Redefining the access in retreatments: Part IV of V
22/11/2020
Enrico Cassai
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
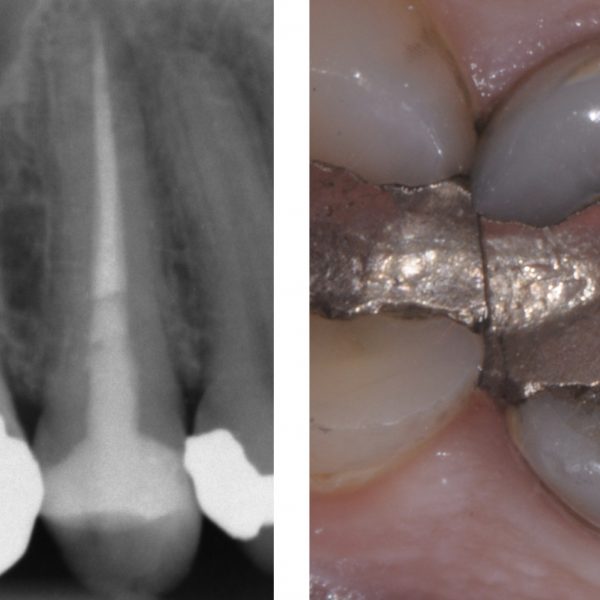
In the context of retreatments and re-access, sometimes it happens to perform a new endodontic therapy recovering the old prosthetic crown.
A careful preoperative evaluation can allow the clinician to pick the best therapeutic choice and to address the wishes of the patient.
The need to maintain the old prosthetic crown may arise from the willingness of the patient or of the colleague who sent the patient or from a choice of the clinician.
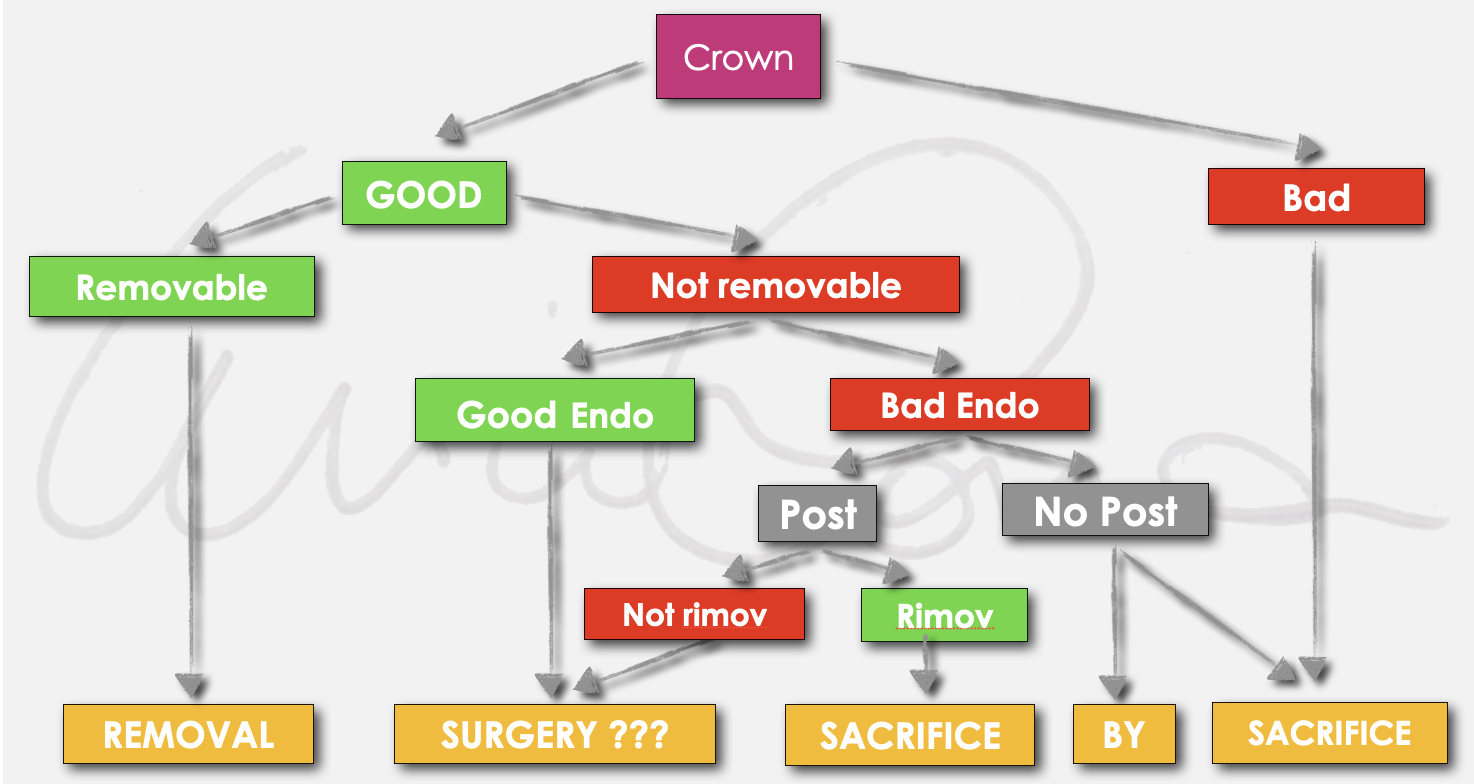
Fig. 1
The choice that the clinician must make in the presence of a pre-existing crown is related to a series of factors that can be summarized in Diagram 1.
