Redefining the access in retreatments: Part III of V. The crown access management
07/11/2020
Enrico Cassai
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
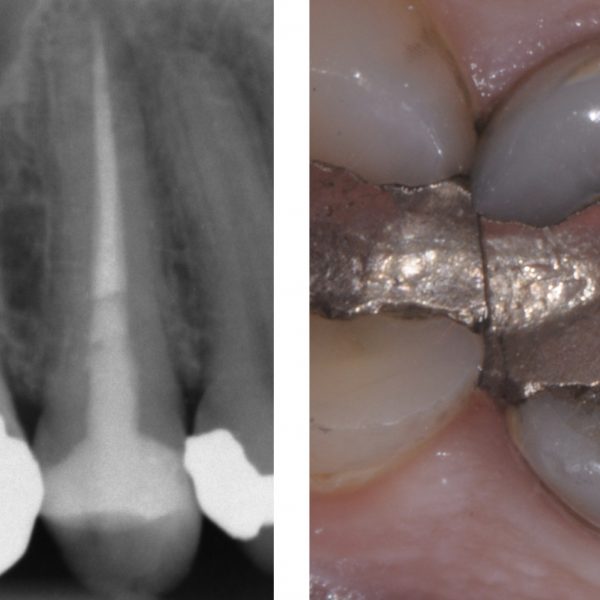
In the context of retreatments and re-access, it often happens to perform a new endodontic therapy dealing with the presence of a crown.
A careful pre-operative evaluation can allow the clinician, according with the patient's wishes, to face the best therapeutic choice.
The opportunities are, in fact, those related to the removal of the pre-existing crown in a conservative way, the execution of an endodontic therapy through the pre-existing crown or the sacrifice of the crown with its subsequent replacement.
The choice that the clinician must make in the presence of a pre-existing crown is related to a series of factors that can be summarized very briefly in Diagram 1 and their consequences in Diagram 2.
