Bioceramic sealers application: the ultimate guide
25/11/2021
Riccardo Tonini
Warning: Undefined variable $post in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /var/www/vhosts/styleitaliano-endodontics.org/endodontics.styleitaliano.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
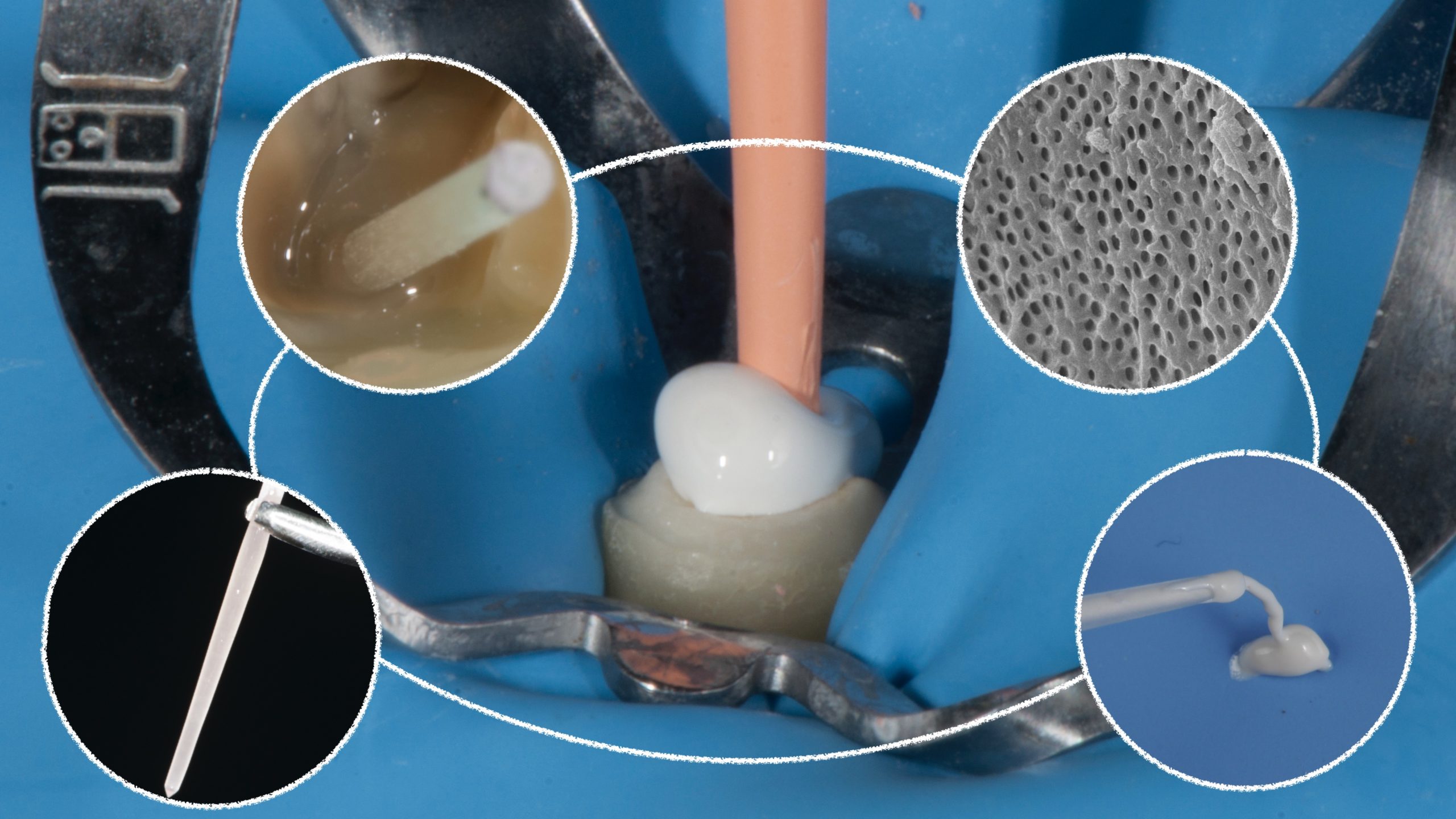
Warm and cold Gutta percha in combination with various types of root canal sealers have been considered the dominant techniques since the mid nineteenth century. With the advent of Bioceramic premixed sealers, maybe a new era started, but first of all a new trend has been established. All these kind of sealers should be extruded by a needle, usually conical, made in polymer and with different sizes on the basis of the consistency of sealers. This bundle syringe and needle is a beautiful format to see during expo, because in a single step one could ideally solve many matters that clinician has to face, like achieving perfect sealer consistency during preparation, deliver sealer from tray to the canals, saving time and ergonomics. Unfortunately, when a clinician has to work on a patient, he discovers that this format opens the door to other problems, like overfilling, under filling and material waste.