It will be necessary to carefully evaluate the quality of the coronal restoration in terms of seal, aesthetic and function.
Secondly, to analyze the presence of accessory retention such as posts, considering their position, length and possible removal.
Finally, he will have to focus his attention on the quality of the endodontic treatment, thinking about the possible presence of iatrogenic errors such as blocks and / or ledges that make it difficult or impossible to reach a new apical seal.
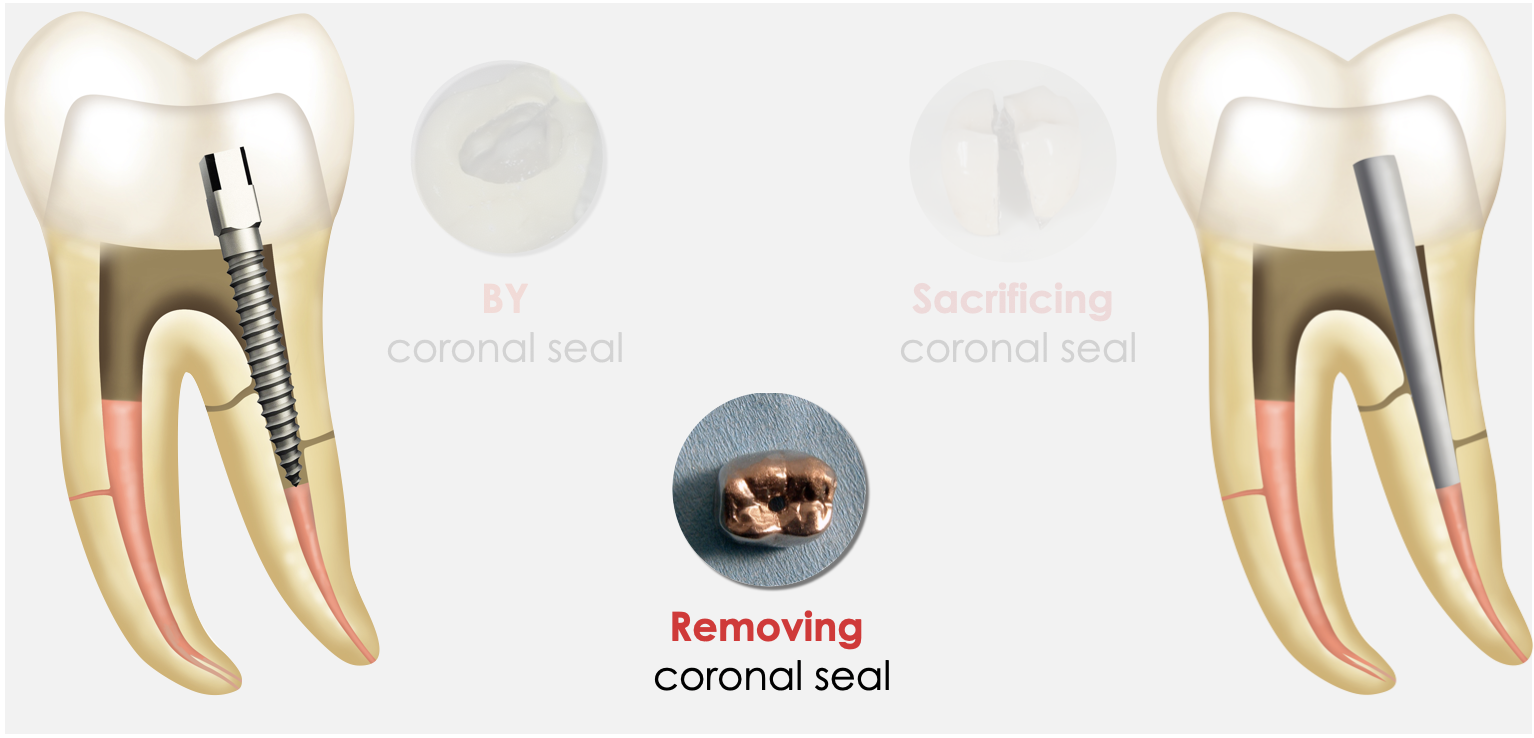
Fig. 2
If the choice of the clinician is linked to the maintenance of the pre-existing prosthetic crown, its removal should be done in the most atraumatic way (Diagram 2).
