Removal of separated files; More than one way to achieve.
28/02/2024
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Fractured endodontic instruments visualized on the initial radiograph of a case that calls for retreatment may pose a great challenge to the clinician who is being asked to undertake an already complicated task.
Conventional conservative management of separated instruments includes attempts to remove or bypass the fragment, or prepare and fill the root canal system to the coronal level of the fragment. The American Association of Endodontists publication “Broken Instruments - Clinical decision making algorithm”, specifies that the treatment plan needs to take into account not only mechanical aspects (type of alloy, length of fragment, position in the root canal), but also biological ones (level of infection, level of preparation before the incident of fracture).
In cases of endodontic treatment revision due to persisting symptoms and/or periapical lesions, removal of the fragment, when indicated, may be considered as the optimal approach as it reduces contaminated content within the root canal, removes the risk of friction (and thus new fracture) of the rotary instruments during root canal preparation, and enables better adaptation to the walls of the final obturation materials.
This procedure requires not only adequate illumination and magnification to detect the coronal part of the broken file, but also experience and expertise to avoid excessive removal of dentine, which can jeopardize tooth integrity. Occasionally, versatile thinking and resourcefulness may be required to make the most of a wide range of armamentarium readily available for this scope, or to improvise on or modify existing techniques to accomplish this goal.
