By-pass with style
14/02/2024
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
The main purpose of an endodontic treatment is to render the root canal system free of bacteria. This will facilitate the resolution of inflammation and the alleviation of symptoms. But most of the time, the clinician faces obstacles that must be overcome to properly disinfect the root canals. Failure to remove these interferences means that parts of the root canal system will not be thoroughly cleaned and will carry on containing a significant population of bacteria. This fact will sustain infection and jeopardize the outcome of the treatment.
One of the aforementioned obstacles that will affect the chemomechanical disinfection of a root canal is file separation/fracture. Although a separated file is not detrimental per se and considered to be responsible for 2-4% of endodontic failures, the subsequent compromised disinfection apically to the fractured file and the underfilling of the canal has been shown to be the cause of 33% of endodontic failures.
Therefore, the main goal of every clinician in a case of a fractured file is to provide adequate cleaning of the canal especially above the separated file. This can be achieved by removing the instrument with dedicated grasping tools or by by-passing the instrument.
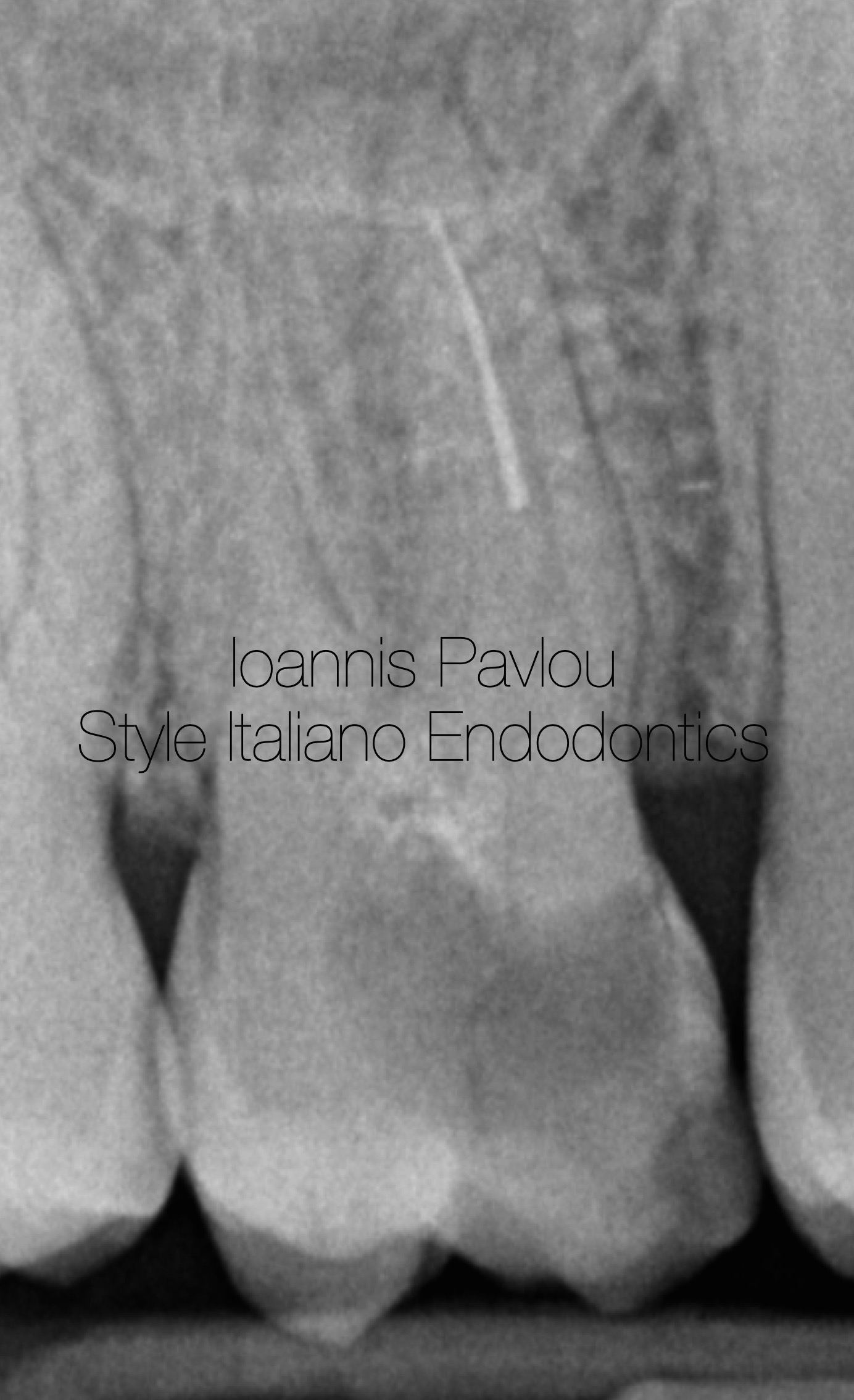
Fig. 1
Figure 1 shows initial x-ray with a fractured NiTi file, 5-6mm in length, lodged at the mid-apical part of the mesiobuccal canal. The tooth had a big carious cavity in the mesial half and a periapical lesion in the palatal root.