This is a choice that I personally do not prefer, but sometimes I find myself forced to proceed by the will of the patient or especially of the colleague who sends him/her.
The maintenance of the pre-existing prosthetic crown depends on its quality in terms of seal, aesthetics and function: vice versa, the treatment plan should be modified.
Another aspect to consider is the maintenance of the abutment in its almost complete integrity after the removal of the crown, otherwise problems with marginal seal and adaptation of the crown could arise after the end of the endodontic treatment.

Fig. 3
The atraumatic removal of the crown in order to be able to reuse it after the end of the endodontic treatment can take place through the use of different devices.
It is necessary to try to maintain its structural integrity for marginal seal, aesthetic seal (avoiding chipping of the covering material or of the intoto material).
In the hypothesis that during the disassembly step the crown suffers significant damages, it is necessary to consider removing it and replacing it.
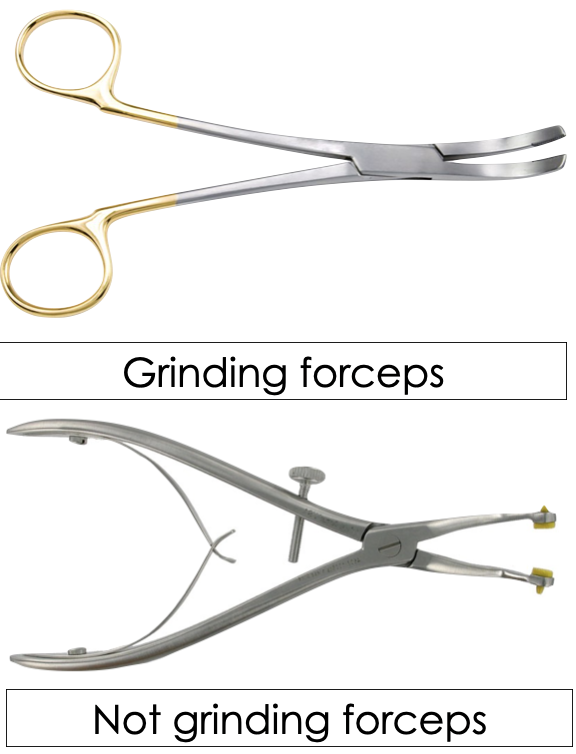
Fig. 4
The first opportunity to completely remove a pre-existing crown is to use special forceps.
The forceps for temporary crowns in resinous materials or totally metallic crowns have frictioning branches to increase the grip. They must not be used against crowns in ceramic material. otherwise the crown would be scratched.
The forceps for crowns in ceramic material have the branches covered with a silicone sleeve to prevent scratches.
In both cases the system only works if the crown has been temporarily cemented.