It will be necessary to carefully evaluate the quality of the coronal restoration in terms of seal, aesthetic and function.
Secondly, to analyze the presence of accessory retention such as posts, considering the position in which they are placed, their length and their possible removal.
Finally, attention will have to focus on the quality of endodontic treatment, thinking about the possible presence of iatrogenic errors such as blocks and / or ledges that make it difficult or impossible to reach a new apical seal.
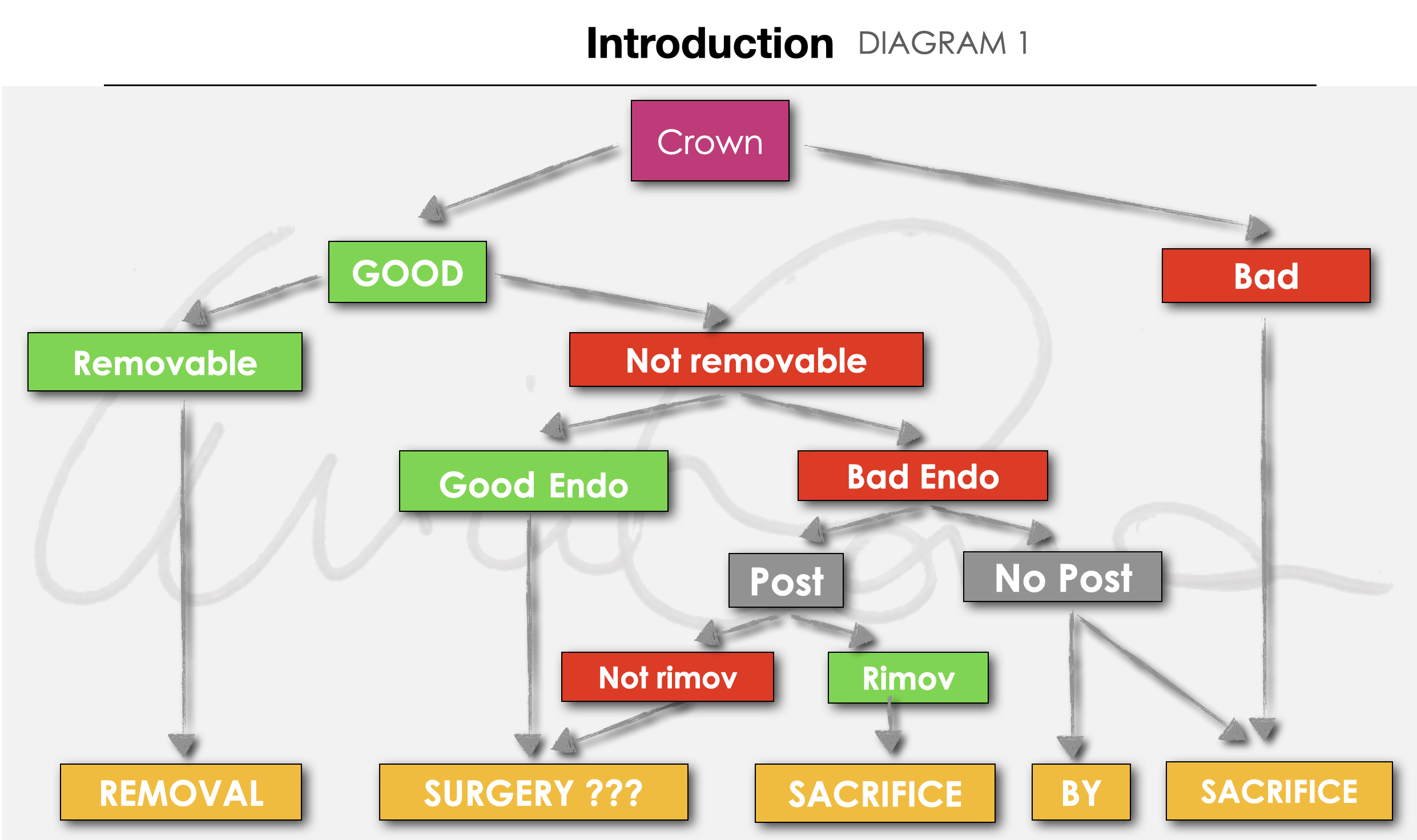
Fig. 1
Diagram 1
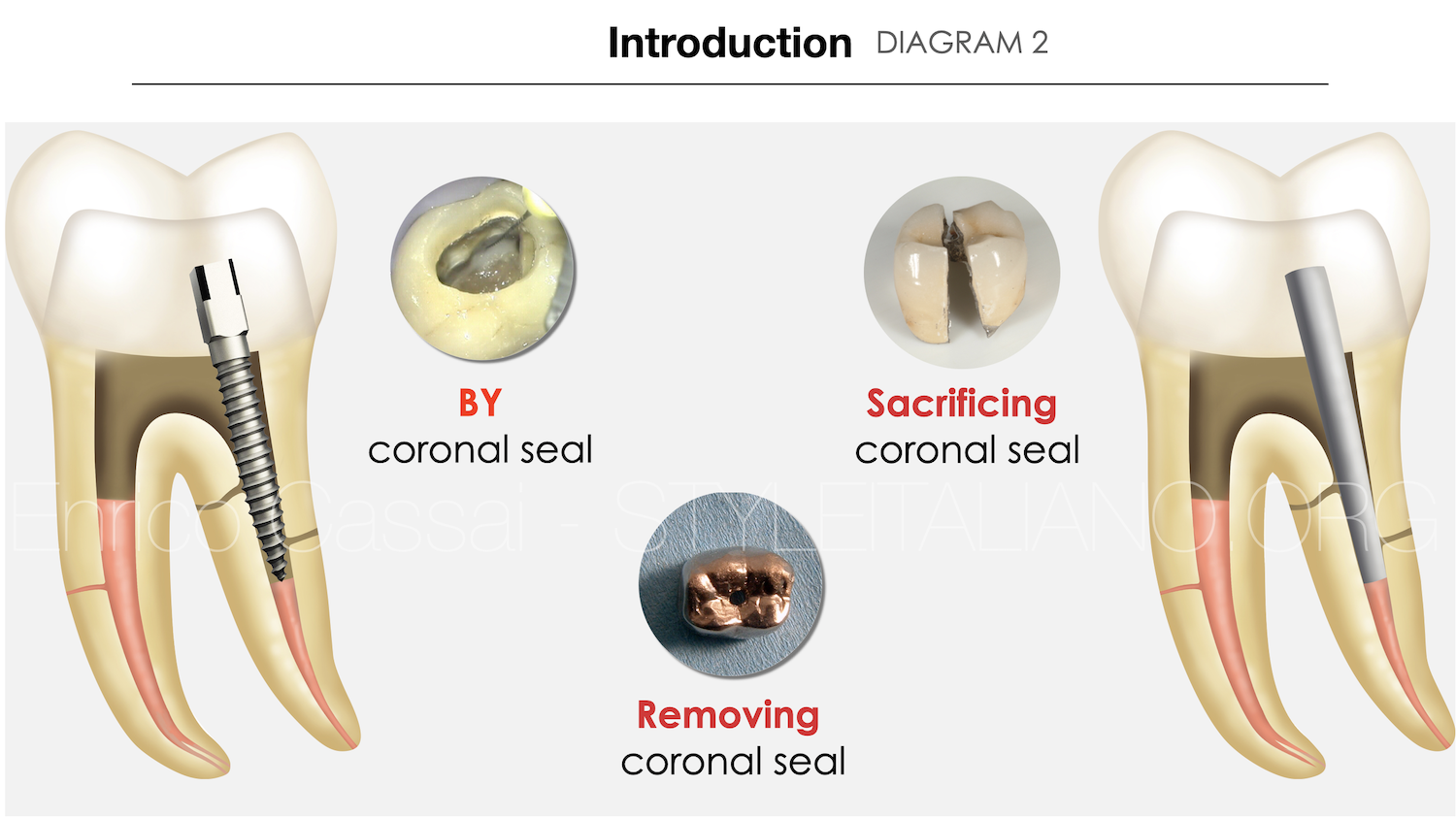
Fig. 2
Diagram 2

Fig. 3
In this section I will consider re-entry through a pre-existing prosthetic crown.