After anaesthesia and proper isolation, caries were removed and the cavity was sealed peripherally with RubberDam liquid. The pulp chamber was adequately enlarged preserving at the same time precious pericervical dentine.
Four canals were identified (MB1, MB2, DP and P). MB1 and MB2 orifices were very close, so after orifice opening, they became one canal.
With the aid of Gates Glidden burs, the MB canal was enlarged up to the fractured file, providing a straight access.
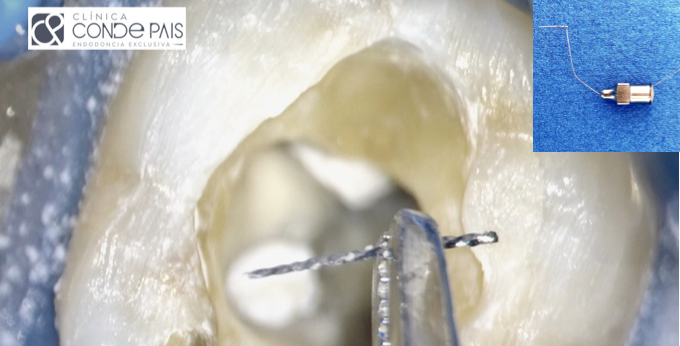
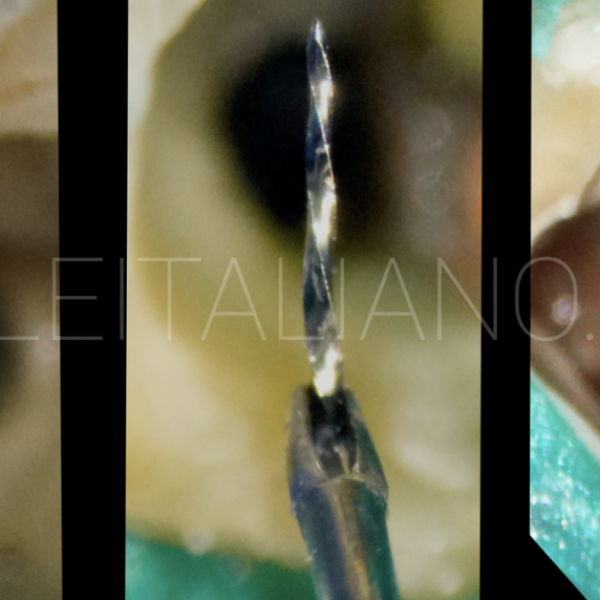
Although in the initial x-ray, the mesiobuccal root seems to be fairly straight, in reality the root had a mesiopalatal inclination. The coronal part was visible under magnification, so it was decided to be removed. With the use of dedicated ultrasonic tips (E9, Fanta), 1-2 mm of the coronal part of the file was revealed and an attempt to dislodge the file was made. The file could be seen that can be moved and a BTR pen was