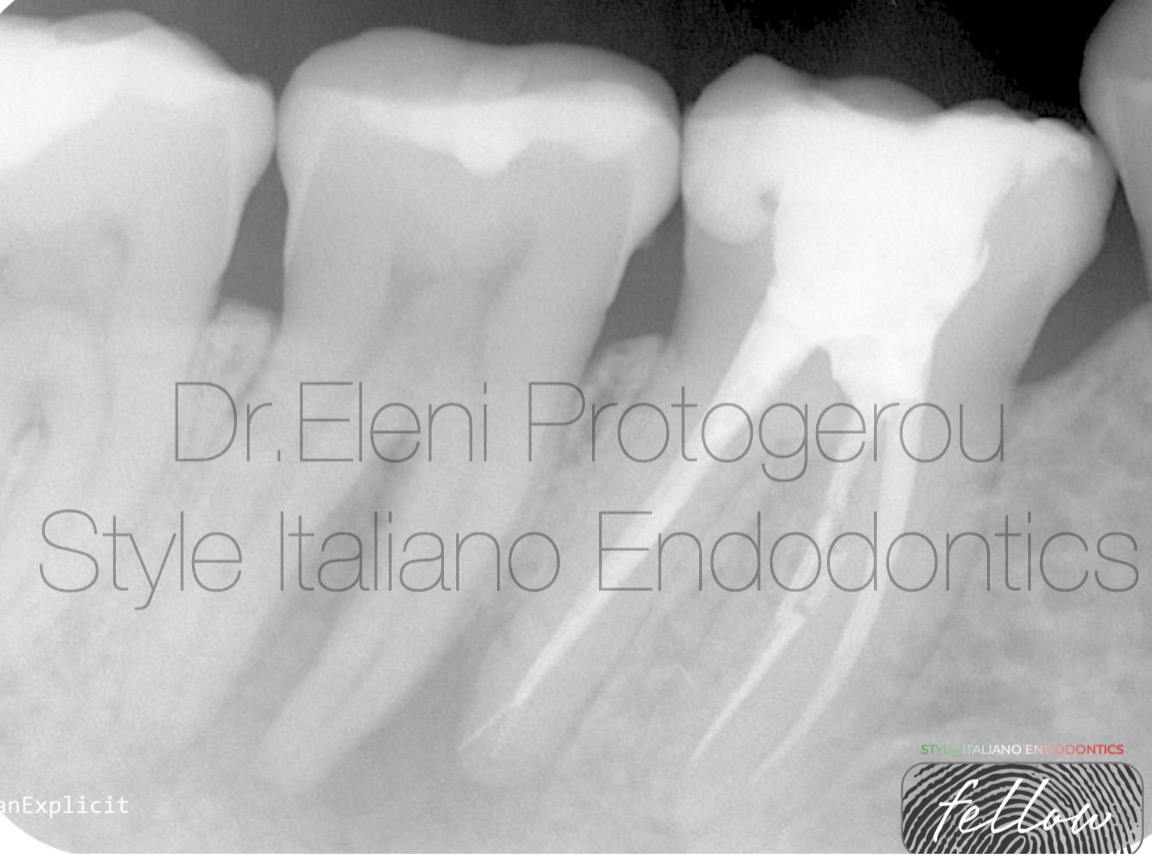
Fig. 1
Figure 1
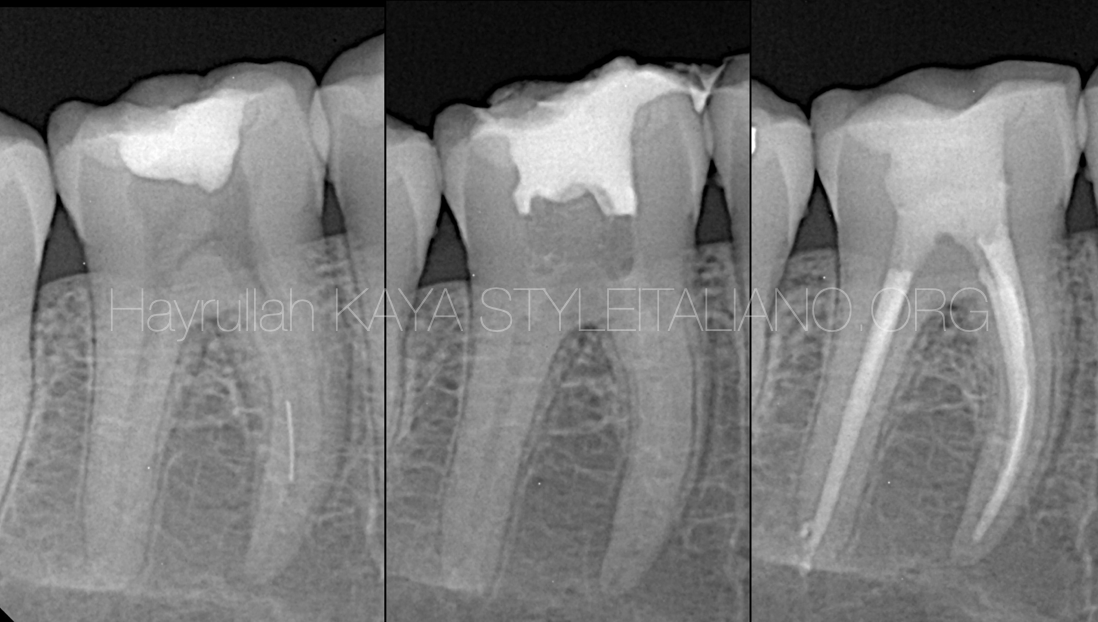
37 year-old female patient with non-contributory medical history was referred for root canal retreatment of tooth 46.
Dental records report acute pain and swelling on right lower jaw 3 months ago, for which Amoxicillin (1gr per 12 hours for 1 week) was prescribed by her dentist. Since then no other major pain incident reported aside for slight sensitivity on percussion. Initial radiograph (Figure 1) suggests a large periradicular lesion related to the distal root apex. Two fragments of endodontic files are evident in the mesiobuccal root canal, and one small fragment in the distal root possibly located into an apical split.
After inferior alveolar nerve block with mepivacaine, the tooth was isolated and careful removal of the occlusal composite filling was performed until gutta-percha was revealed in the three root canal orifices (mesiobuccal, mesiolingual, distal).
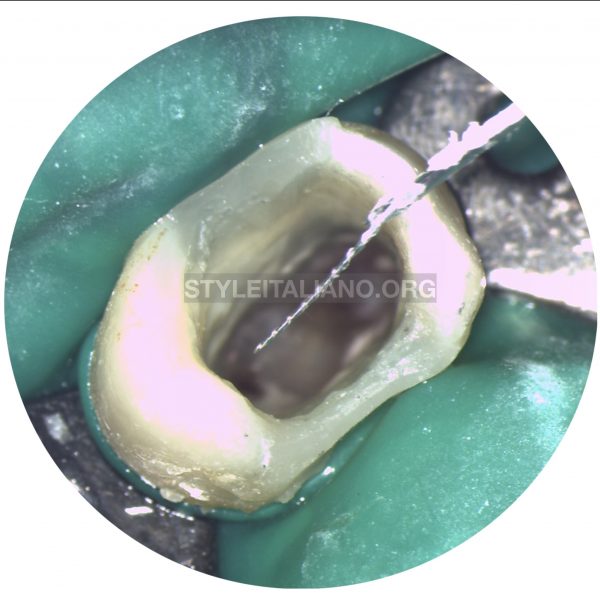
Mesiobuccal root canal was already enlarged, possibly in an attempt to remove the fragments. Ultrasonic tip ET20 (Satelec, Acteon Group, France) was used to remove lingual dentine overhangs, so as to obtain an improved visualization of the coronal stainless steel fragment. The fragment was then gradually released and removed, using the ultrasonics in a counterclockwise motion.
