Endodontic management of mandibular canine with two roots and two canals
17/07/2020
Khalid Jamal Attar
Warning: Undefined variable $post in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
The aim of endodontic treatment is to eliminate microorganism infection from the root canal system and prevent reinfection.[1]
Successful Endodontic treatment depends upon Adequate knowledge about the morphology of root canal system and diagnosing the anatomic variants to avoid missed canals, Therefore, the clinician should be aware of any anatomical variations which may alter the prognosis for root canal therapy.Usually, mandibular canine has one root with a single root canal . Further incidence which showed that 98.3% of these teeth presented with a single root, 92.2% presenting with one canal and one foramen, 4.9% with two canals and one foramen, and 1.2% with two canals and two foramina,the incidence of two-rooted canines was as low as 1.7%. [2]

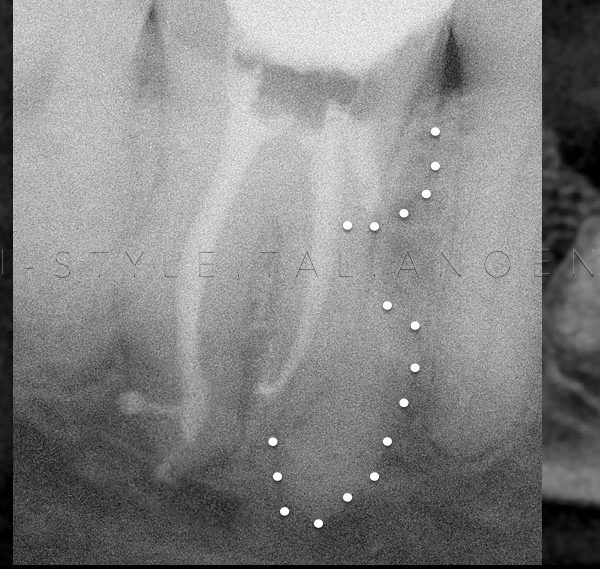
Fig. 1
A 35-year-old female came to our dental office with severe pain in the right mandible.
The pain disturbed her sleep and lingered for several minutes.
Clinical examination revealed tooth 43 with composite restoration, her tooth was tender to percussion and no response to the electric pulp test.
Intraoral periapical radiograph showed that the tooth was with large filling restoration closed to pulp chamber tissue with suspected two roots.
A clinical diagnosis of chronic irreversible pulpitis with symptomatic apical periodontitis was made and root canal therapy was recommended.
Local anesthesia with epinephrine was introduced through infiltration, then the rubber dam was placed for isolation.
After removal of old restoration and deep caries with high-speed endo access bur No.1(Dentsplysirona.USA), the pulpal floor was carefully examined with dental operating microscope Zumax (Zumax Medical Ltd, china).
Two separated buccal and lingual orifices were identified.

Fig. 2
The access cavity outline was extended bucco-lingual to establish straight-line access .
The working length was established with no.10 k-file using electronic apex locator Root ZX II (J. Morita, Tokyo, Japan) and confirmed radiographically.

Fig. 3
The canals were prepared firstly by flaring with One Flare from(Micro-mega ,France ) and then cleaning the canals from pulp tissue and debris by normal saline after that start to complete shaping with 2shape files rotary system to all working length Ts1,Ts2 (Micro-mega,France) and copious irrigation was carried out during the instrumentation phase with 5.25%(NAOCL).
Periapical radiograph was taken to confirm working length with gutta percha cone , final rinsing is 5.25% sodium hypochlorite (NAOCL) with ultrasonic activation UltraX device Eighteeth (Changzhou Sifary Technology Co.,Ltd,china) for 30second followed by 17% (EDTA) for 1 minute with safe 2-side vents irrigation tips IrriFlex (Produits Dentaires,Swizterland) (Figure3).
The obturation was achieved by cold lateral compaction technique with BC sealer (Meta-Biomed,Korea ).

Fig. 4
Irriflex can penetrate immediately at the same level of mechanical preparation. Its flexibility ensures a smooth penetra inside the canal.
30G, 4 % taper, 27 mm long,
Soft polypropylene body
Back-to-back 2-side vent design
Needle fully transparent to improve user comfort and liquid delivery precision Slightly pre-bendable to meet specific irrigation requirements

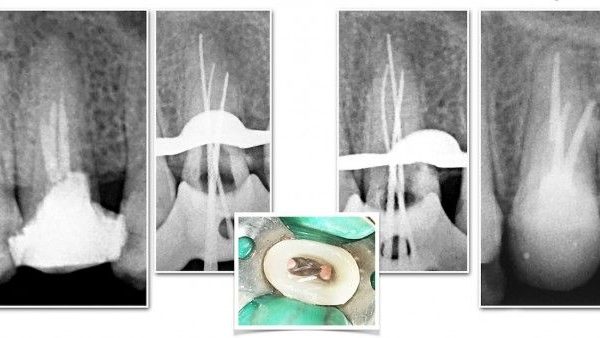
Fig. 5
Post obturation radiographs showed two well obturated canals ending at radiographic apex and the pulp chamber was cleaned by air abrasion with water then final restoration was done (Figure 4).

Fig. 6
Outcome was satisfactory and subside patient's discomfort.
The patient was advised to receive a full coverage restoration when he returned for his 1-month follow-up visit.
Conclusions
Although the probability of permanent mandibular canine has extra roots and root canals are infrequent, the clinicians should suspect any anatomical variations in these teeth. Careful interpretation of conventional radiographs, appropriate access cavity design to visualize the entire pulp chamber floor as well as the use of magnifying tools are helpful to evaluate complex root canal anatomy .
Bibliography
Pécora JD, Sousa Neto MD, Saquy PC. Internal anatomy, direction and number of roots and size of human mandibular canines. Braz Dent J 1993;4:53-7.
Sjogren U, Hagglund B, Sundqvist G, Wing K. Factors affecting the long-term results of endodontic treatment. J Endod 1990;16:498-504. Back to cited text no.