This option can arise from a series of needs such as:
- willingness of the patient
- presence of a crown that cannot be removed except through sacrifice
- presence of a non-removable crown in the absence of non-removable posts
- presence of a good crown in terms of marginal seal, aesthetic and functional aspects
- operating time
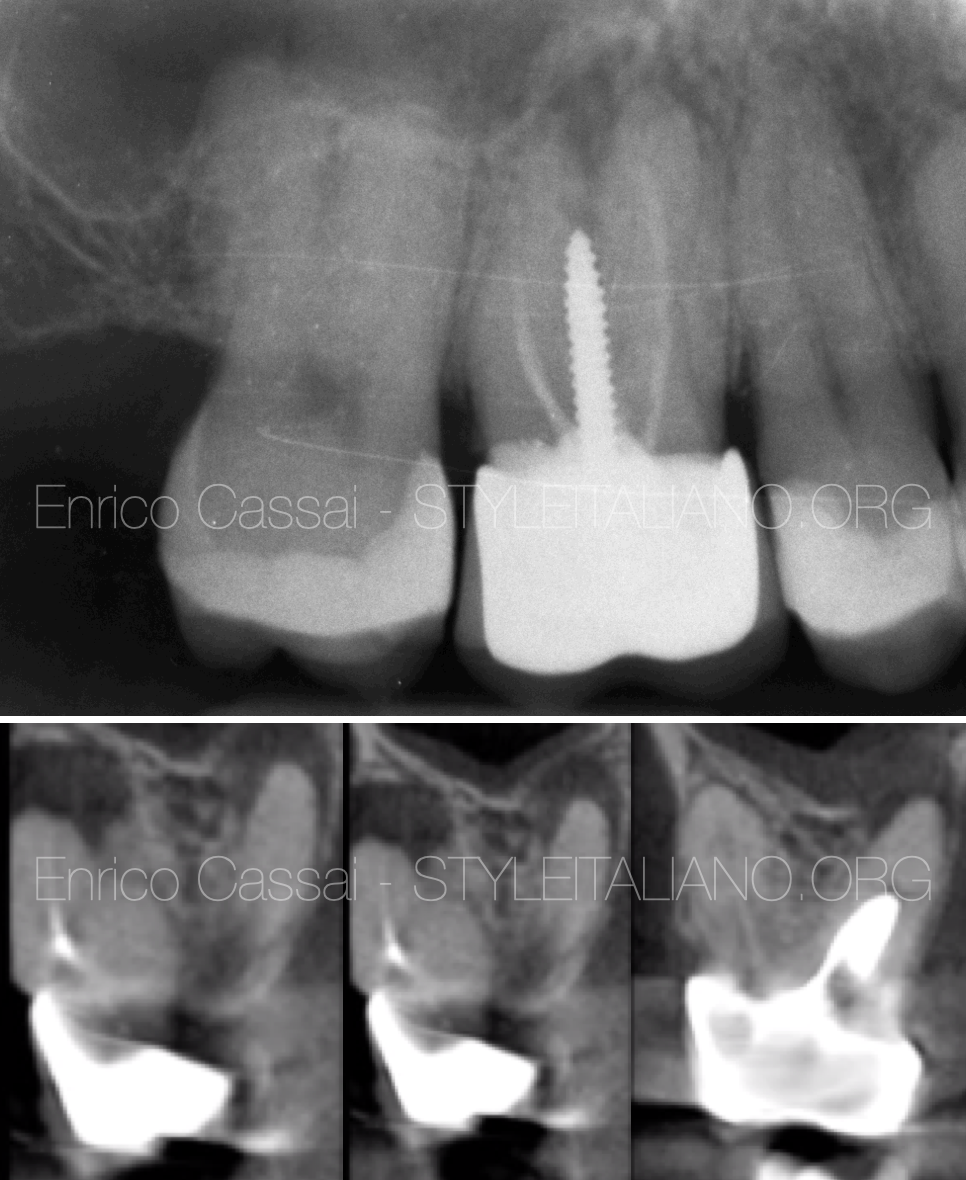
Fig. 4
PREOPERATIVE EVALUATION (X-RAY + CBCT)
The execution of a CBCT in addition to the preoperative x-ray is a mandatory tool in retreatments as it is already well explained in literature.
In this case, CBCT was fundamental in highlighting:
- presence of periapical lesions in MB, DB and P roots
- absence of damage related to the positioning of the post in the P canal
- presence of the MB2 canal with a confluency at the apex with the MB1
- project the correct extension of the access cavity to remove the post properly, identify all the orifices without excessively weakening the prosthetic structure

Fig. 5
After performing a multiple isolation with rubber dam, proceed with the execution of the access cavity on the pre-existing crown.
