

Redefining the access in retreatments: part V of V
29/11/2020
Enrico Cassai
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
In the context of retreatments and re-access, very often it happens to perform a new endodontic therapy removing and sacrificing the old crown.
The choice that the clinician must make in the presence of a pre-existing crown is related to a series of factors that can be summarized in the following diagram and were already discussed in the previous parts of this series of articles.
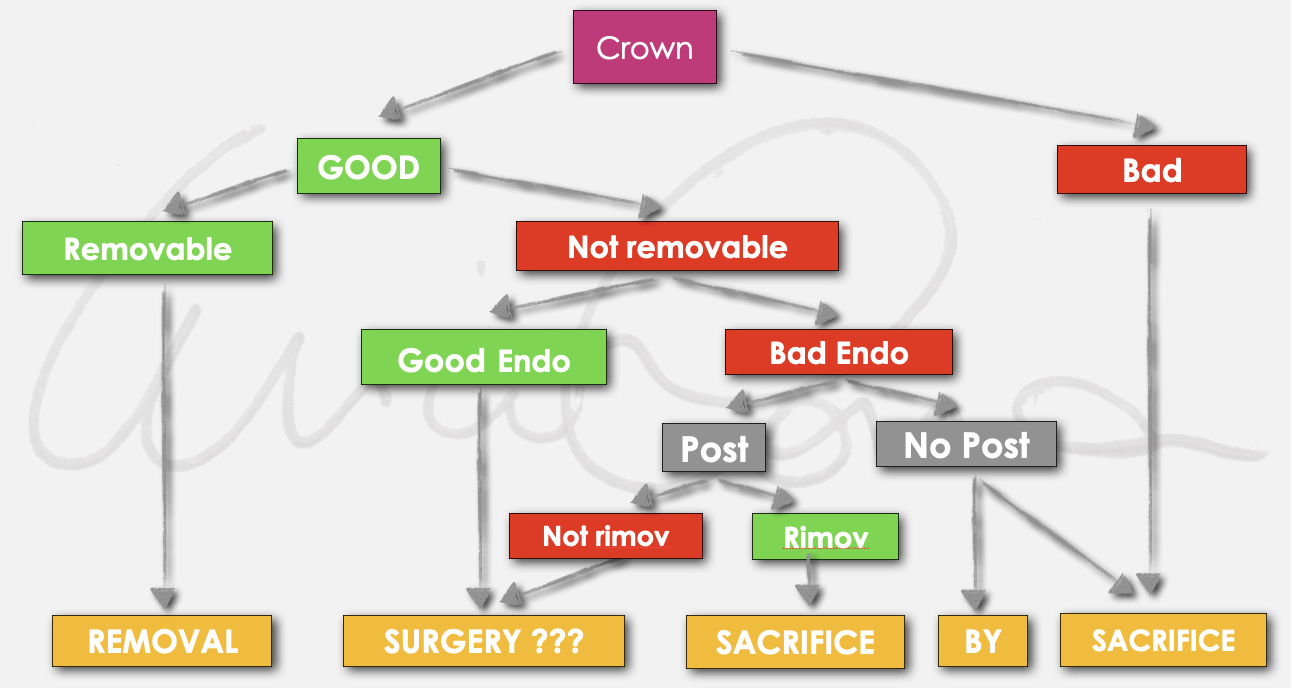
Fig. 1
Summarizing :
- evaluate the quality of the coronal restoration in terms of seal, aesthetic and function
- presence of accessory retention such as posts, considering the position in which they are placed, their length and their possible removal.
- quality of endodontic treatment, thinking about the possible presence of iatrogenic errors such as blocks and / or ledges that make it difficult or impossible to reach a new apical seal.