Fig. 5
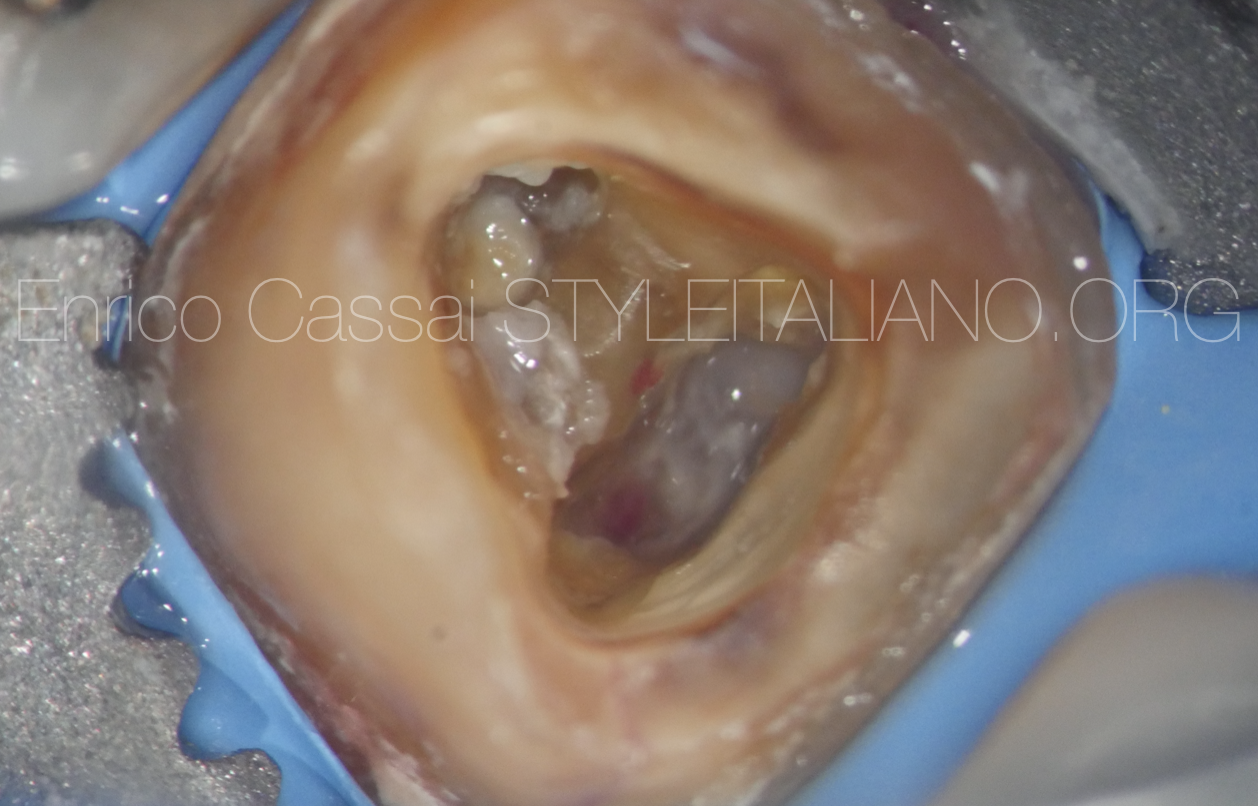
Fig. 6
After removing the pre-existing crown and designing the preliminary access cavity
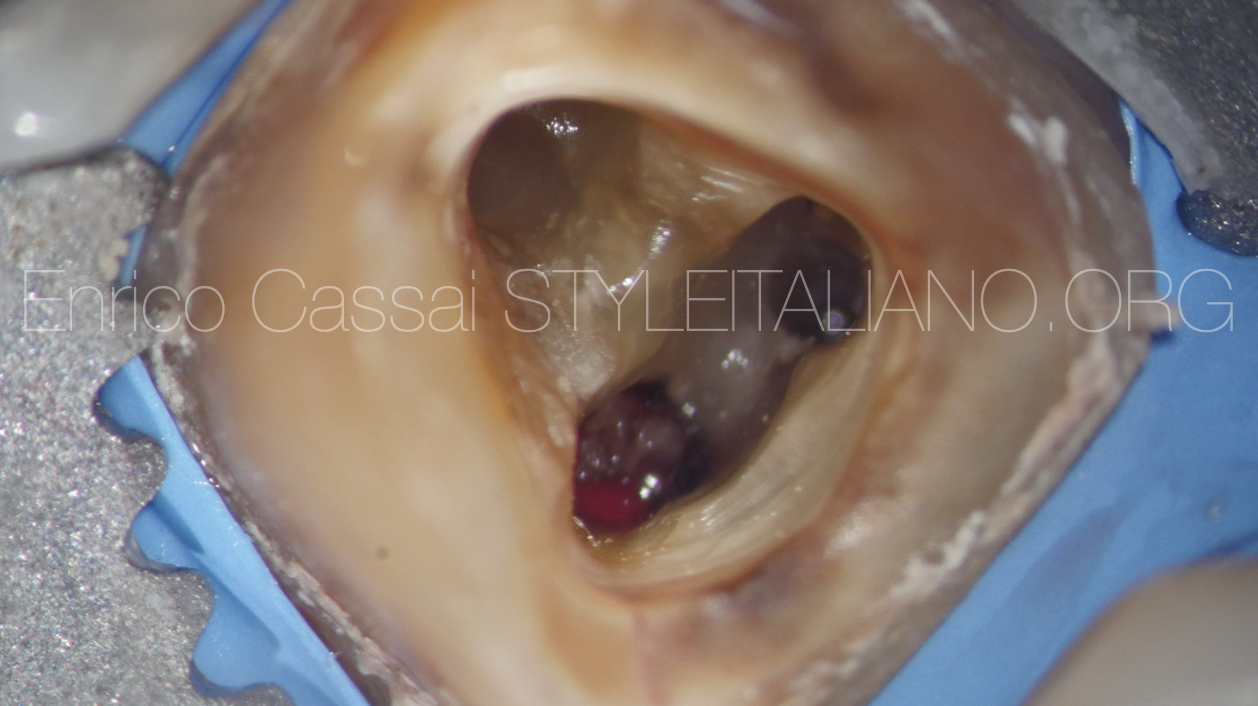
Fig. 7
Access recontouring and main canals identification: ML, D. Not clear the position of MB
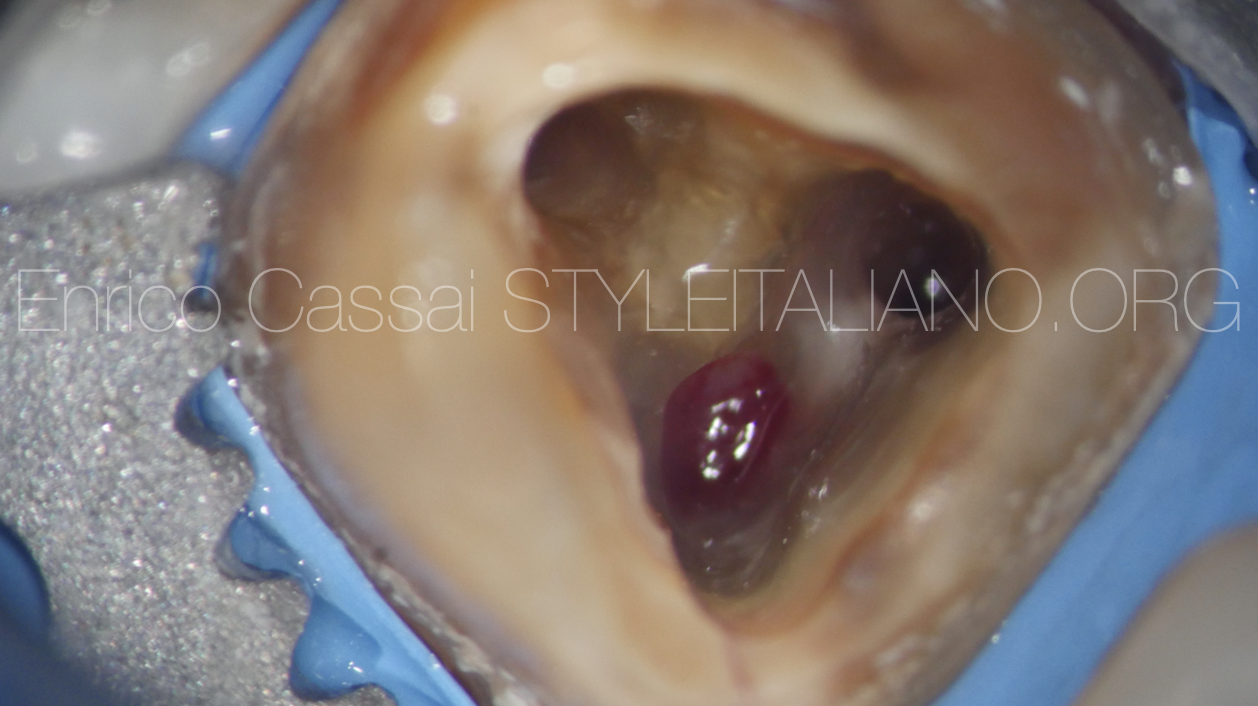
Fig. 8
Looking to the position of the blood coming out from the MB canal, it seems not in the correct position
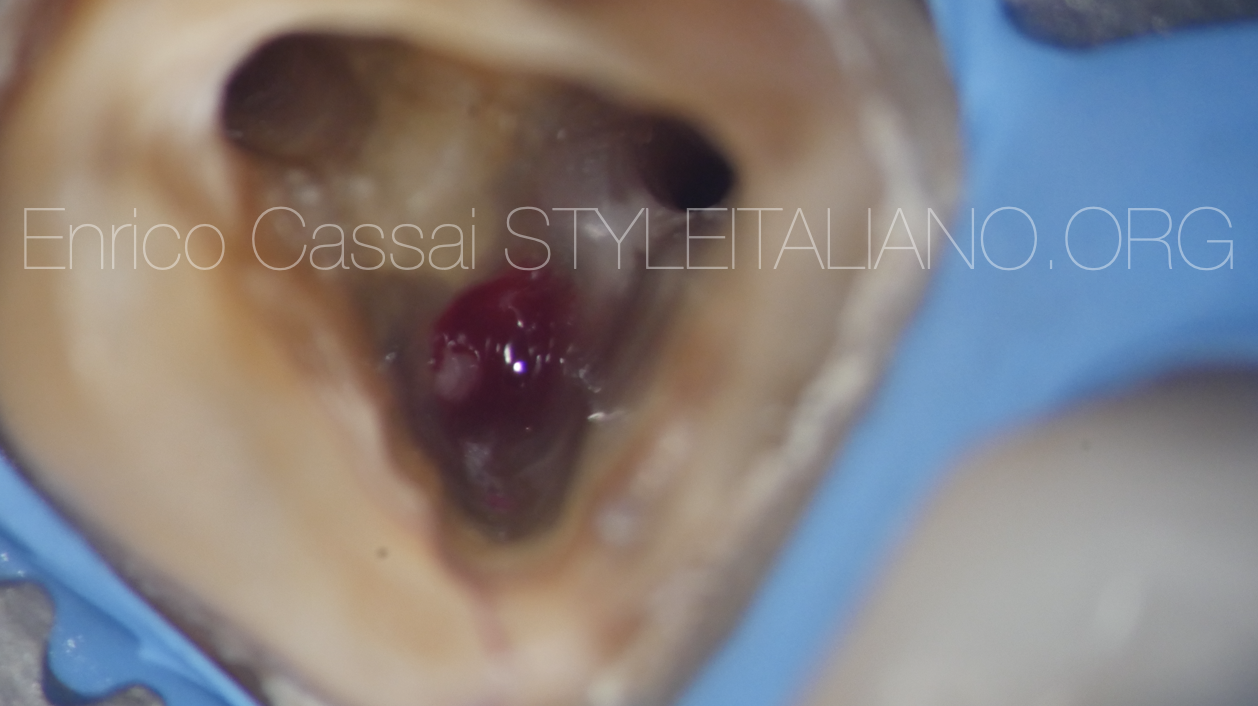
Fig. 9
In fact, it appears a bleeding point more buccally

Fig. 10
Using an endodontic probe and a micro-opener I found the MB and enlarged the orifice

Fig. 11
The MB was scouted until reaching the Working length.

Fig. 12
The picture shows the position of the MB canal and the perforation that should be treated

Fig. 13
The MB canal was shaped until the working length.

Fig. 14
Detail of the shaped canal

Fig. 15
