RADICULOUS/ SMALL MOLARS/ MOLARIZED PREMOLARS/ THREE CANALLED MAXILLARY PREMOLARS- HOW TO IDENTIFY AND MANAGE THEM
06/01/2023
Garima Poddar
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2


Fig. 1
Tools and techniques helpful in detection of a three canalled premolar are as follows-
Tip while reading the radiograph-
a). Sieraski et al suggested, that a maxillary premolar is likely to have three roots when the mesio-distal width of the mid root image is equal to or greater than the mesio-distal width of the crown.
b). 2-3 intraoral pre-operative x-ray images at different angulations could give more details of the roots and canal configuration.
c). In case of a split of the buccal canals – identifying a point of “fast-break” could hint the presence of extra canal.

Fig. 2
Tips for acces cavity modifications-
Maxillary premolars with three canals need access cavity refinement by broadening the outline on the buccal aspect mesio-distally to permit good access to each of the two buccal canals.
Extending the cavity design into a “T” shape helps locate and instrument the mesio buccal and disto buccal canals with ease.

Fig. 3
Tip while shaping the canals-
While shaping, its important to understand that for successful management of the narrow buccal canals, over enlargement should not be attempted as excessive canal preparation could result in a lateral “strip” perforation. The roots are usually very slender and narrow in such teeth.
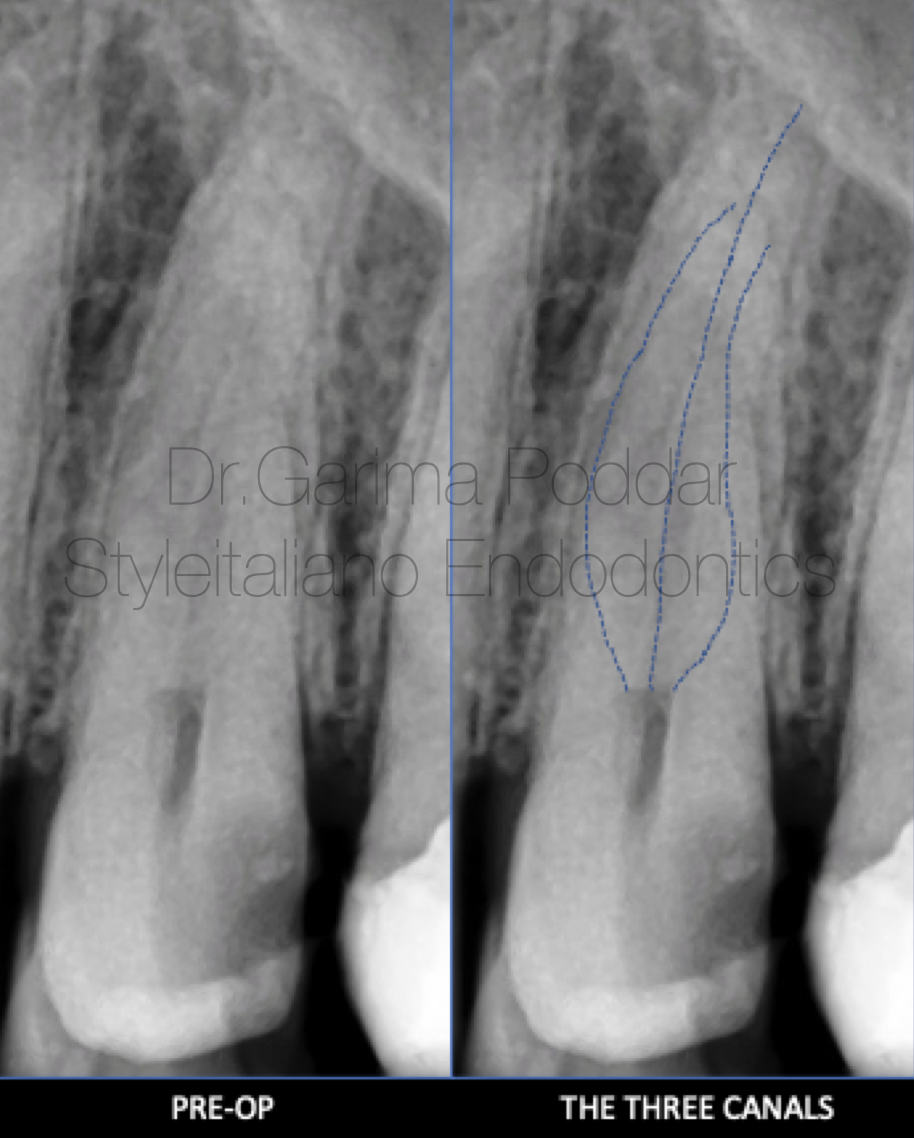
Fig. 4
CASE REPORT 1-
A 35 year old male patient reported to our hospital with pain and tenderness in maxillary left posterior region.