Fig. 2
If the choice of the clinician is to remove the pre-existing prosthetic crown, some considerations have to be done.
This is a choice that I personally do prefer, compared with the other explained in the previous articles almost all the time for different reason:
- the pre-existing crown could lack from the point of view of the marginal seal, aesthetics or function.
- it is not possible to accurately evaluate the characteristics of the underlying abutment
- in case of atraumatic removal of the crown and modification of the underlying abutment, its re-adaptation involves a loss of precision
- the possibility of using a provisional crown allows to control the healing, evaluate the marginal tissues and allow a better integration in the final step of the definitive restoration with the marginal peridontium
The limits of this approach are mainly related to:
- willingness of the patient
- economic evaluations
- presence of non removable posts or obstacles inside the canals that do not allow the creation of a new apical seal
- high risk of destroying the dental abutment during the removal
- high risk to have an improper dental abutment
In all of the above circumstances, the clinician should evaluate alternative treatment plans, such as endodontic surgery (if possible) or tooth extraction and implant placement (if possible).

Fig. 3
When removing a crown, try to be as fast as possible and try not to touch the underlying stump.
In this sense, I recommend using new coarse-grained cutters to remove the ceramic coating layer and multi-blade crown cutters for the underlying metal structure. For zirconia crowns, I recommend using dedicated burs.
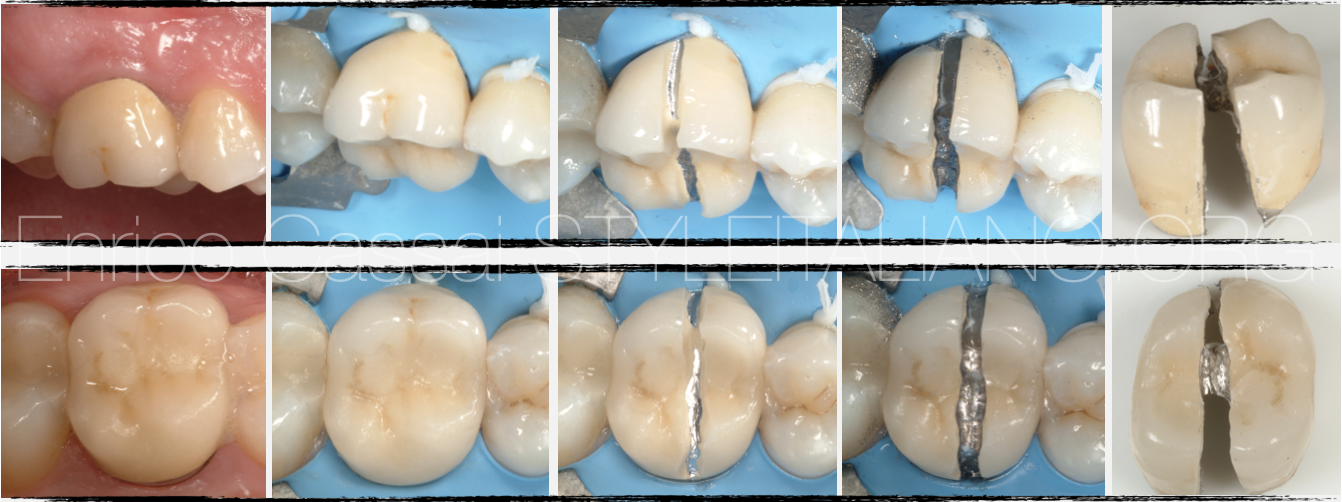
Fig. 4
The crown can be completely cut from buccal to lingual / palatine or sometimes it may be enough to create the space for the insertion of a lever inside to allow its removal.

Fig. 5
One aspect to take into consideration is the aesthetic area.
In fact, when removing a crown in the anterior or aesthetic area, once the endodontic therapy has been completed and the dental abutment has been reconfigured, a provisional crown(preprepared or chairside) must be placed.
Fig. 6
Here is an example of crown removal in an aesthetic area.