used to grasp the file. The loop was secured and small movements were made in order to free the separated file. Unfortunately, the file was overused, distorted and possibly lodged further apically. That led to separation of the coronal part and the remaining file was beyond the curve, so it was decided to change the approach and try to bypass it.,
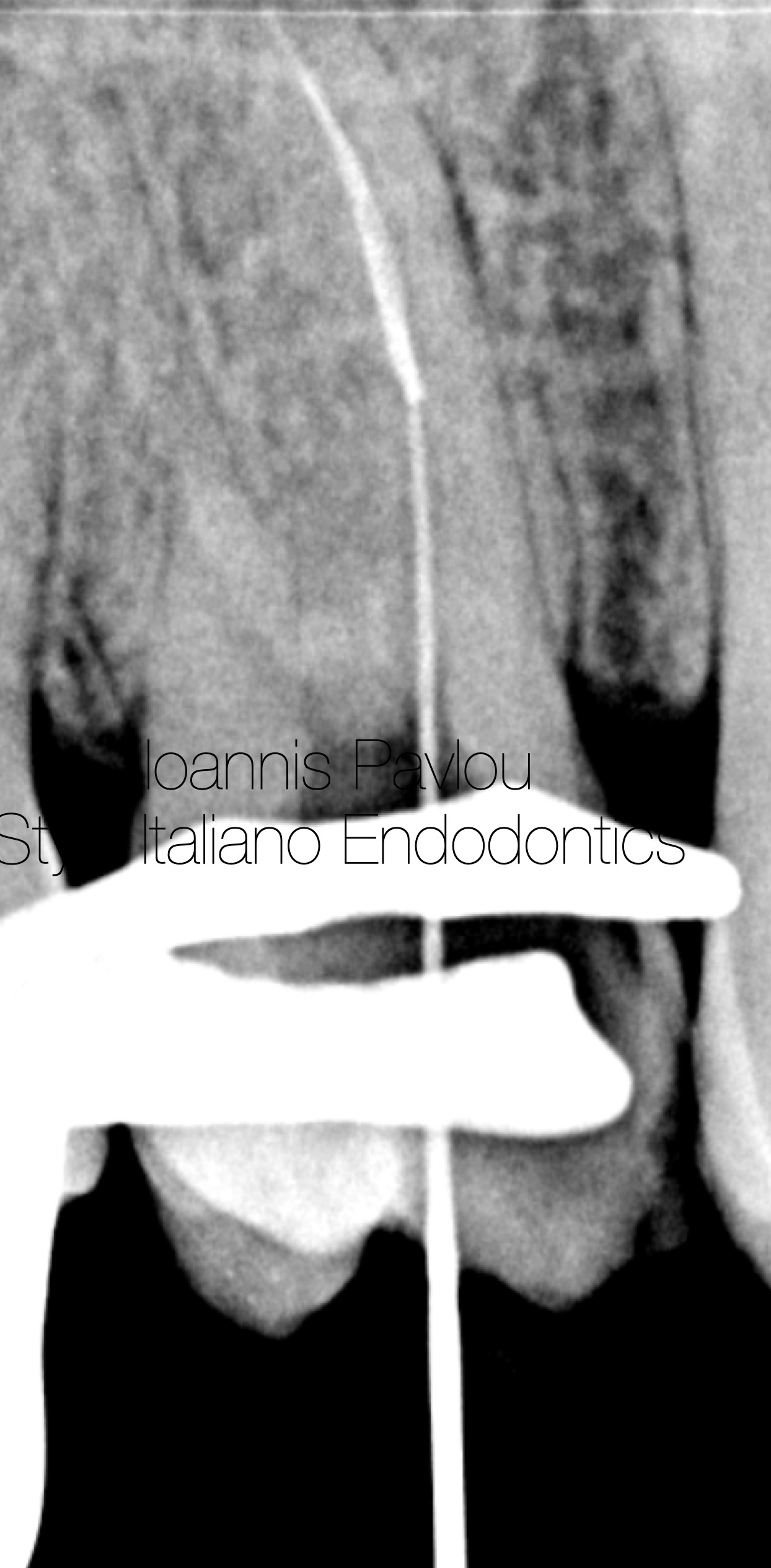
Fig. 2
Whenever we try to bypass a fractured file, especially a NiTi file, we need to remember two things. Fractured NiTi files tend to straighten inside the canal, touching always the outer wall of the canal, and that the majority of the NiTi files have a triangular design. That means that we can only bypass the file by staying on the inner curve of the canal. By soaking the canal with EDTA 17% and with the use of a no10 C-pilot or D-finder file, a path was created. After several attempts, the apex was reached, indicated by the apex locator and verified with an interim x-ray (Figure 2).

