Redefining the access in retreatments: Part I of V
10/06/2020
Enrico Cassai
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
One of the most important step of endodontic therapy is the execution of the access cavity. Very often the failure of the therapy arises from an incorrect realization of this initial step with consequences that can lead to the missing of canals, improper detersion and shaping of the root canal system until the fracture of instruments.
This is the first of five articles, where is explained the correct approach that must be take during the reaccess in a retreatment through the explanation of a clinical cases.
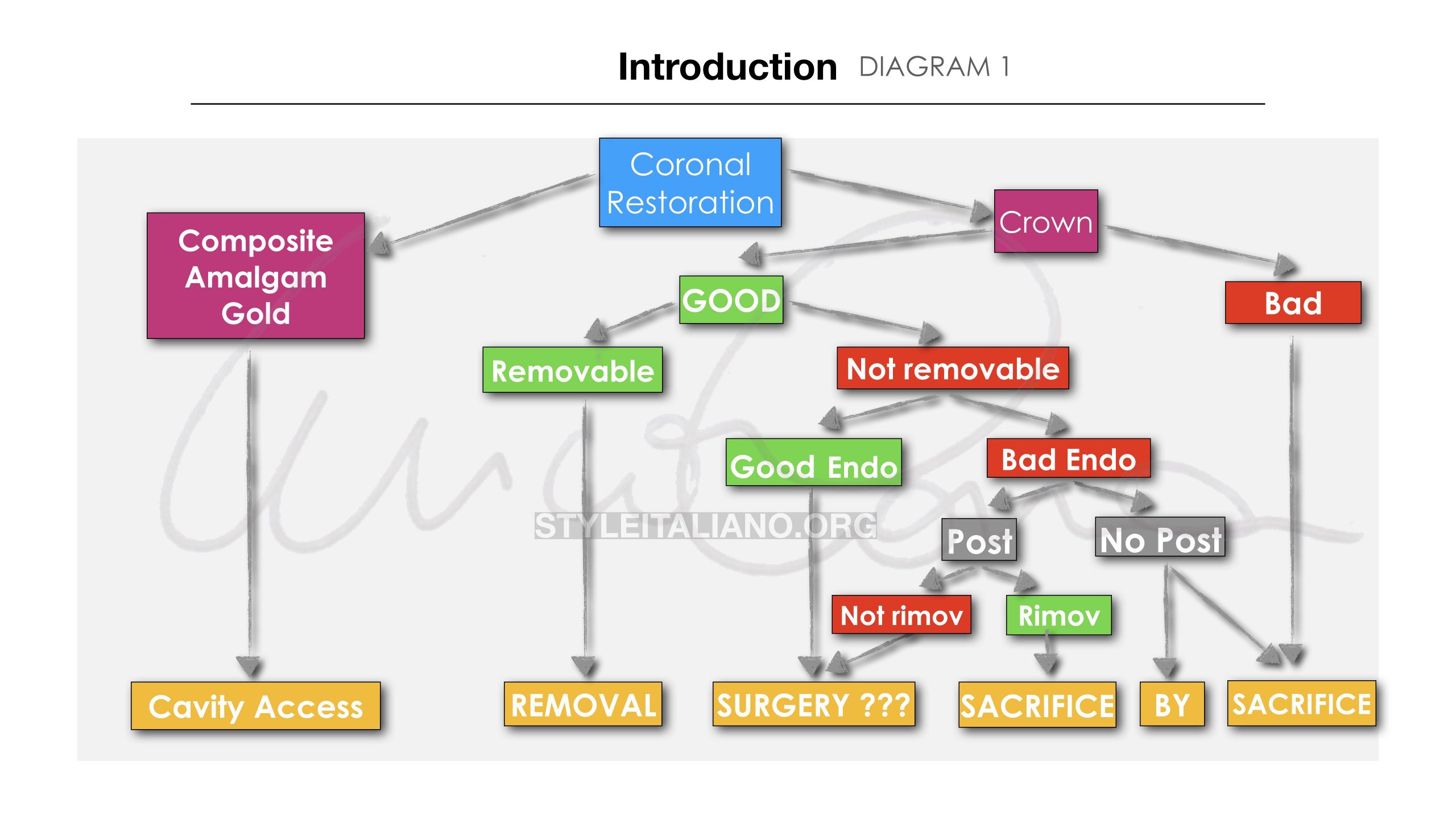
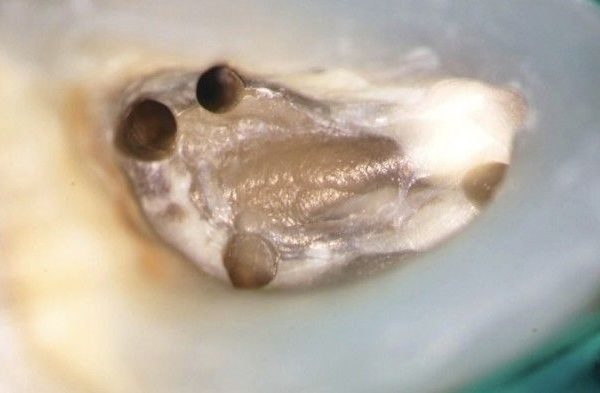
Fig. 1
Among the main cases of failure of endodontic therapy, as the scientific literature shows (1,2) surely there is the lack of finding root canals or the incorrect apical seal.