ENDODONTIC ACCESS CAVITY
Take care about some aspects:
- perform the cavity more extensively than would be done on a natural tooth to increase the light and foresee any alterations of the underlying prepared tooth
- choose the appropriate burs based on the type of material with which the crown is made and preferably new ones
- evaluate the correct inclination during the penetration steps respecting the angle of the abutment
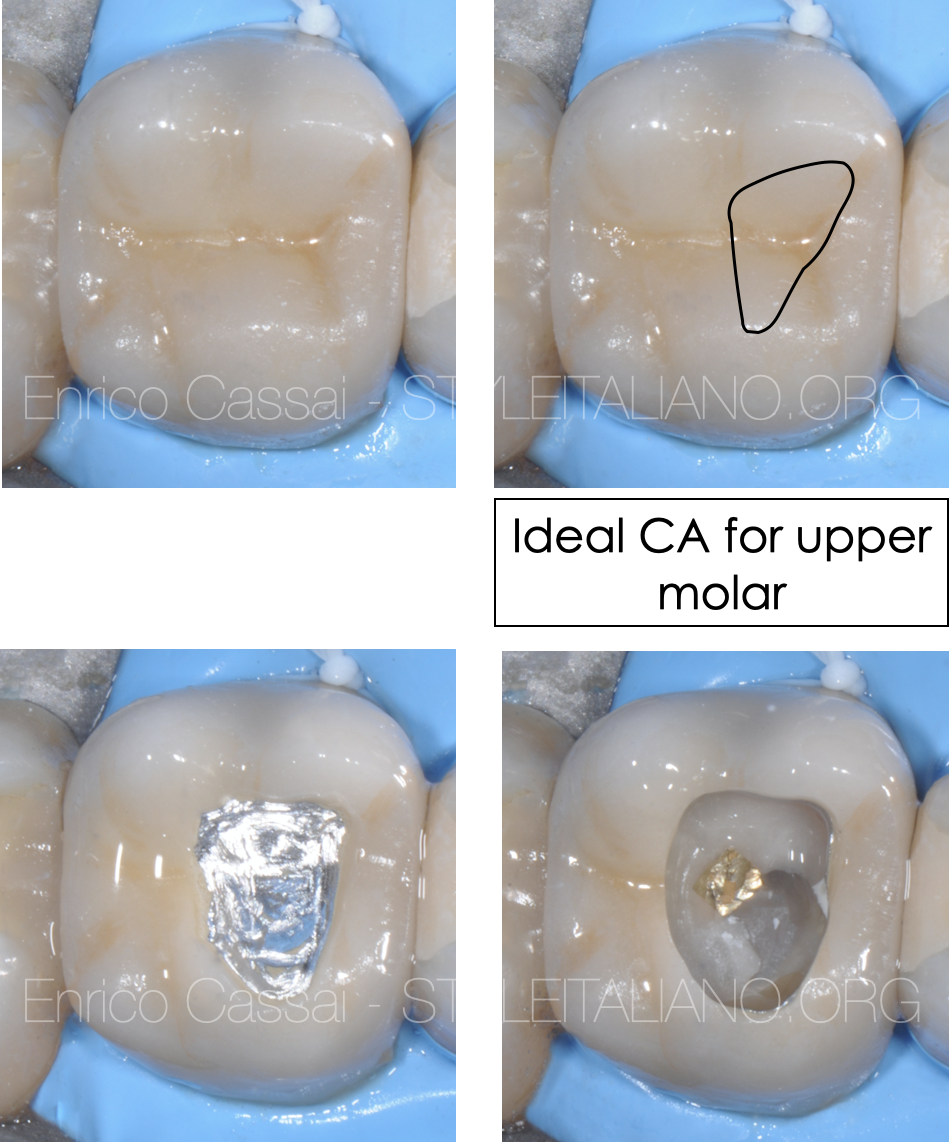
Fig. 6
In this case I designed a cavity access through a metal-ceramic crown. For this reason it is important to use a NEW coarse-grained diamond bur to remove the ceramic coating. Then I used a multi-blade bur to remove the thickness of the underlying metal, trying not to end up at the same level as the previous cut.
In fact, the risk is to cause accidental fractures of the ceramic coating.
I removed the restorative material of the abutment with a diamond-coated bur and ultrasonic tips appropriately isolating the post which was unscrewed with ultrasonic tips.