Fig. 3
The pathway was further enlarged with the use of no15 D-finder and no20 K-file. Figure 3 shows files in all the canals to the apex. For the instrumentation of the MB canal AF F One rotary instruments were used. This line with R-wire technology and the flat design on one side, is easier to bypass the fractured instrument. The canal was instrumented up to 25.04 . Palatal canal was instrumented up to 60.02 (Hyflex EDM) and Distal canal up to 50.03( Hyflex EDM). The chemomechanical disinfection was completed with copious irrigation of EDTA 17% (3 mins) and NaOCl 5,25% (10ml per canal, 10 mins) with the aid of ultrasonic activation (Ultra-X). The canals were dried with intracanal suction and paper points. Intracanal medicament was placed for 10 days (Calcipast).

Fig. 4
At the second visit, patient was symptom free and confirmed an uneventful period. The intracanal medicament was removed with irrigation and ultrasonic activation. Instrumentation to the established working length with the master file for each canal was executed. Canals were dried and a cone fit x-ray was done (figure 4).

Fig. 5
Obturation was done with cold compaction of single cone with bioceramic sealer (NeoSealer, Avalon). Figures 5 and 6 show the final x-rays after obturation. The patient was sent back to the referral dentist for permanent restoration.

Fig. 6
I graduated as a Certified Dental technician in 1995 from the Technological Educational Institution of Athens. In 2002 I completed my dental studies at the Aristotle University of Thessaloniki. I worked and studied in the UK for 8 years completing a series of postgraduate studies, the most important being the Postgraduate Diploma in Endodontics (Queen Mary, London) and the Postgraduate Diploma in Periodontology (University of Central Lancashire). I returned to Greece in 2010 and since 2015 I have been the principal of a clinic limited in Endodontics and Periodontics. In 2022 I completed the MSc in Prosthodontics at the University of Siena with a special interest in bruxism and TMD.
Conclusions
Fractured instruments present great difficulties for the clinician to provide an adequate disinfection of the root canal system. Any attempts to remove the separated file should respect the anatomy of the root canal and preserve as much as possible precious tooth structure and especially pericervical dentine. In case of bypassing the separated instrument we should always remember to stay in the inner curve of the canal and not to use rotary instruments larger than 4% taper.
Bibliography
- Spili P, Parashos P, Messer HH. The impact of instrument fracture on outcome of endodontic treatment. J Endod. 2005 Dec;31(12):845-50. doi: 10.1097/01.don.0000164127.62864.7c. PMID: 16306815.
- Iqbal A. The Factors Responsible for Endodontic Treatment Failure in the Permanent Dentitions of the Patients Reported to the College of Dentistry, the University of Aljouf, Kingdom of Saudi Arabia. J Clin Diagn Res. 2016 May;10(5):ZC146-8. doi: 10.7860/JCDR/2016/14272.7884. Epub 2016 May 1. PMID: 27437351; PMCID: PMC4948527.
- Terauchi, Y. (2022). Management of Fractured Instruments. In Endodontic Advances and Evidence-Based Clinical Guidelines (eds H.M.A. Ahmed and P.M.H. Dummer). https://doi.org/10.1002/9781119553939.ch18
- Success Rates for Removing or Bypassing Fractured Instruments: A Prospective Clinical Study
Nevares, Giselle et al. Journal of Endodontics, Volume 38, Issue 4, 442 – 444
5. Clinical Outcome of Non-Surgical Root Canal Treatment Using a Single-cone Technique with Endosequence Bioceramic Sealer: A Retrospective Analysis
Chybowski, Elizabeth A. et al. Journal of Endodontics, Volume 44, Issue 6, 941 - 945