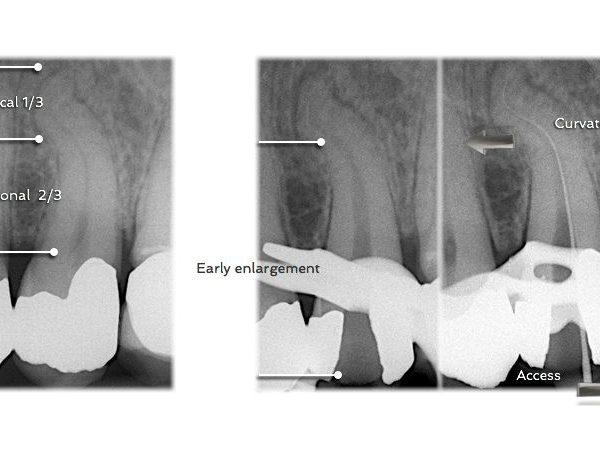
After doing thorough diagnosis, it was concluded that the patient suffered from SAP related to the Lower Right Canine which was crowned as premolar for aesthetic purpose. IOPA radiographs were taken for the lower right canine, which seemed to be a challenging case here due to its long and curved root, thin apical third, not to mention that the patient had a shallow floor of the mouth.
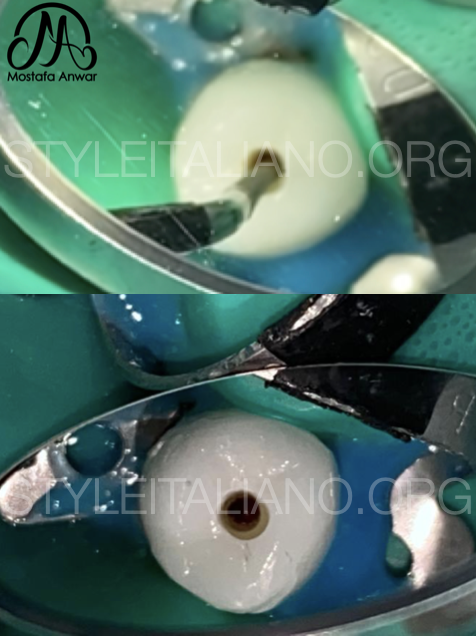
Fig. 2
Root Canal Treatment Procedure:
Before starting the treatment, it was planned that achieving the MIE is crucial to save the crown already cemented to the Canine, starting from the Access cavity till the obturation phase.
All the steps were done under dental operating microscope using the most advanced techniques in all the steps of RCT, while putting the patient’s interest as the main objective. The goal was to preserve the Peri-Cervical Dentin (PCD) as much as practical, where the PCD contributes to the fracture strength of the tooth. PCD is described as the tooth structure of 4 mm above and 4 mm below the crestal bone.
Practical Contracted Endodontic Cavity was done, then flaring of the cavity walls was done using Ultrasonic tips for better visibility, shaping, disinfection and obturation.

Fig. 3
Working length was determined using Apex Locator and it was found to be 27 mm.
The biomechanical preparation was done using controlled memory rotary files up to the working length, where the Master Apical File (MAF) was of size 40/.04. This size would enable proper disinfection either by syringe & needle or any other irrigation activation method specially in case of CEC.
In this case, due to proper choosing of the MAF in terms of Tip size & Diameter, achieving proper disinfection was maintained using a 30G side-vented needle for irrigation which could reach the desired length at the apical third.
After that, cycles of ultrasonic activation of the irrigant before the curvature were done. Sonic activation was used below the curvature.

Fig. 4
Master Cone radiograph was taken of the same size as the MAF, up to the working length.

Fig. 5
Obturation was done using Synchronized Hydraulic Condensation technique using BioCeramic sealer and the master cone only. This technique is easily done specially in cases of severe curvatures or double curvatures.
Composite restoration was adapted into the CEC at the same visit.
Conclusions
This clinical case showed us that MIE concept can be applied but its a case dependent scenario. Canal disinfection is the ultimate goal and its the main step where reduction of intra-canal bacteria could be achieved.
Preserving of tooth structure is important but not on the expense of any iatrogenic errors like missed canals, improper disinfection or mechanical preparation errors.
Bibliography
- Anil Kishen et al, 2015. “Contracted endodontic cavities: the foundation for less invasive alternatives in the management of apical periodontitis”. Endodontic Topics.
- Plotino et al, 2017. “Fracture Strength of Endodontically Treated Teeth with Different Access Cavity Designs”. Journal of Endodontics.
- Lee et al, 2019. “Influence of apical preparation size and irrigation technique on root canal debridement: a histological analysis of round and oval root canals”. International Endodontic Journal.
- Kulild et al, 2014. “Master apical file size – smaller or larger: a systematic review of healing outcomes”. International Endodontic Journal.