All the canals were shaped and were ready to be filled

Fig. 16
Before filling the canals I treated the perforation. I put a gutta-percha point in both mesial canals to avoid the MTA to fall into them
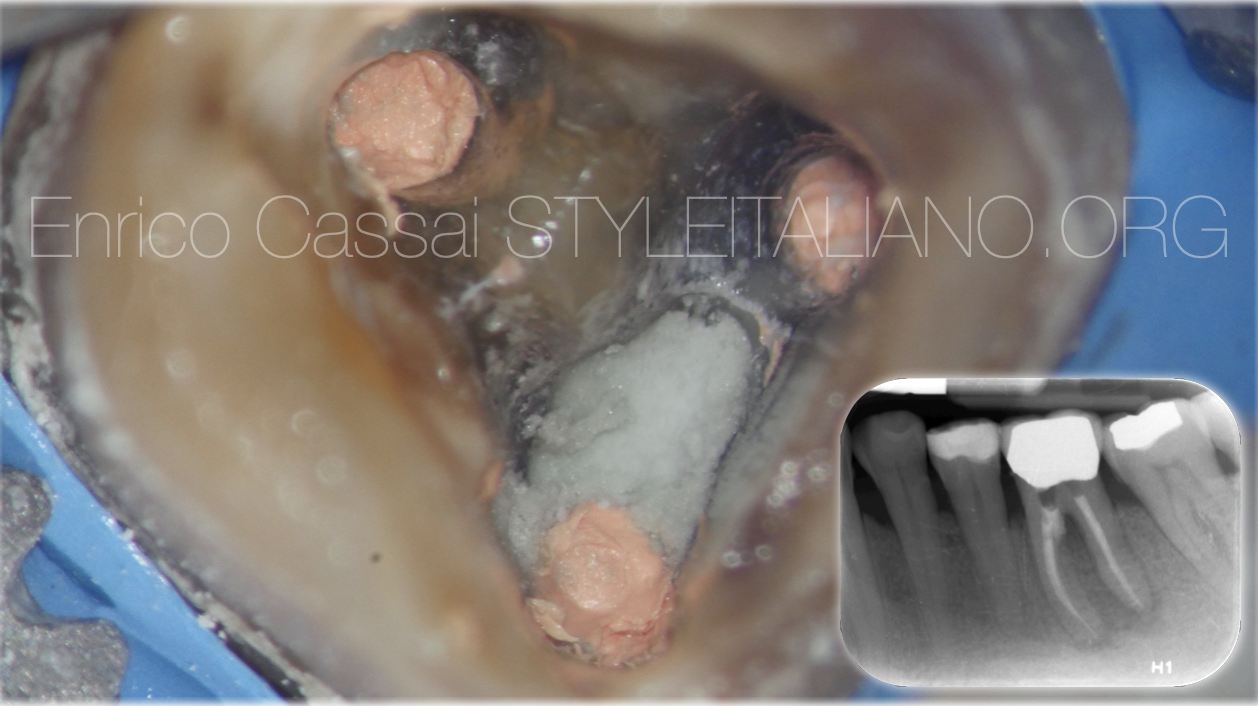
Fig. 17
After checking the hardening of MTA I executed the final obturation of all canals with the continous wave of condensation technique.

Fig. 18
A significant portion of the dentist's energy or that of the instrument being used is absorbed by the periodontal ligament:
- pain felt by the patient
- luxation of the ligament
It is virtually impossible for the dentist to be certain that forces are being directed precisely to the same axial direction as the crown's path of insertion. For this reason, the dentist generally proceeds with a series of light, off-center tapping movements. Abutment fractures are therefore common

Fig. 19