Fig. 7
A young patient came in my office with a provisional crown on tooth 1.1. A screw post was inserted inside the canal but it was loose, with a high risk of decementation of the crown or damages to the root (crack or fracture).
The patient felt pain at the percussion on 11 and also to the palpation on the apical zone of the tooth.
The tretament plan was to disassemble the crown and post, retreat, restore the dental abutment with a post & core and put a provisional crown in the same appointment.
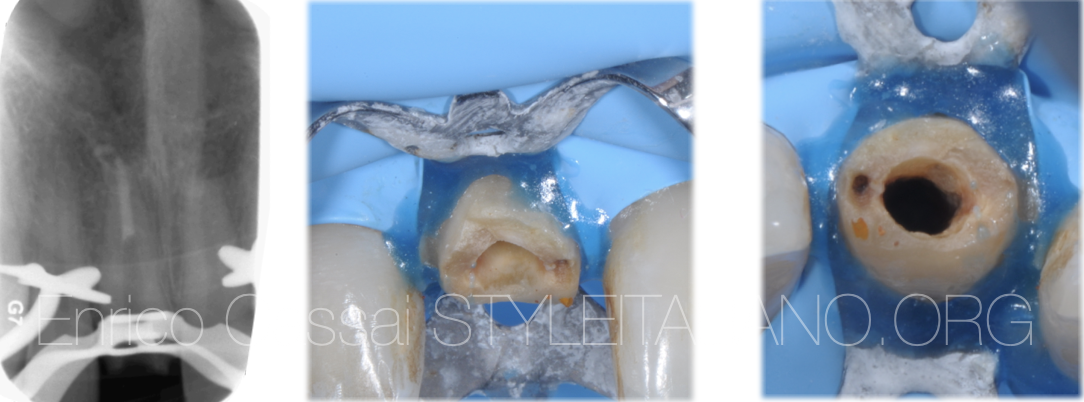
Fig. 8
I did a multiple isolation in order to be easily able to restore the tooth in the same appointment after the endodontic therapy without removing the rubber dam.
First of all I removed the crown.
After removing the post by unscrewing it with an ultrasonic tip, I began to take care of the obturation material present into the middle-apical portion of the canal.
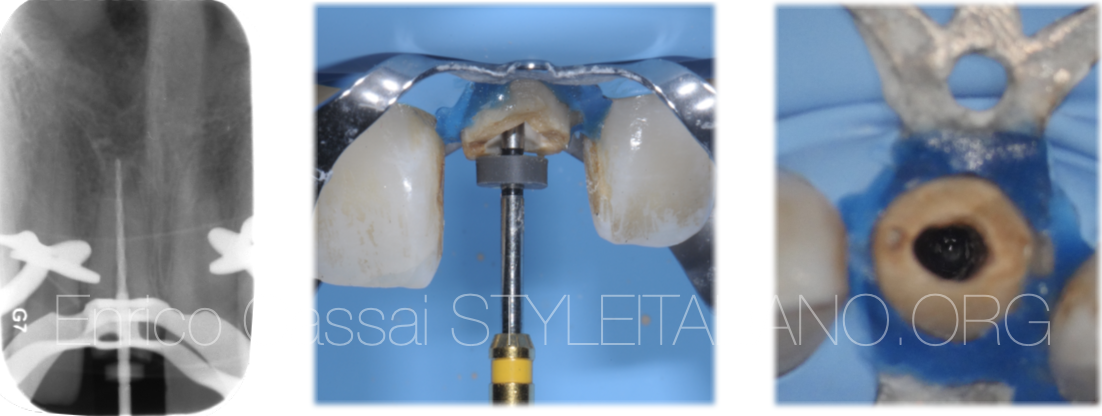
Fig. 9
Since the canal appeared straight, I decided to remove the gutta-percha with mechanical instruments and a minimum use of solvents.
I reached the working length, but the apical portion of the roots seemed resorbed: this would have made it difficult to avoid extrusion of gutta-percha packed with a continuous wave of condensation, so I decided to do an apical plug with MTA.
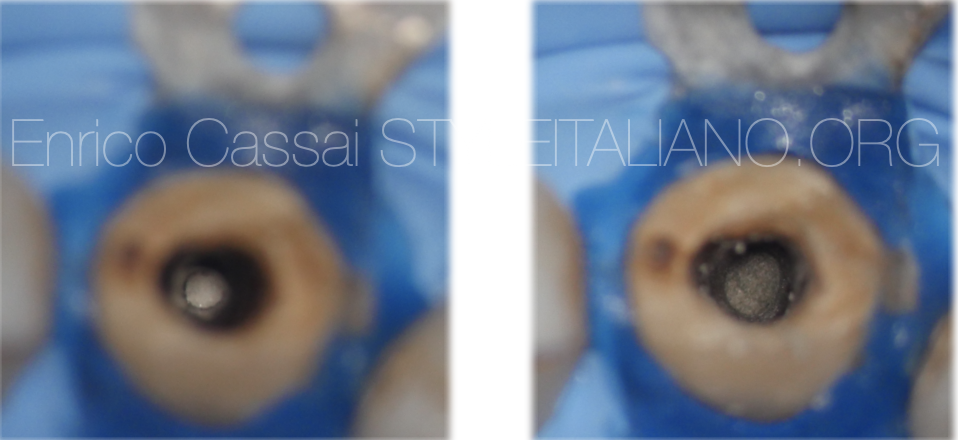
Fig. 10
When doing an apical plug I prefer to put a collagen barrier beyond the apex in order to have a better vision with the microscope and to have a better control of the obturation in this area.
I used a MTA carrier to bring the filling material at the apical portion and I compacted it for 5-6 mm.