Fig. 1
This is a typical examples of uncontrolled extrusion. The clinician was expecting a feedback from the canal during sealer application made with syringe, but unfortunately only the final X-ray highlighted the clinical matter. In terms of symptoms both cases were completely asymptomatic during the following days.

Fig. 2
Due to this uncertain situation, some clinician suggested to come back to the origin with paper points or lentulo models, but honestly the concept is like unaccepting the evolution and in any case both concepts still leave risks for the clinician, like dehydration of sealer made by paper points and lentulo breakage.

Fig. 3
This is the reason why a new application technique has been designed basing on two different models:
- Plastic carrier as applicator
- Modified Irriflex Needle
Plastic carrier applicator
This techniques is the easiest:
- Extrude just coronally 3mm of sealer with the needle that comes in the box
- Distribute on the walls the sealer moving plastic carrier close to the WL.
- Introduce GP cone inside the canal
- Make the desired GP technique, Warm or Cold.
Modified Irriflex needle Technique
This technique requires a bit more training made by the operator and it is made in this way:
1) Apply irriflex to the Bioceramic sealer needle
2) Place a rubber stop on Irriflex
3) Cut last 2/3 mm of the needle
4) Adjust the rubber stop 1mm shorter than wl
5) check sealer extrusion on rubber dam
6) extrude sealer in the first 4 mm of the canal
7) stop extrusion when sealer appears at orifice level
8) introduce irriflex inside the canal without further material extrusion and move the needle by side in order to distribute sealer on the walls (NO UP AND DOWN MOVEMENTS)
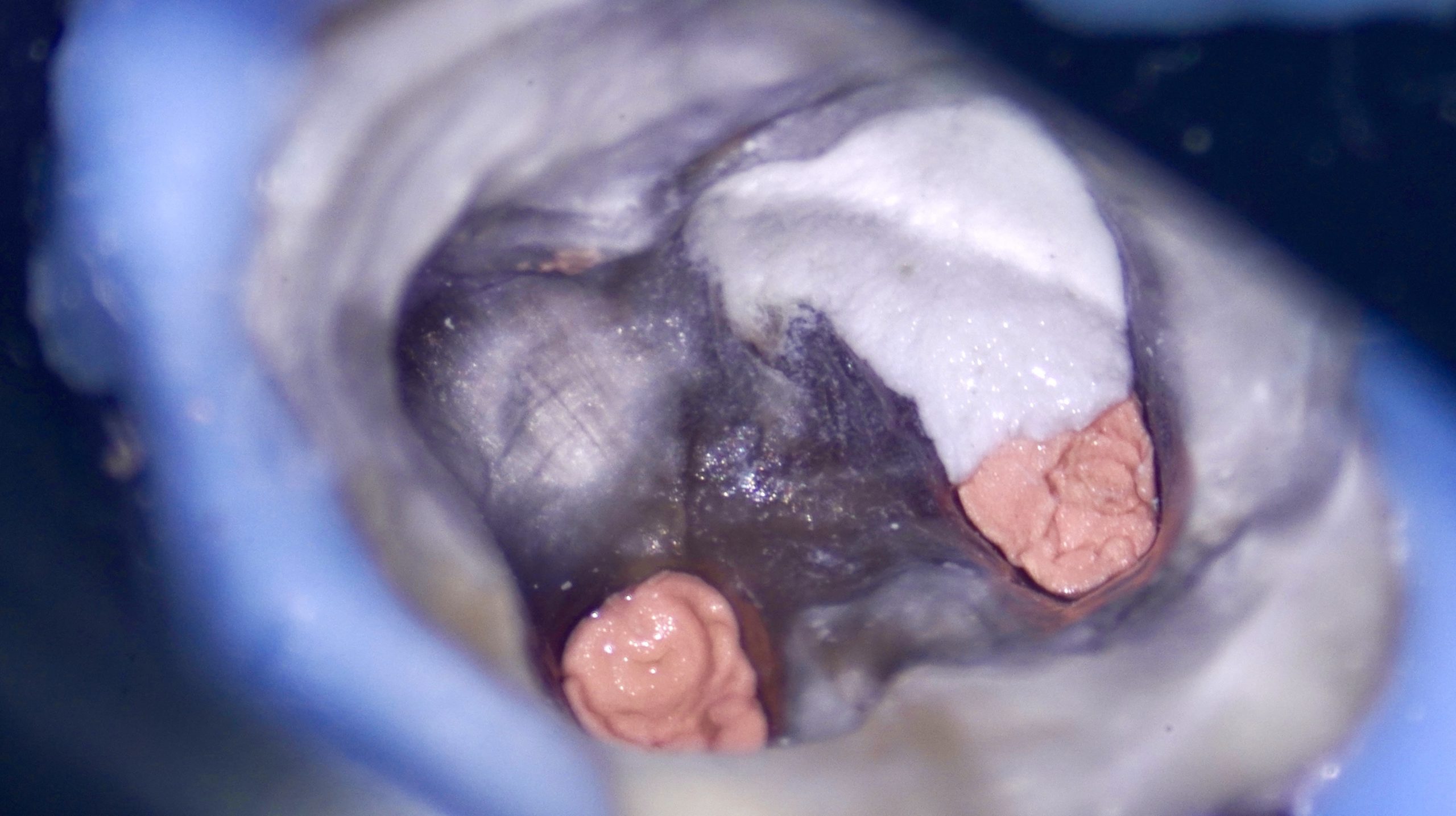