The same tip was used to release the coronal 2mm of the apically broken Niti file. Because those files are prone to fracture at the point of contact with the ultrasonic vibration, it is vital to avoid constant touch of the coronal part of the fragment and use a lower power mode during dentine removal at the circumference. In addition, it is preferable to use a grasping tool when the right time comes. In this case, EndoCowboy (Köhrer Medical Engineering GmbH, Germany) was used with a 0.12 lasso tip to grab and retrieve this fragment.

Fig. 2
Figure 2 shows the cone fitting after removal of instruments in the mesiobuccal root canal. A fragment of small size probably 8 or 10 is evident in the mesiolingual canal at the apical third, which has been by-passed by the cone.
Cone fitting is still not ideal and in the distal root canal the guttaperhca cone is short of the apex, despite the fact that the apex locator (ipex II, NSK, NAKANISHI INC, Japan) gave signal at this point, possibly due to the apically located small metallic fragment distal to the main canal.
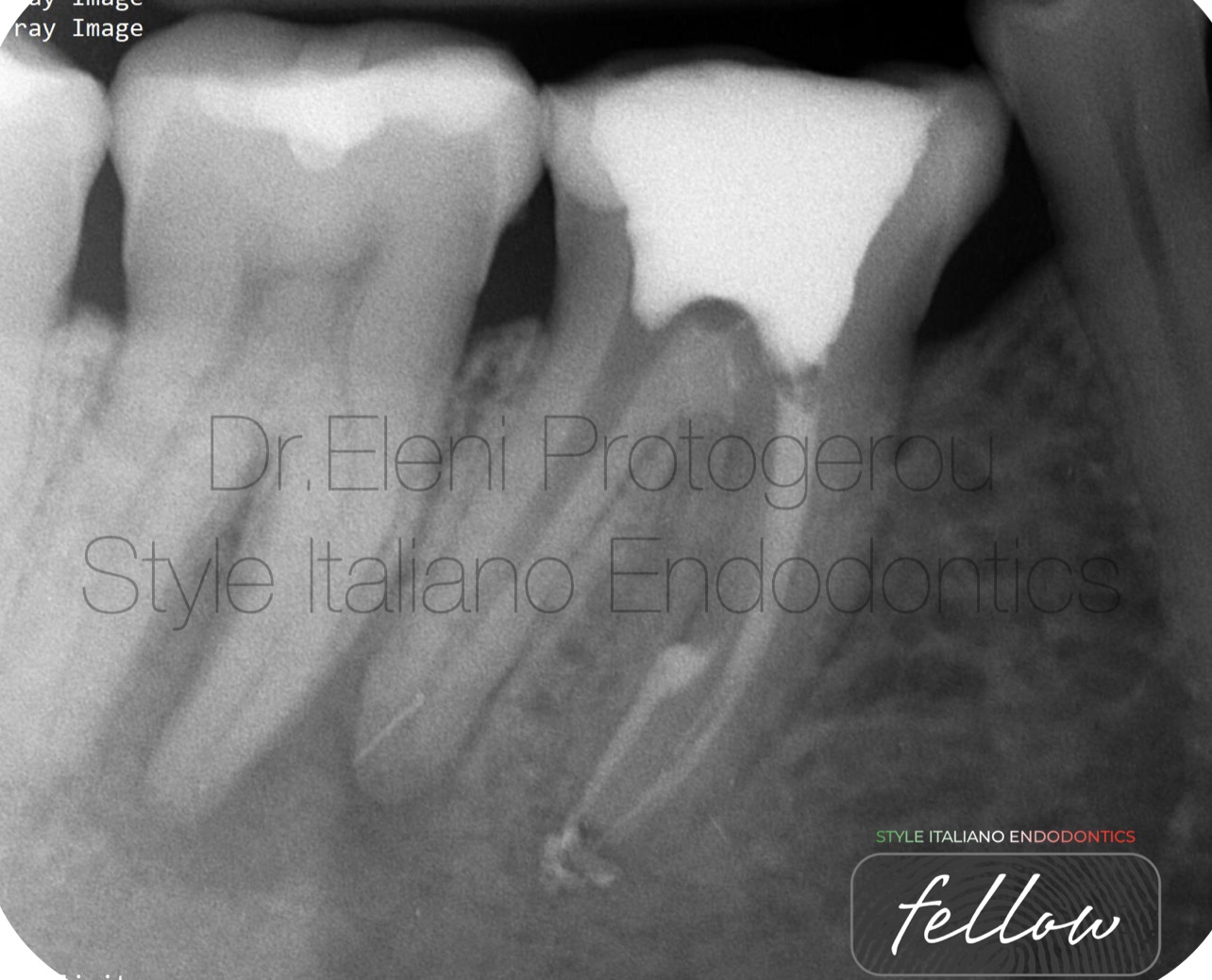
Fig. 3
Figure 3
At this point, final obturation of the mesial root canals with warm vertical compaction technique and AH plus sealer was performed, while in the distal root canal the apical fragment is clearly depicted.