Fig. 11
After MTA hardened, I placed thermoplastic gutta-percha on it and restored the dental abutment with a post and core composite material.

Fig. 12
After restoration I adapted a previously prepared provisional resin crown to the tooth

Fig. 13
3 months after the therapy I checked the healing process and the integration of the provisional crown with the soft tissues, then I took an impression for the ceramic crown.
The ceramic crown was done modifying a little bit the proportion of the tooth, in order to eliminate the little diastema.

Fig. 14
7 years follow up
Fig. 15

Fig. 16
A patient came to my office complaining about continuous pain on the tooth 3.6.
The patient referred he received a prosthetic crown on this tooth two years earlier.
At the radiographic examination a large radiopacity on the distal root could be seen, the old obturation seemed short, the shaping had no taper (maybe the tooth was filled with cold gutta-percha) and there was something like a screw post in the distal root.
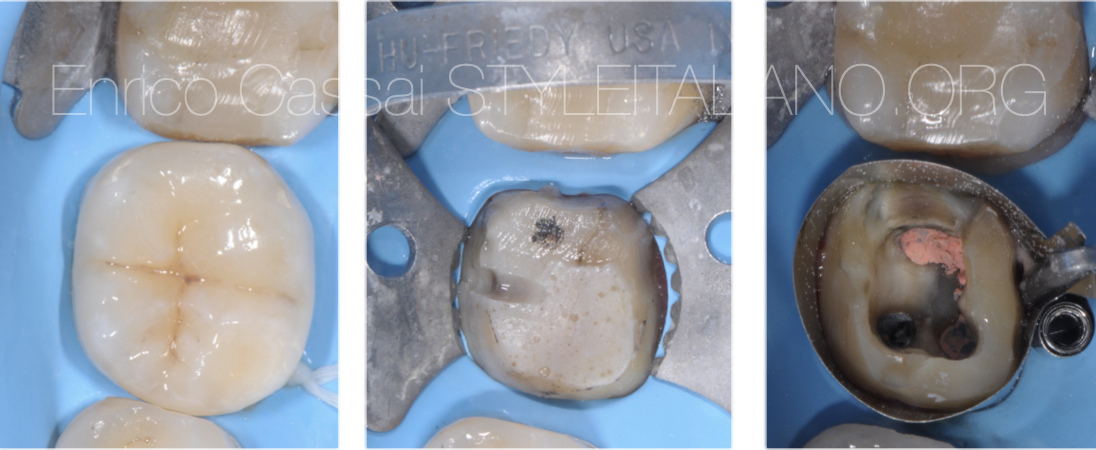
Fig. 17
I did a multiple isolation in order to be easily able to restore the tooth in the same appointment after the endodontic therapy without removing the rubber dam.
First of all I removed the crown.
After unscrewing the post with ultrasonic tips I removed the obturation material, scouted, cleaned, shaped and filled all the canals.
Since the canals were really long I preferred to use a carrier based technique in the mesials and the continous wave technique in the distals.
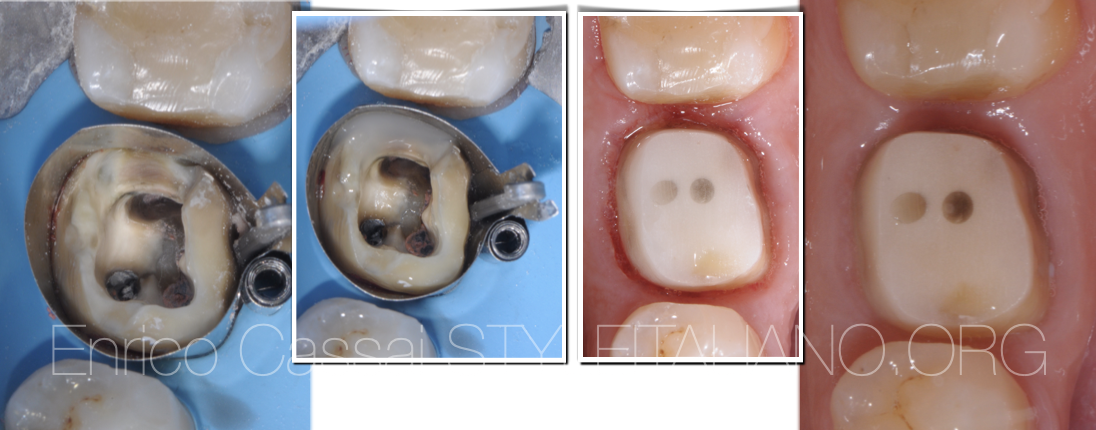
Fig. 18
In the same appointment I restored the tooth with post & core composite material and I prepared the dental abutment for the impression for the provisional crown.

Fig. 19
Dental abutment after the impression and x-ray after the first appointment.