Many of these problems are connected to an initial error in the construction of the access cavity.
For this reason, once the indication for endodontic retreatment has been evaluated (which is not only based on purely endodontic evaluations, but also of a restorative, periodontal and occlusal nature), the clinician will have to pay close attention to the reconfiguration of the access cavity.
This operation often clashes with the evaluation of the pre-existing restoration and on its possibility of removal, replacement or recovery based on the type of restoration present, its quality, its possible removal and the quality of the underlying restoration (see diagram 1).
If the restoration through which it is necessary to perform orthograde reprocessing is a dental amalgam, there are some considerations to be made before proceeding operationally, especially about what the final restoration will be, which in most cases will be cusp-covered. (3)

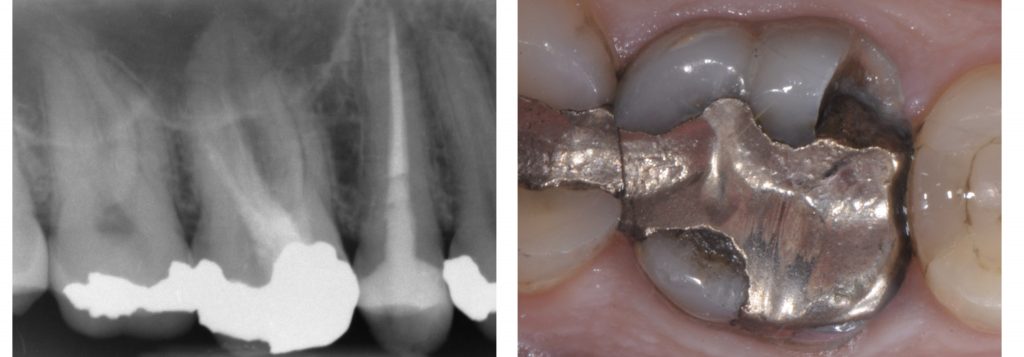
Fig. 2
The removal of amalgam commences as follows:
- New dental bur
- Isolation with rubber dam
- High volume suction and a continual addition of water spray
- Section the amalgam along the cavity wall, around the edge of amalgam
