

Revascularization - 6 years follow up
09/07/2020
Fabio Gorni
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
One of the main objective in case of incomplete root formation is to re-establish the blood flow allowing the continuation of the root development. Nowadays, the revascularization technique is an alternative to the traditional apexification using calcium hydroxide for a period of time in order to induce a formation of calcified apical barrier .
Infection control seems to be crucial for success of revascularization , most of the studies are using as medication TAP ( triple antibiotic paste ) Metronidazole - Mynociclin - Ciprofloxacin , but not always without long-term complications as discoloration , for this reason the use of calcium idroxide has been preferred . No consensus at the moment on the best protocol to follow , more studies are necessary to evaluate long term efficacy and the role of the new approaches.
The revascularization technique can be applied using different protocols: in this article we want to describe a case of pulp regeneration using Platelet - Rich - Plasma and calcium hydroxide in the first step of the decontamination.
A 9 yrs old male came to my office due to a trauma he had some months before. The involved tooth was a non vital immature permanent upper incisor: the intra-oral examination showed swelling and sinus tract, wile radiographic examination showed open apex with incomplete root formation and thin dentin walls.
After the isolation with rubber dam, the access cavity was performed. The pus drawn out, then canal was irrigated with saline solution, followed by sodium hypochlorite and ultrasonic activation UAI (Irrisafe US Tips - Acteon Satelec - France).
The canal was dried with micro suction aspirator and paper points, after that a calcium hydroxide past was applied in the canal with a lentulo spiral.
After one month , in a second appointment , the canal was irrigated with saline solution and the periapical tissue , beyond the apex , instrumented with manual files to encourage the bleeding. Afterwards a fibrin sponge was inserted in the apical one third 3-4 mm to the foramen to allow blood clot formation . After few minutes the protocol was followed by the application of the PRP gel over the clot . A flow composite temporary filling closed the access .
After one year from the the PRP application we decided to finish the treatment closing the middle one third with an MTA apical plug .
The tooth was restored with a back packing with gutta-percha and composite.
The different radiographic follow-ups are showing a complete reconstruction of the apical anatomy and healthy periapical tissues.

Fig. 1
the fistula is located in the border between the attached gengiva and mucosa.
in the pre-op x-rays is clear the periapical lesion and the immature apex , the root walls are very thin with a reverse anatomy of the apical one third of the root
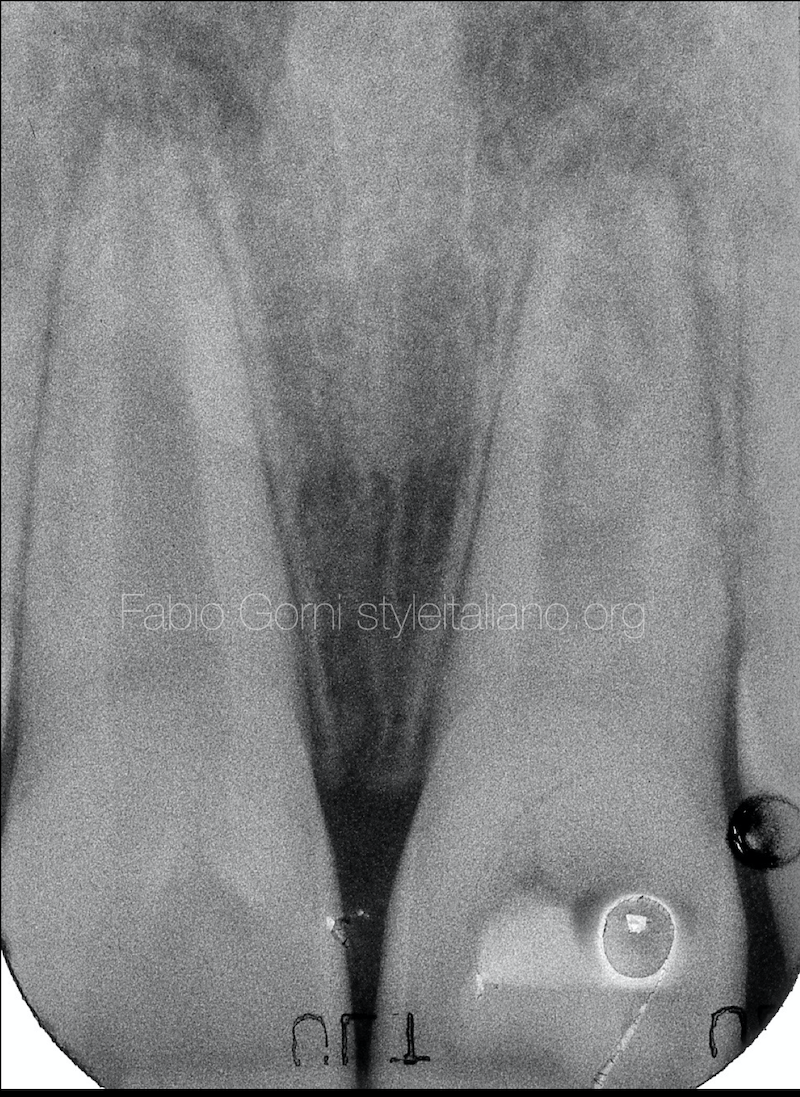
Fig. 2
After 6 months the x-ray shows a different situation, the lesion is healing and the root walls are thicker