Fig. 20
3 months later I checked the healing process and the integration of the provisional crown with the soft tissues, then I took an impression for the ceramic crown.

Fig. 21
9 years follow up: the lesion completely disappeared.
Conclusions
In this article the correct protocol in the case of removal of a preexisting crown for an orthograde retreatment was shown.
The recommendations are the following:
- take always a CBCT beside an initial x-ray
- study with accuracy any diagnostic preoperative record in order to intercept in advance any possible problem during the therapy (missed canals, curvatures, blocks, ledges,…)
- make sure to have preprepared a provisional crown before starting the removal of the pre-existing one
- Take all the time you need to perform the disassembling, the endodontic retreatment, the post&core (if needed) restoration and even the impression or the adaptation of the preprepared provisional crown
- Control every month the tooth with provisional crown and check the marginal seal of the crown, together with the absence of symptoms.
- Do the definitive crown once the tooth is asymptomatic, the lesion appears in healing and the tissue integration and the shape of the provisional crown are perfect
Bibliography
Scianamblo MJ: Endodontic failures: the retreatment of previuosly endodontically retreated teeth, Revue Odontostomatol (Paris), 1988
Parreira FR et al: Cast prosthesis removal using ultrasonic and thermoplastic resin adhesive, J Endod, 1994
Carr GB: Retreatment. In Cohen S, Burns Rc, editors: Pathways of pulp, 199
Girard JL: Advancement in the removal of permanently cemented crowns and bridges, Smile Dent J, Vol 5, Issue 4, 2010
Westermann R: A System for Treating Crown-and-Bridge Failures, Dentistry Today, 1996
Retreatments, Edra