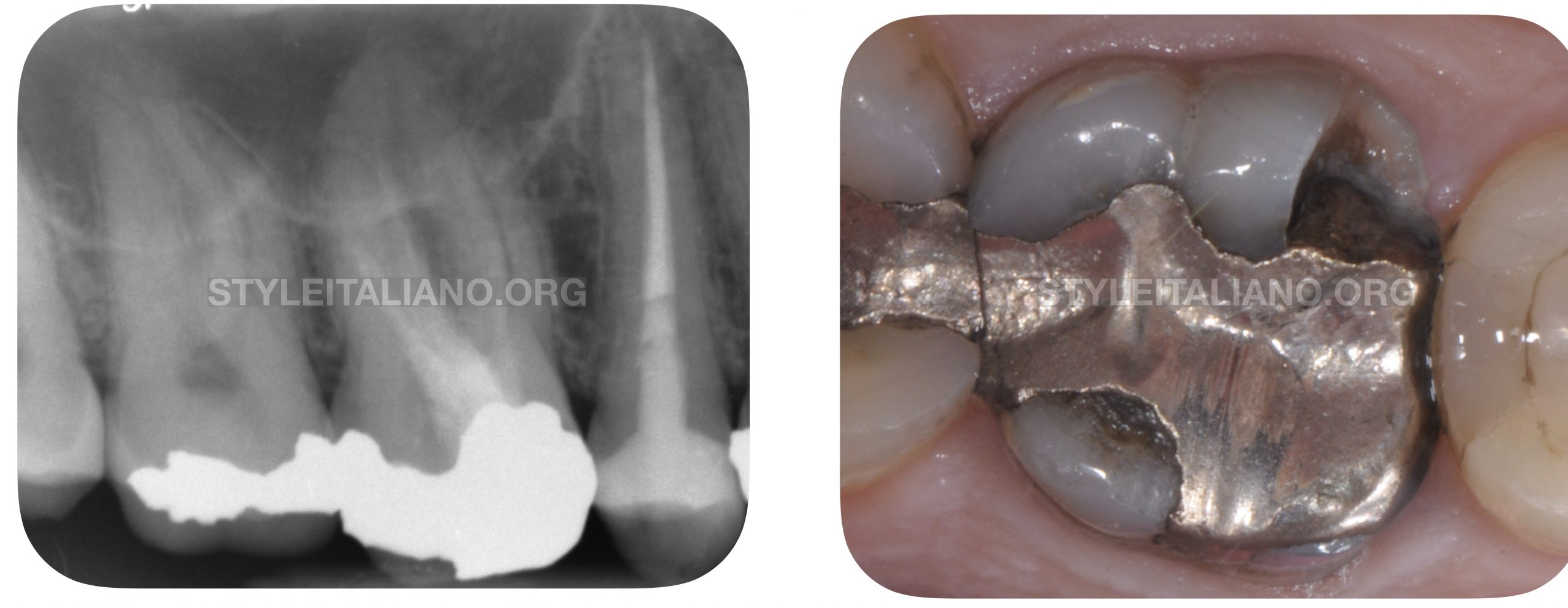
Fig. 3
The 43-year-old patient comes to the office for the fracture of a pre-existing amalgam restoration in a tooth previously endodontically treated.
The tooth on clinical examination is painful to percussion and palpation of the mesiobuccal root which presents a swelling.
The radiographic examination shows the presence of a lesion to the mesiobuccal root associated with a pre-existing incongruous endodontic treatment.
It is suggested as treatment plan to perform an orthograde retreatment and to restore with a full covarage cusps indirect restoration the tooth.

Fig. 4
Before proceeding with the removal of the amalgam it is necessary to isolate the operating field with a rubber dam to reduce the ingestion of mercury powder by the patient.
This also constitutes an important barrier for the operator and the assistant against the aerosol produced.
The multiple isolation in this case allow an immediate restoration at the end of the endodontic therapy if necessary.

Fig. 5