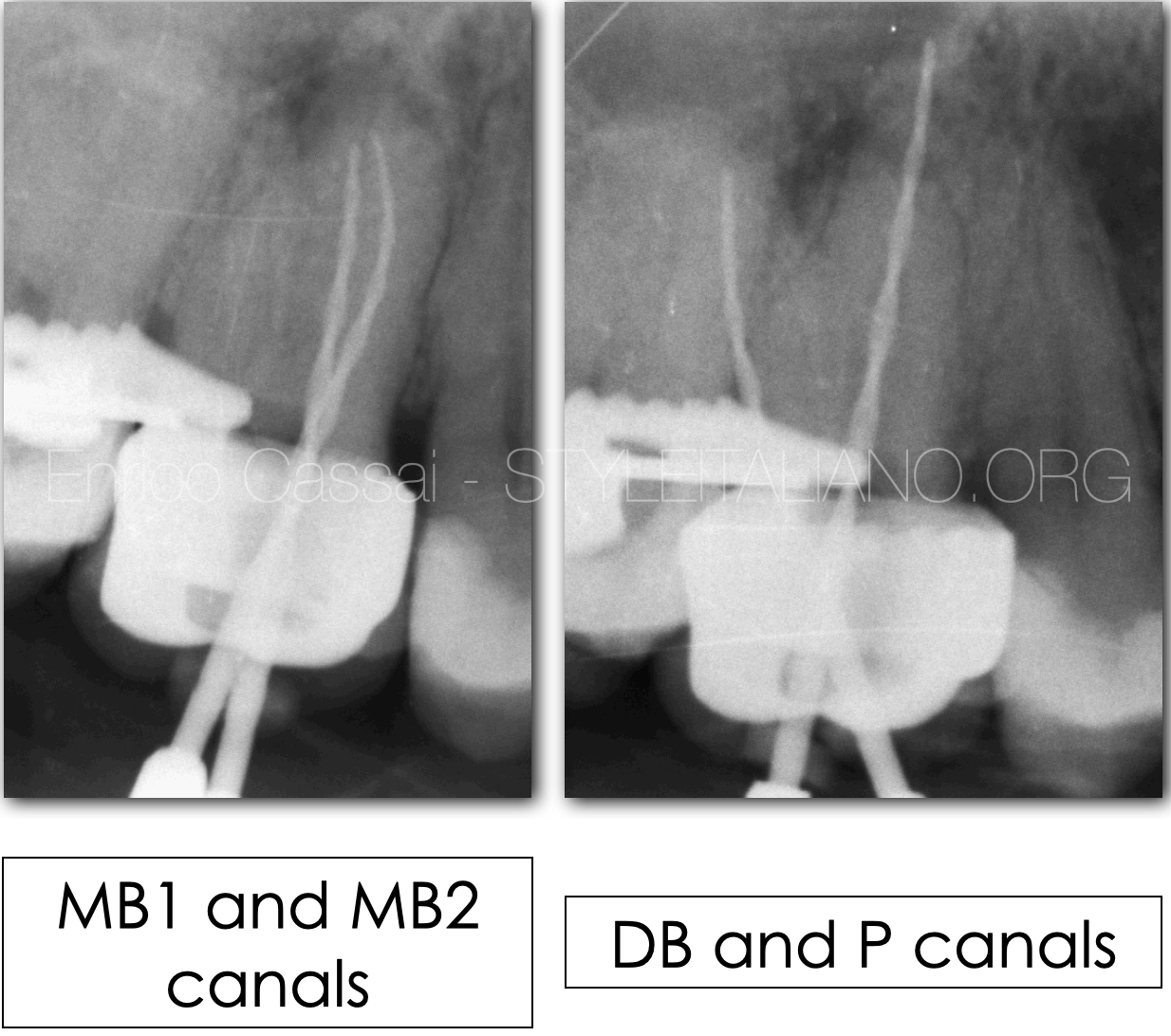
Fig. 7
WORKING LENGTH DETERMINATION
Once the cavity access was done, the canals were identified and the coronal interferences (preflaring) in MB and DB canals were removed, I scouted with K-file up to the correct working length, then cleaned and shaped all the canals.
To check the accuracy of the electronic WL I took an x-ray with the last mechanical file brought to the WL for every canal.

Fig. 8
At the end of the treatment a control x-ray was performed to evaluate its correct execution.
Canals were filled with the continuous wave of condensation technique.
It is possible to appreciate from the different projections that the MB2, as seen during the intra-operative x-ray, is confluent with MB1 at the apex.
All the canals were well filled and the patient was sent back to his dentist to finish the restoration of the tooth.

