

A complex trauma with pulpal exposure: the digital alternative
22/02/2017
The Community
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Traumatic injuries are increasing in the last few years, particularly in young people. When the trauma causes a pulpal exposure, it’s mandatory to avoid pulpal necrosis, particularly in teeth that have an open apex. The pulp capping procedures are quite simple and easy to accomplish but a proper coronal protection by adhesive restoration should be considered as soon as possible.
CAD/CAM indirect restoration are suitable solution for teeth in which a huge part of dentine and enamel tissues were missing.
In the following case a paradigmatic example has been presented.

Fig. 1
A young boy, aged 10, is checking in for an emergency regarding a traumatic lesion on a front tooth during a fight in the courtyard.

Fig. 2
The fracture of tooth 2.1 is complicated by a wide pulp exposure. Patient does not refer pain and trauma happened approximately two hours before. The fragment of the injured tooth is missing. No rx signs of horizontal fractures are evident in the X-Ray taken with the long cone technique. The apex of the tooth is not completely matured.
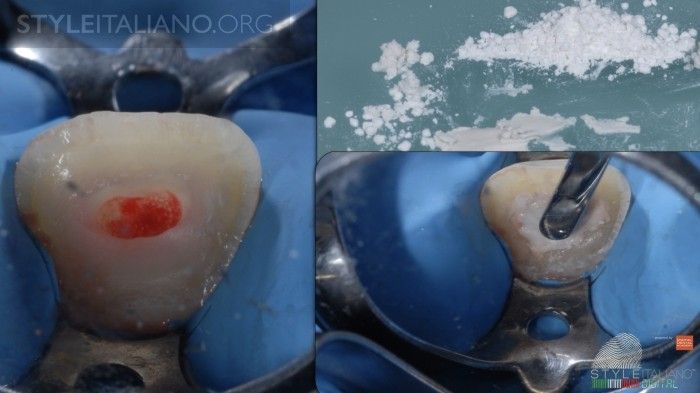
Fig. 3
Following local anesthesia, we executed a pulpotomy and then a complete sealing of the remaining pulp using a calcium silicate cement (Tech Biosealer Capping- Isasan), a medication indicated for direct pulp capping.

Fig. 4
During the same visit, after the residual pulp sealing, the endodontic access cavity is closed using a composite resin (SE Bond Kuraray + Tetric Flow Ivoclar Vivadent). Always during the same visit, after a professional cleaning session….
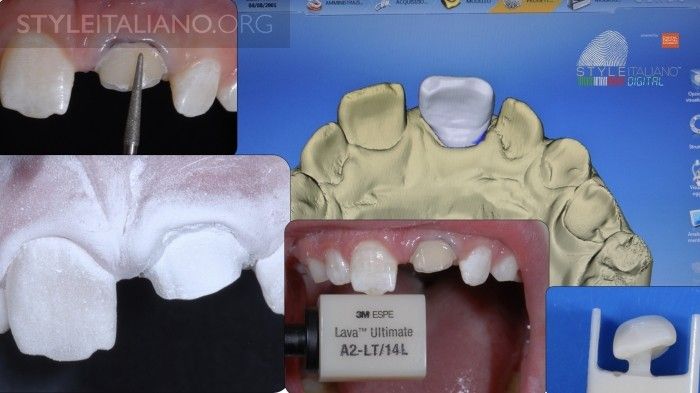
Fig. 5
...the fractured tooth was prepared using the most conservative method, and an optical impression is taken using Sirona Blue Cam 4.2. This way we receive a proposal of an overlay that is sequentially milled in Lava 3M and immediately cemented using an adhesive technique (SE Bond - Kuraray + Tetric Flow - Ivoclar Vivadent)

Fig. 6
The clinical steps of the adhesive cementation of the overlay in LAVA 3M. One can appreciate the final trimming, polishing and characterization of the overlay before the luting procedure

Fig. 7
Radiographic and photographic check after one week followinghte adhesive cementation.

Fig. 8
Radiographic and photographic check after one week following the adhesive cementation.

Fig. 9
Radiographic and photographic check after 4 years. The apex of the 2.1 is perfectly closed and the tooth is answering positively to all the pulpal vitality tests. It will be restored using a lithium disilicate onlay.
Conclusions
CAD/CAM indirect restoration has been employed to solve these functional and esthetic problems in a young boy who experienced a heavy dental trauma in anterior upper incisors; by an indirect adhesive machined composite veneer the tooth has been reconstructed with a proper shape and a guaranteed durability.
Bibliography
Andreasen FM, Kahler B. Diagnosis of acute dental trauma: the importance of standardized documentation: a review. Dental traumatology : official publication of International Association for Dental Traumatology 2015;31(5):340-349.
Bakland LK, Andreasen JO. Will mineral trioxide aggregate replace calcium hydroxide in treating pulpal and periodontal healing complications subsequent to dental trauma? A review. Dental traumatology : official publication of International Association for Dental Traumatology 2012;28(1):25-32.
Borkar SA, Ataide I. Biodentine pulpotomy several days after pulp exposure: Four case reports. Journal of conservative dentistry : JCD 2015;18(1):73-78.
Caprioglio A, Conti V, Caprioglio C, Caprioglio D. A long-term retrospective clinical study on MTA pulpotomies in immature permanent incisors with complicated crown fractures. European journal of paediatric dentistry : official journal of European Academy of Paediatric Dentistry 2014;15(1):29-34.
Griffin JD, Jr. Utilizing bioactive liners. Stimulating post-traumatic dentin formation. Dentistry today 2012;31(10):132, 134-136.
Gudkina J, Mindere A, Locane G, Brinkmane A. Review of the success of pulp exposure treatment of cariously and traumatically exposed pulps in immature permanent incisors and molars. Stomatologija 2012;14(3):71-80.
Koch KA, Brave DG. Bioceramics, Part 2: The clinician's viewpoint. Dentistry today 2012;31(2):118, 120, 122-115.
Lam R. Epidemiology and outcomes of traumatic dental injuries: a review of the literature. Australian dental journal 2016;61 Suppl 1:4-20.
Lauridsen E, Hermann NV, Gerds TA, Ahrensburg SS, Kreiborg S, Andreasen JO. Combination injuries 1. The risk of pulp necrosis in permanent teeth with concussion injuries and concomitant crown fractures. Dental traumatology : official publication of International Association for Dental Traumatology 2012;28(5):364-370.
Martens L, Rajasekharan S, Cauwels R. Pulp management after traumatic injuries with a tricalcium silicate-based cement (Biodentine): a report of two cases, up to 48 months follow-up. European archives of paediatric dentistry : official journal of the European Academy of Paediatric Dentistry 2015;16(6):491-496.
Moule A, Cohenca N. Emergency assessment and treatment planning for traumatic dental injuries. Australian dental journal 2016;61 Suppl 1:21-38.
Pini NI, Nagata JY, Sundfeld-Neto D, Correr-Sobrinho L, Soares A, Aguiar FH, et al. Reestablishing Biology, Function, and Esthetics for Fractured, Immature Incisors. Operative dentistry 2015;40(4):341-349.
Vidal K, Martin G, Lozano O, Salas M, Trigueros J, Aguilar G. Apical Closure in Apexification: A Review and Case Report of Apexification Treatment of an Immature Permanent Tooth with Biodentine. Journal of endodontics 2016;42(5):730-734.