The removal of the amalgam takes place with multi-blade tungsten carbide burs, along the limits of the restoration, taking care not to touch the dental walls, sometimes very thin or undermined with the risk of breaking. The quality of the underlying dental tissue is then assessed: carious tissue is eliminated and the thickness of the residual walls is evaluated in order to plan already at this moment the type of final restoration whether with partial or total cusp coverage.
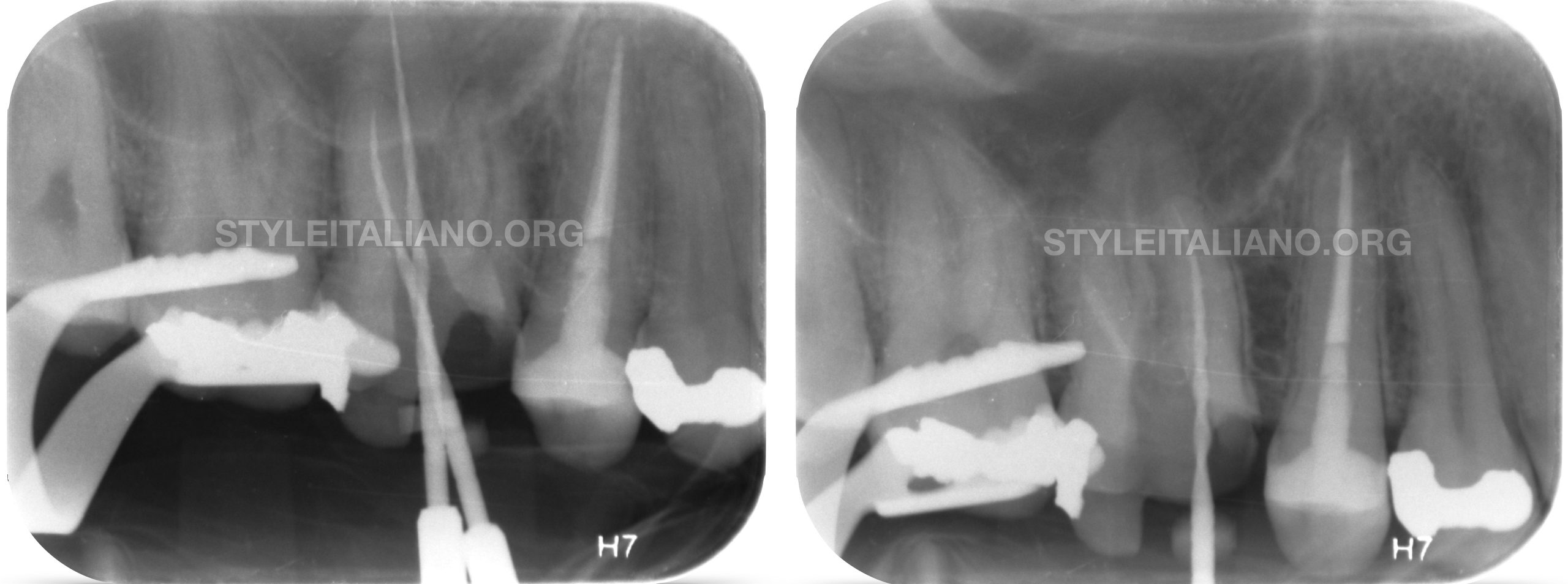
Fig. 6
After removing the amalgam we proceed to the identification of the main canals (MB, DB, P), the removal of coronal interferences (preflaring) if present, the scouting with K-file up to the correct working length and t the cleaning and shaping. The correct working length of the main canals was estimated with the last mechanical file brought to the working length. It was only after this step that the accessory canal (MB2) was identified, scouted and cleaned & shaped.
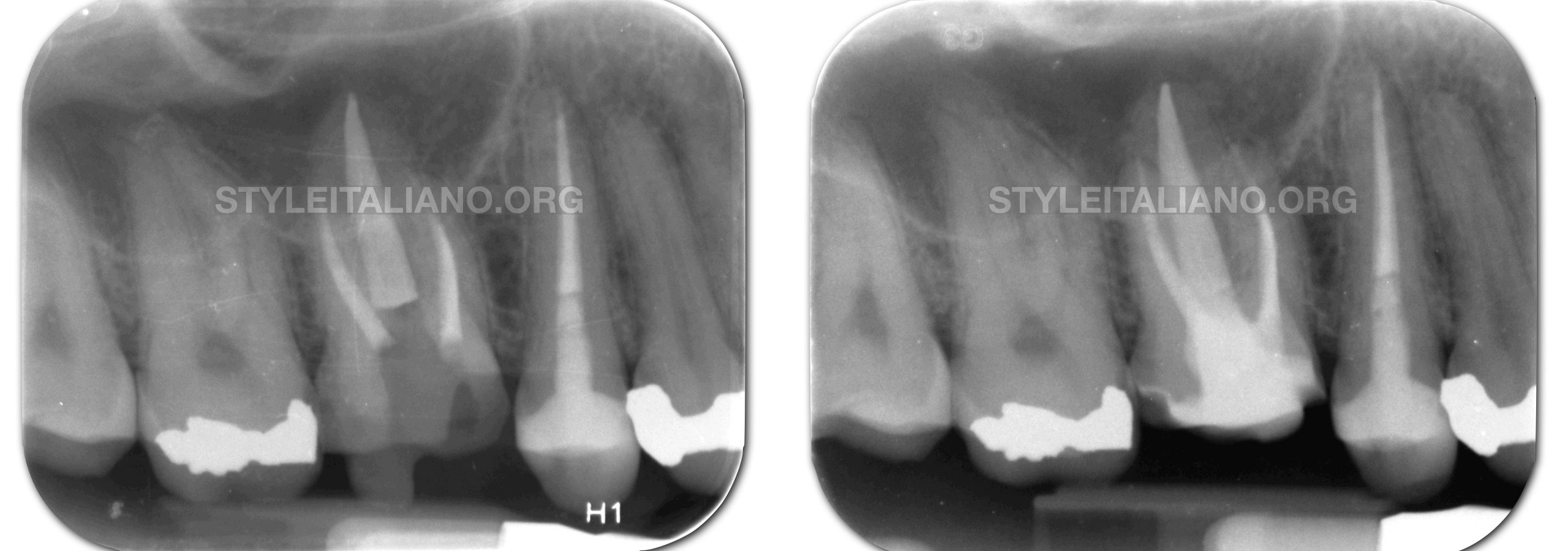
Fig. 7
The canals were all closed with the continuous wave of condensation. After performing a control x-ray to evaluate its correct execution, the tooth was rebuilt with a composite build-up and prepared for a definitive full coverage restoration. In the same session, the impression was taken after the preparation.