Fig. 9
At the 4-years follow up, the x-ray showed the perfect healing of the lesion

Fig. 10
4 years follow up
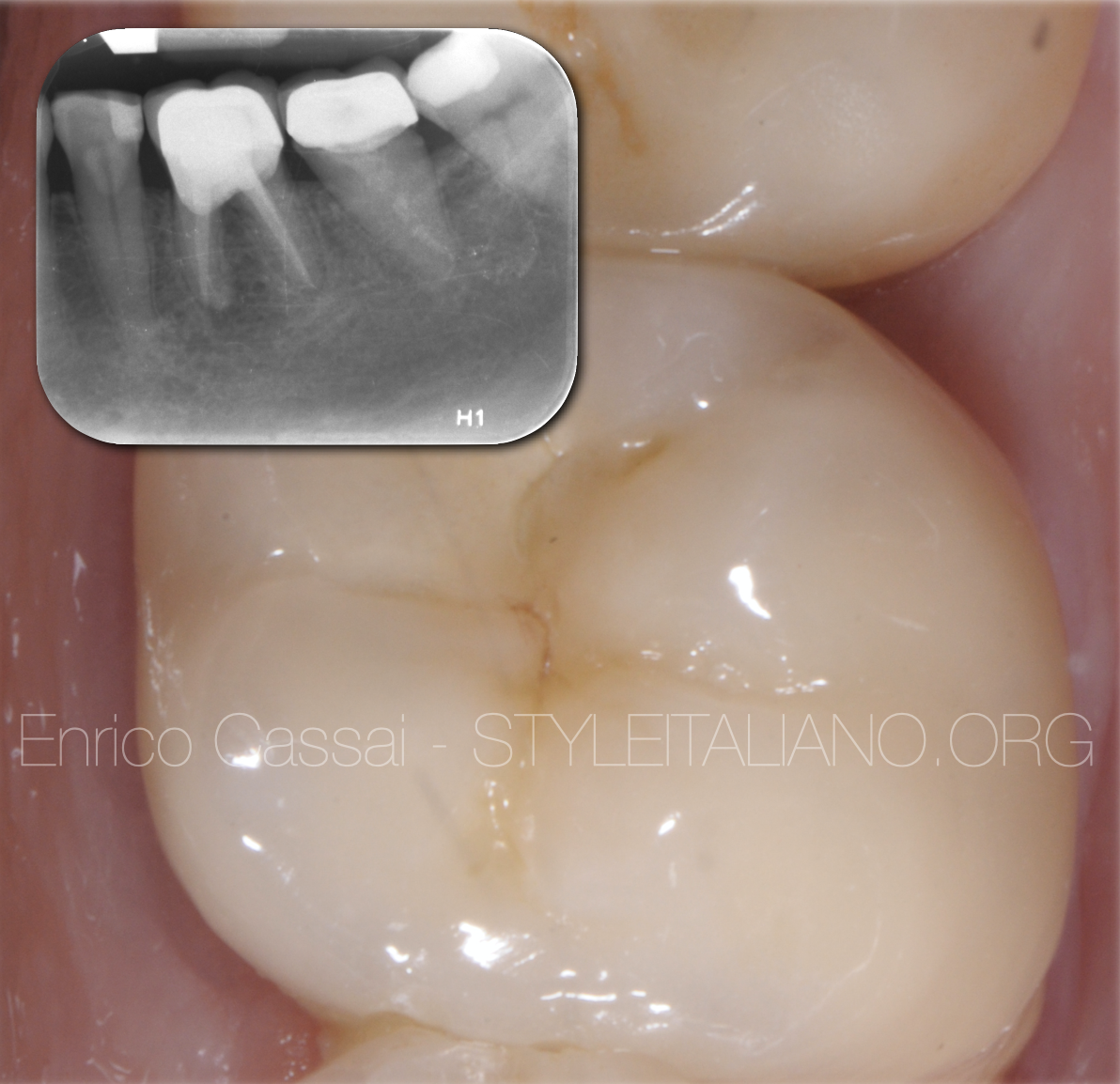
Fig. 11
SELECTIVE ENDODONTIC RETREATMENT
In some cases it may happen that there is a need to re-access only one root canal through the crown, because it was forgotten or not found during the initial treatment.
Although generally it is an approach that I do not prefer and I do not recommend for the increased difficulty, it can occur when requested by a colleague who sends a patient and in the presence of a pre-existing congruous endodontic treatment.
PREOPERATIVE EVALUATIONS (CBCT)
As in any retreatment, it is absolutely recommended to perform a CBCT in addition to the initial x-ray before starting the treatment.
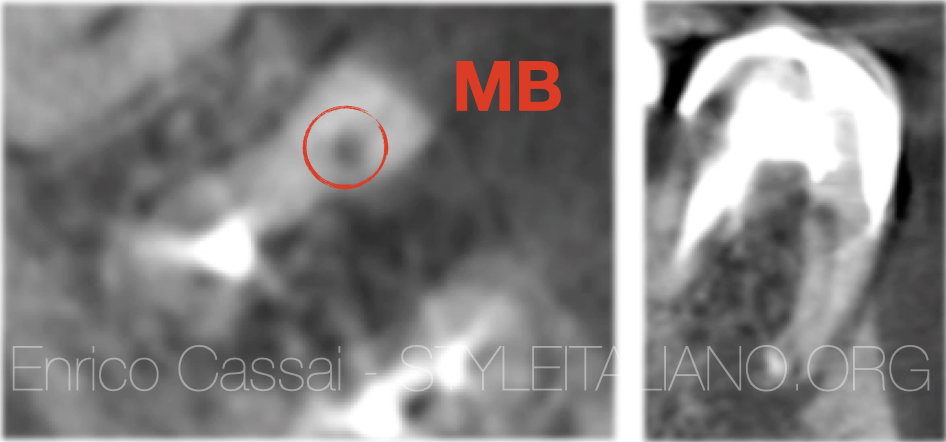
Fig. 12
In this way, the clinician will be able to easily locate the position of the forgotten canal and study a correct and conservative design of the access cavity to selectively find the canal without excessively damaging the structure of the pre-existing crown.