On clinical examination it was observed that tooth number 24 and 25 were symptomatic.
Diagnosis of chronic irreversible pulpitis was made with the help of pulp tests, clinical and radiographic evaluation.
On the pre-operative x-ray, faint radiolucent lines could be traced guiding towards the presence of three canals in maxillary first premolar.
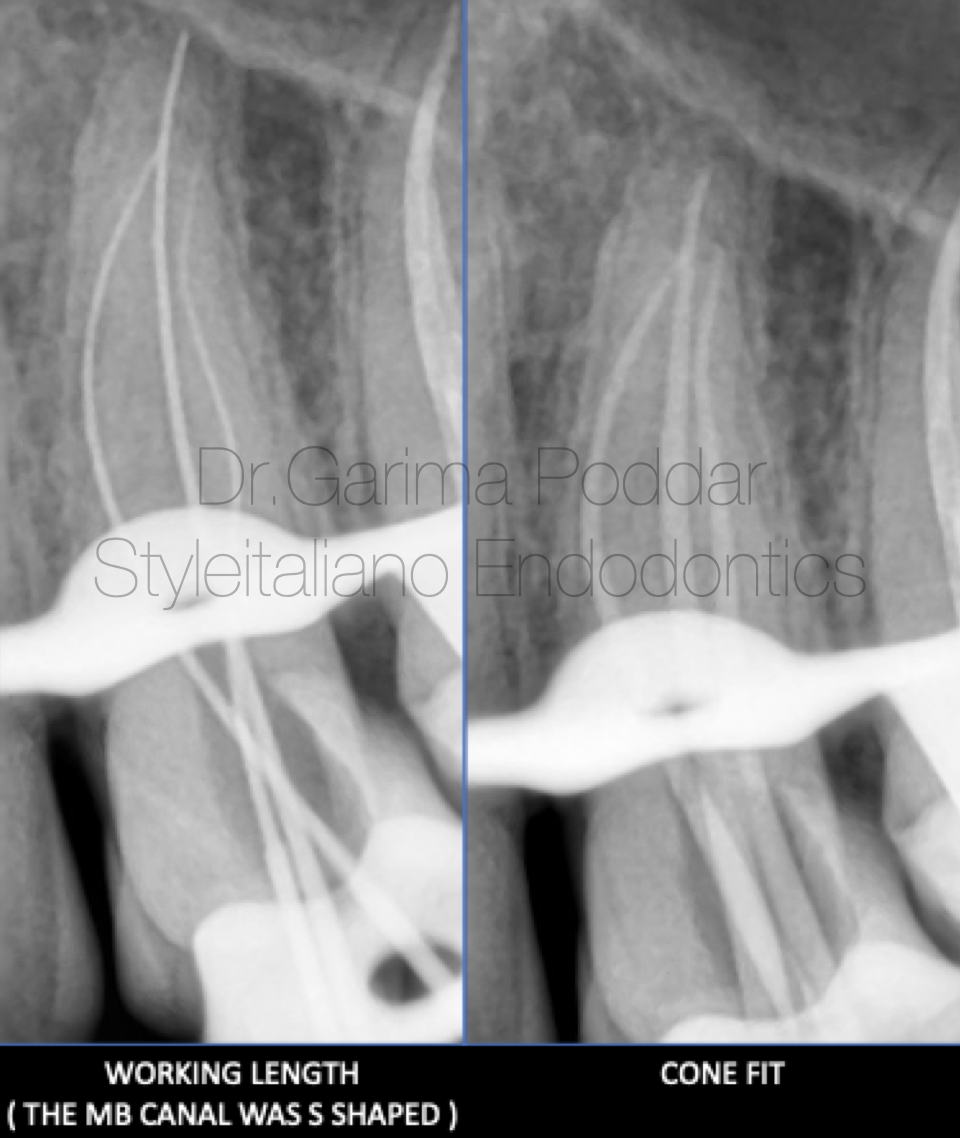
Fig. 5
Local anesthesia was administered and rubber dam isolation was done. Access preparation was done and a pre-endo build up was done.