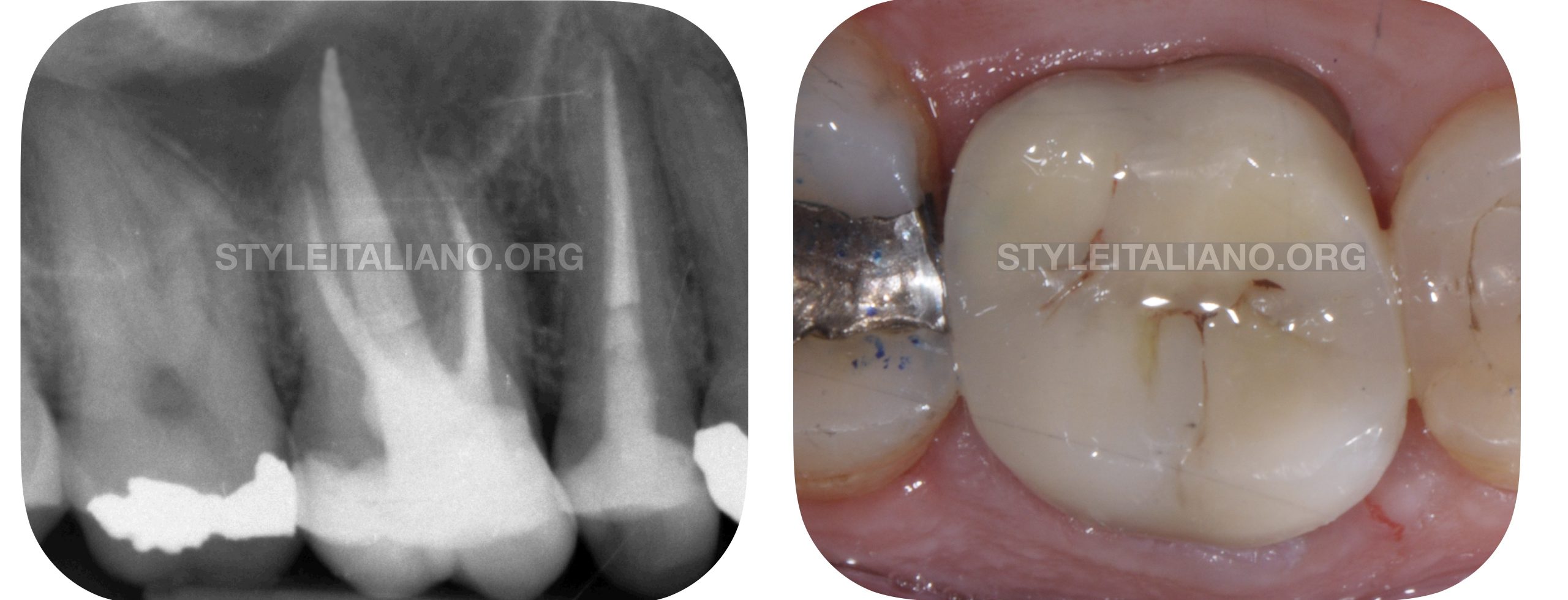
Fig. 8
Photo and x-ray of the dental element as soon as the cusp-covered restoration is cemented.

Fig. 9
seven-year check-up where the physiological deterioration of the composite restoration is observed, however accompanied by maintenance of the correct coronal and apical seal.
Conclusions
In this first article of a series of 5 was shown the correct prtocol in the case of re-access on an orthograde retreatment of a amalgam restored tooth.
The recommendations are the following:
- evaluate the possibility of ortograde retreatment not only from an endodontic perspective. The long-term prognosis has to be considered even after the restoration step(and what is connected to) and also the possible alternatives.
- isolate the operating field
- remove the amalgam restoration as quickly as possible with new multi-blade tungsten carbide burs
- once the existing restorations, carious tissue and unreliable dental structures have been removed, the type of restoration planned has to be evaluated properly
- reconfigure the access cavity
- find the main canals, scout, clean and shape them
- find the accessory canals, scout, clean and shape them
- perform the obturation of the root canal system
- if it is possible perform an immediate composite build-up or in the absence of time, place a temporary restoration by planning the subsequent restoration step
Bibliography
Scianamblo MJ: Endodontic failures: the retreatment of previuosly endodontically retreated teeth, Revue Odontostomatol (Paris), 1988
Parreira FR et al: Cast prosthesis removal using ultrasonic and thermoplastic resin adhesive, J Endod, 1994
Carr GB: Retreatment. In Cohen S, Burns Rc, editors: Pathways of pulp, 1998
Koral SM. IAOMT Safe Removal of Amalgam Fillings. International Academy of Oral Medicine & Toxicology; 2007