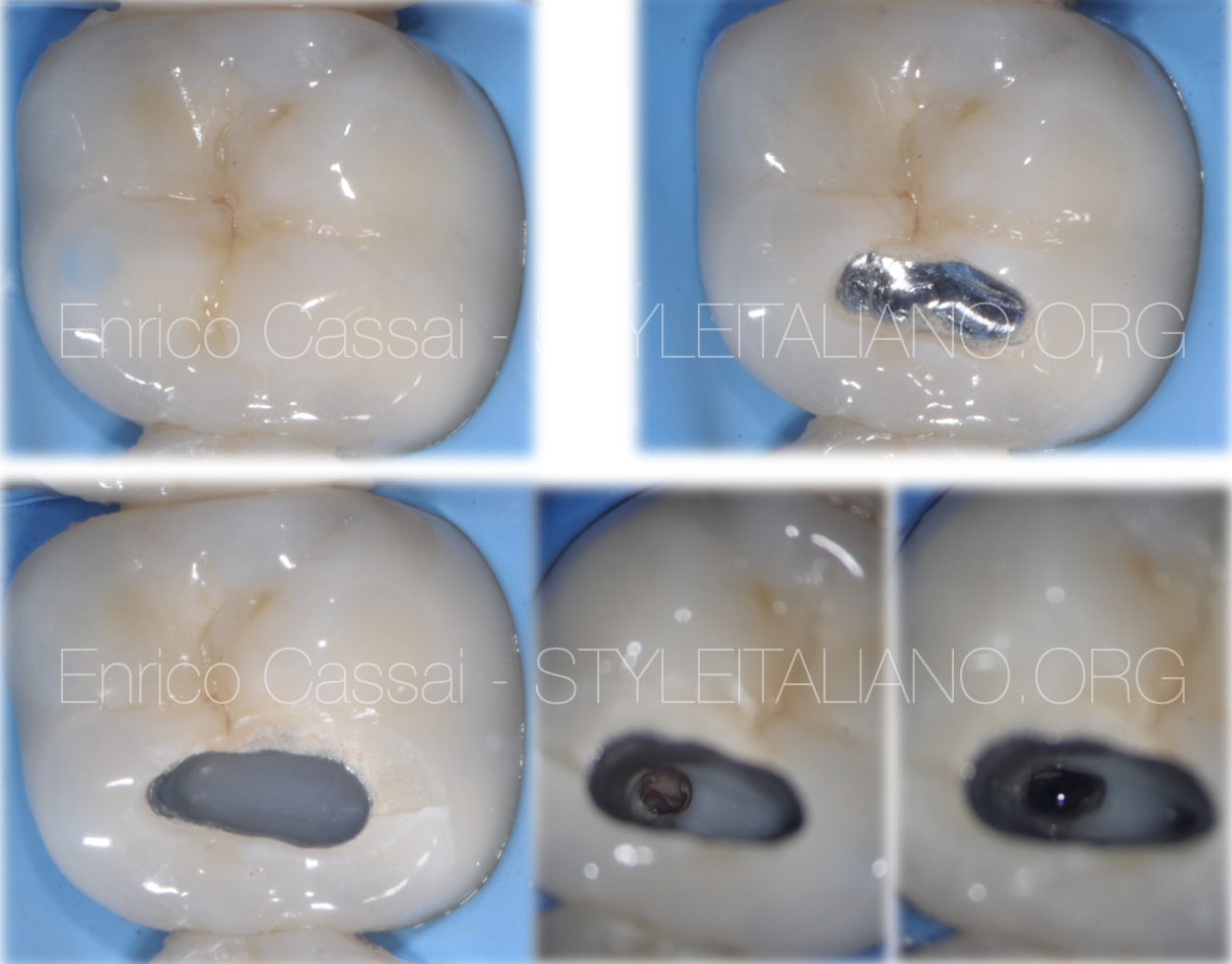
Fig. 13
MODIFIED ENDODONTIC ACCESS CAVITY
The cavity access realisation must follow the same assessments made previously, however, should done much smaller.