Among the most reliable percussion systems in removing a pre-existing definitively cemented crown, there are some dedicated devices.
In this case the force that is exerted to remove the crown is adjustable and never excessive, so the risks of abutment fractures are reduced.
These type of device can be used both for removing single crowns and bridges.

Fig. 20

Fig. 21
Another category of active system for removing a pre-existing crown includes devices that partially modify the structural integrity of the crown.
These are devices in which it is necessary to drill a hole on the occlusal or axial face of the crown and then insert levers or devices that allow complete decementation.
The crown can be reused at the end of the endodontic treatment but will show repairs along its surface with little loss of seal and aesthetics.
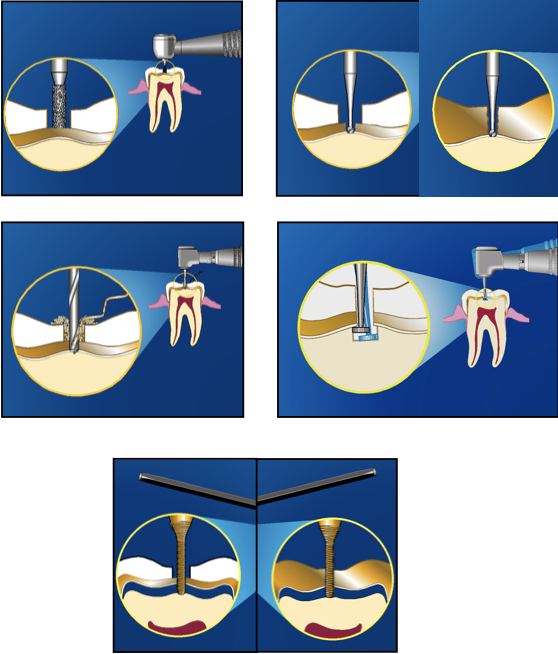
Fig. 22
With this type of devices follow this steps:
- Expose the metal with a bur