9) before introducing GP cone make sure that no more sealer is in the middle of the coronal third. It must look like a black hole with white circumference.
10) introduce GP cone and make your preferred technique
REMEMBER: LESS MATERIAL WASTE WITH THIS NEEDLE
In case of carrier based technique, the operator can use both techniques, but it’s suggested to distribute the sealer just in the coronal /mid part of the canal. Also here the canal must be empty in the central part in order to avoid GP blockage at the coronal level
Conclusions
A new material can become a fast trend in dentistry, but even if it’s a promising one, the operator should carefully evaluate also the operative technique. It’s not fair pretend that all operators will be able tu use it since the beginning in proper way. The two techniques here suggested has been developed with hundreds trials until good outcomes has been obtained
Bibliography
Schilder H (1967) Filling canals in three dimensions. Dent Clin North Am, 724-53.
Roggendorf MJ, Ebert J, Petschelt A, Frankenberger R (2007) Influence of moisture on the apical seal of root canal fillings with five different types of sealer. Journal of Endodontics 33(1), 31-33.
Akcay M, Arslan H, Durmus N, Mese M. Capar ID (2016) Dentinal tubule penetration of AH Plus, iRoot SP, MTA Fillapex, and GuttaFlow Bioseal root canal sealers after different final irrigation procedures: A confocal microscopic study. Lasers in Surgery and Medicine 48(1), 70-76.
Al-Haddad A, Ab Aziz C, Zeti A (2016) Bioceramic-based root canal sealers: a review. International Journal of Biomaterials, 2016.
Camilleri J (2011) Characterization and hydration kinetics of tricalcium silicate cement for use as a dental biomaterial. Dental Materials 27(8), 836-844.
Camilleri J (2015) Sealers and warm gutta-percha obturation techniques. Journal of Endodontics 41(1), 72-78.