With an ultrasonic tip enlargement of the distal root canal to a lingual direction was carefully done and the coronal tip of the instrument became evident. To avoid further enlargement of the distal canal an XP-endo Finisher (FKG Dentaire, Switzerland) at 1000 rpm speed was used at working length with small coronally directed strokes.

Fig. 4
Figure 4
The fragment was finally dislodged and removed. At this point, obturation of the mesiolingual canal was revisited due to some voids and cone fitting for the distal canal was checked.
In an attempt to compensate for the pre-existing loss of dentin, the middle and coronal part of the mesiobuccal canal were filled with Biodentine (Septodont, France), which has mechanical properties close to human dentin.
Cones in the distal root canal slightly extruded working length and were adapted accordingly.

Fig. 5
Figure 5
Final obturation of the distal canal and deep split was performed with Ah plus sealer and WVC technique.
A small piece of Teflon tape was placed just over the floor and the orifices and temporary restoration with Cavit G was done.

Fig. 6
About the author:
Dr Eleni Protogerou
Endodontist with expertise in orofacial pain differential diagnosis, root canal treatment and traumatic dental injuries. Bringing 11 years of comprehensive experience determining causes, prevention and treatment of diseases and injuries related to teeth's dental pulp. Valued by patients for promoting good dental hygiene through continuous education and encouragement of preventive maintenance measures. Certified in Endodontics.
Conclusions
Many factors influence successful fragment removal such as operator judgment, training, experience, and utilizing the best technologies and techniques. Knowledge and respect for the anatomy of teeth and familiarization with the typical range of variation associated with each tooth type are essential.
The clinician must keep in mind that fragment removal is just a medium for better disinfection and not an end in itself. The main goal of endodontic treatment of non- vital or revision cases remains to reduce the microbial load to a specific threshold at which the body's immune system can initiate healing. The ultimate goal is to give the treated tooth longevity and boost its survival in a healthy state.
If fragment removal risks to compromise this goal then alternative, more conservative, approaches should be considered.
Bibliography
1.Cheung GSP. Instrument fracture: mechanisms, removal of fragments, and clinical outcomes. Endodontic Topics. 2009; 16(1):1 - 26.
2. Shen Y, Peng B, Cheung GS. Factors associated with the removal of fractured NiTi instruments from root canal sys-tems. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004; 98(5):605-10.
3. M Fu, Z Zhang, B. Hou. Removal of broken files from root canals by using ultrasonic techniques combined with dental microscope: a retrospective analysis of treatment outcome. J Endod. 2011 May;37(5):619-22.
4. Souter, N.J. & Messer, H.H. (2005) Complications associated with fractured file removal using an ultrasonic technique. Journal of Endodontics, 31, 450– 452.
5. Souter, N.J. & Messer, H.H. (2005) Complications associated with fractured file removal using an ultrasonic technique. Journal of Endodontics, 31, 450– 452.
6. Adl, A., Shahravan, A., Farshad, M. & Honar, S. (2017) Success rate and time for bypassing the fractured segments of four NiTi rotary instruments. Iranian Endodontic Journal, 12, 349– 353.
7. Y.Terauchi, WT Ali, MM Abielhassan. Present status and future directions: Removal of fractured instruments. Int Endod J
. 2022 May:55 Suppl 3:685-709.