Fig. 3
After 12 months the lesion is healed and the apex is going to complete its growth, the root is longer and the tooth looks like the other central incisor

Fig. 4
intra-op x-ray after the application of the MTA , the material was placed over an area of reactive hard tissue located in the middle one third of the root

Fig. 5
Post operative x-ray.
The endodontic treatment has been finalized by a back packing with warm gutta-percha and a final restoration in composite
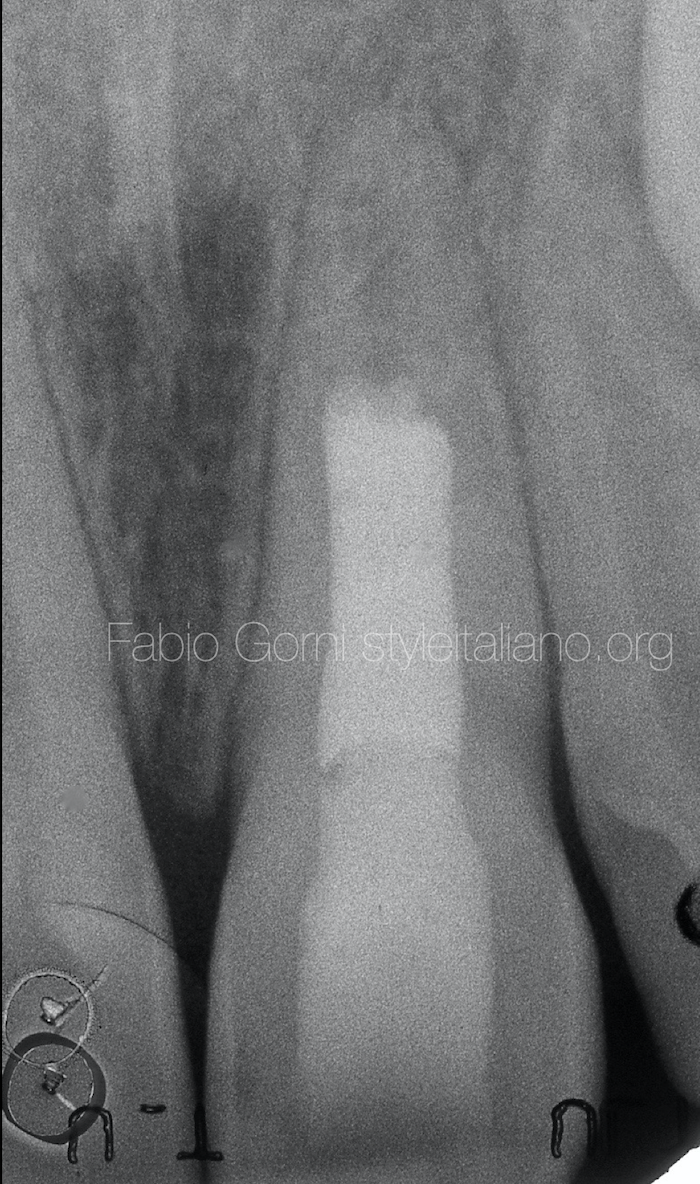
Fig. 6
2 years follow up.
The situation is stable , the periapical tissue is healthy and the tooth has completed its growth

Fig. 7
4 years follow up

Fig. 8
6 years follow up. The radiologic situation shows a perfect continuity of the ligament, the apex looks normal according to the classic anatomy of an adult central incisor
Conclusions
Regenerative procedures constitute an emerging field in Endodontics, because the importance of the root formation is a strategic point in dentistry. Some authors seem opposed to apply the revascularization in infected, non vital immature teeth because it would be too risky trying to revascularize an infected root canal system. We disagree: pulp cells that survived infection can proliferate under the influence of the Hertwig’s epithelial root sheath even during the necrosis inflammation process.
Bibliography
Bakhtiar H, Esmaeili S, Fakhr Tabatabayi S, Ellini MR, Nekoofar MH, Dummer PM. Second-generation Platelet Concentrate (Platelet-rich Fibrin) as a Scaffold in Regenerative Endodontics: A Case Series. J Endod. 2017;43(3):401-8.
Conde MCM, Chisini LA, Sarkis-Onofre R, Schuch HS, Nor JE, Demarco FF. A scoping review of root canal revascularization: relevant aspects for clinical success and tissue formation. Int Endod J. 2017;50(9):860-74.
Estefan BS, El Batouty KM, Nagy MM, Diogenes A. Influence of Age and Apical Diameter on the Success of Endodontic Regeneration Procedures. J Endod. 2016;42(11):1620-5.
Keswani D, Pandey RK. Revascularization of an immature tooth with a necrotic pulp using platelet-rich fibrin: a case report. Int Endod J. 2013;46(11):1096-104.