The key of success in this case is to understand priorly the position in which to develop the cavity design and relate it to the type of material with which the crown is manufactured:
- gold-resin
- gold
- metal ceramic
- full ceramic
- zirconia
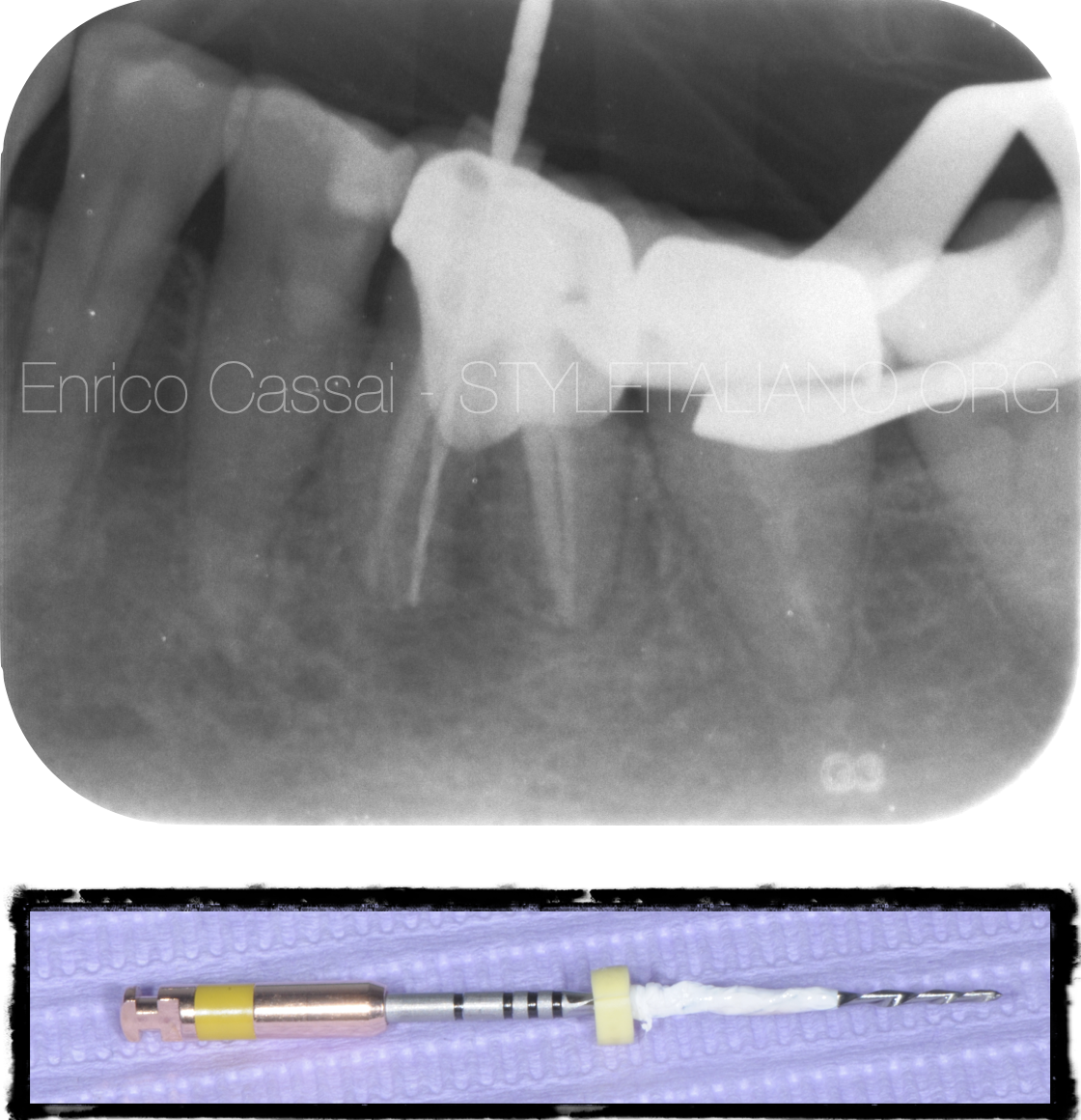
Fig. 14
WORKING LENGTH DETERMINATION
TIPS & TRICKS
Once executed the conservative cavity access, identified the missed canal and the removal of coronal interferences (preflaring) if present, the scouting with K-file up to the correct working length could bring some problems for the presence of metal.
In this case to have a perfect lecture from the apex locator of the right working leght it is suggested to wrap around the file some teflon in order to prevent the touch of it against the metal (if present) of the crown.

Fig. 15
The missed canal were scouted, shaped and cleaned till the correct working lenght and then obturated with the continuous wave of condensation technique.
At the end of the treatment an x-ray was performed to evaluate its correct execution and then the tooth was restored with a composite build-up and sent to the referring dentist with the recommendation to check it with x-ray every year.

Fig. 16
At the 5 years follow up, the x-ray shows the perfect healing of the lesion.
Conclusions
In this article the correct protocol in case of re-access on an orthograde retreatment of preexisting crown was shown.
The recommendations are the following:
- take always a CBCT beside an initial x-ray
- study with accuracy any diagnostic preoperatory investigation in order to intercept in advance any possible problem during the therapy (missed canal, curvatures, blocks, ledges,…)
- Enlarge the cavity access design more than you will do to a natural tooth considering also the inclination od dental abutment
- choose new burs properly and according to the material you have to penetrate
Bibliography
Scianamblo MJ: Endodontic failures: the retreatment of previuosly endodontically retreated teeth, Revue Odontostomatol (Paris), 1988
Parreira FR et al: Cast prosthesis removal using ultrasonic and thermoplastic resin adhesive, J Endod, 1994
Carr GB: Retreatment. In Cohen S, Burns Rc, editors: Pathways of pulp, 199
C Ruddle, Endodontic Access Preparation an opening for success, Dent Today 2007
Retreatments, Edra