- Make a pilot hole through the metal crown only (No penetration into tooth structure or core material)
- Make a precision channel with dedicated bur
- Undermine the metal structure if present
- Turn the device with finger pressure in a clockwise direction until feel the resistance of the cement layer and the crown lift coronally

Fig. 23
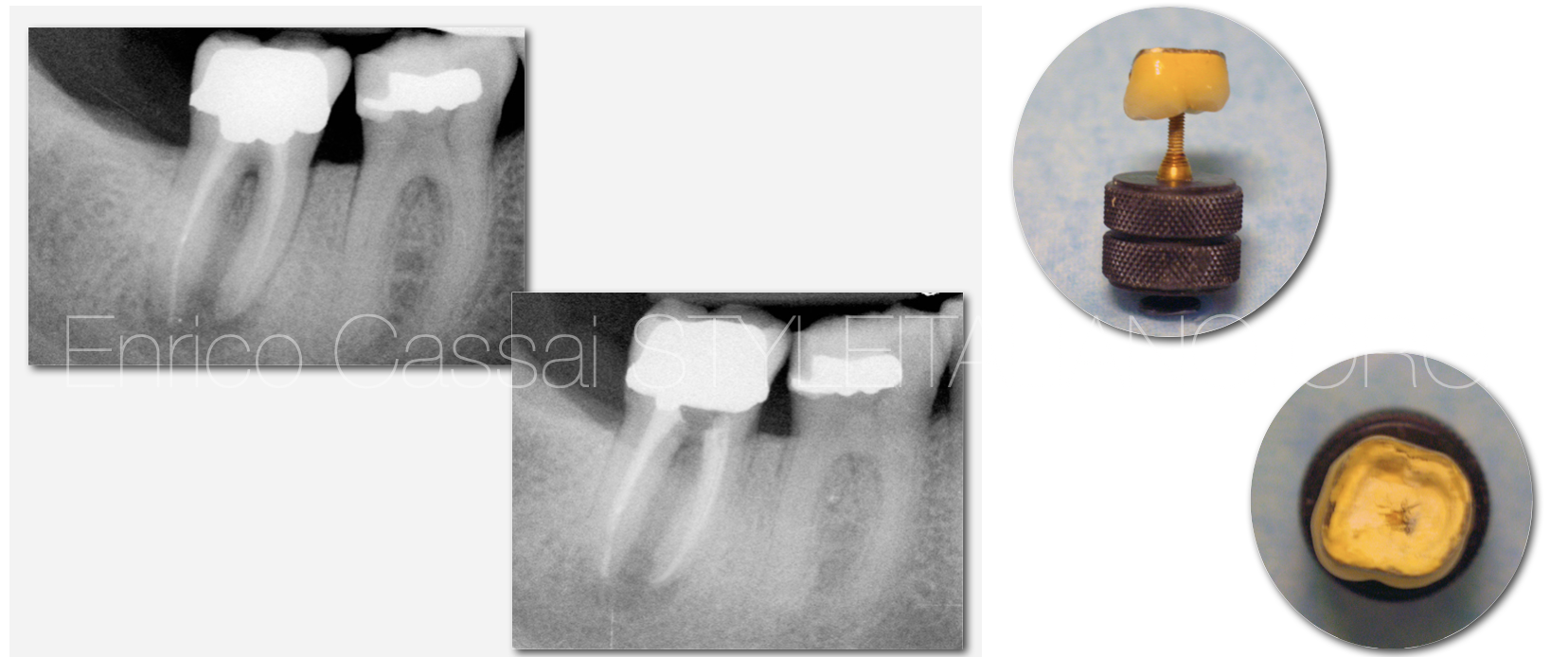
Fig. 24
Conclusions
In this fourth article of a series of 5 was shown the correct protocol in the case of re-access on an orthograde retreatment of preexisting crown.
The recommendations are the following:
- take always a CBCT beside an initial x-ray
- study with accuracy any diagnostic preoperatory investigation in order to intercept in advance any possible problem during the therapy (missed canal, curvatures, blocks, ledges,…)
- reuse the preexisiting crowns only if seals well and is aesthetically correct or in presence of willingness of patient or clinicians who send the patient. Otherwise consider the opportunity to remove it and do it another one new
- use the device that allows the complete removal of the pre-existing crown with no or minimal integrity loss of the crown
- consider this option not as prior choose and the reused crown should be considered as provisional crown in my opinion
Bibliography
Scianamblo MJ: Endodontic failures: the retreatment of previuosly endodontically retreated teeth, Revue Odontostomatol (Paris), 1988
Parreira FR et al: Cast prosthesis removal using ultrasonic and thermoplastic resin adhesive, J Endod, 1994
Carr GB: Retreatment. In Cohen S, Burns Rc, editors: Pathways of pulp, 199
Girard JL: Advancement in the removal of permanently cemented crowns and bridges, Smile Dent J, Vol 5, Issue 4, 2010
Westermann R: A System for Treating Crown-and-Bridge Failures, Dentistry Today, 1996
Retreatments, Edra