Shaping protocol-
Coronal flaring with one flare file(Micromega, France) was done for all three canals.
Hand instrumentation with 8K, 10K, files was performed till working length which was determined using electronic apex locator and confirmed on a radiograph.
OneG files were used for glidepath preparation and shaping was done up till 25-04% files using 2 shape files ( Micromega, France).
Irrigation protocol-
5.25% sodium hypochlorite, distilled water and 17% EDTA were used for thorough irrigation and the solutions were ultrasonically activated.
Obturation protocol-
Cone fits for all three canals were confirmed. Bio ceramic sealer( Ceraseal, Meta biomed) with single cone was the technique of obturation for this case.
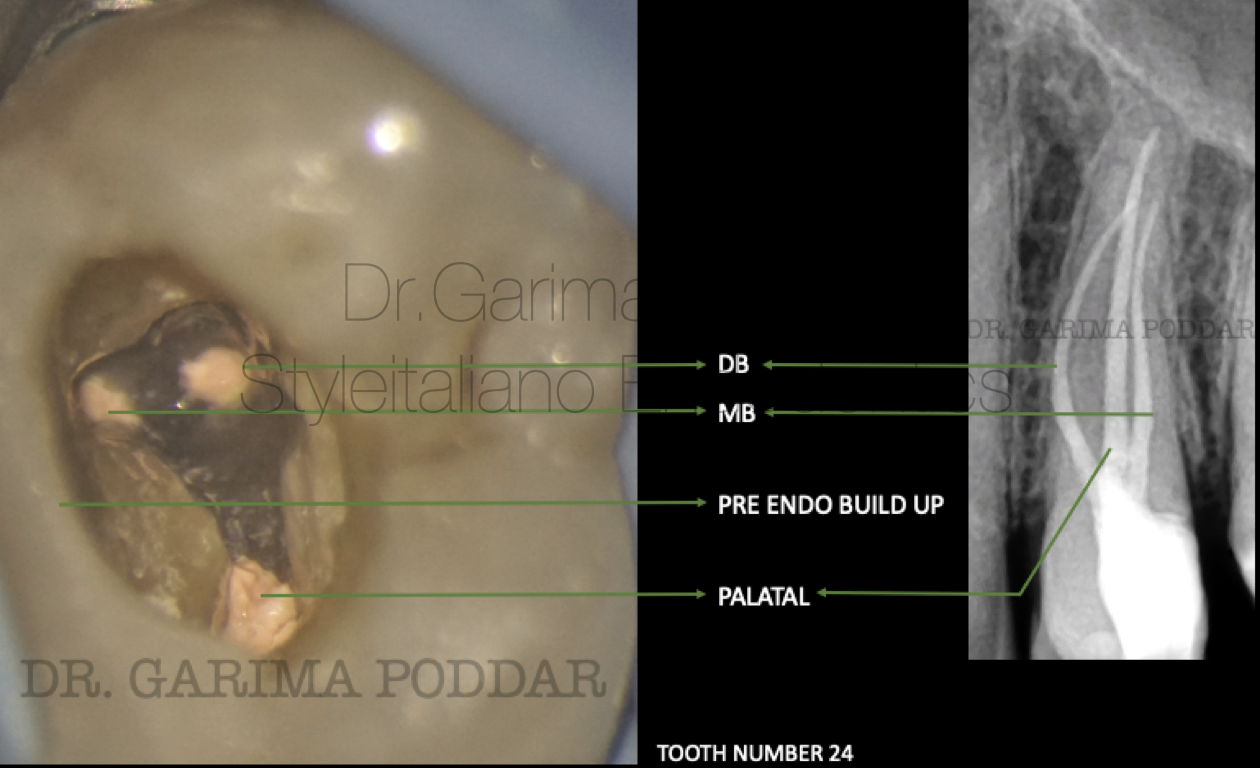
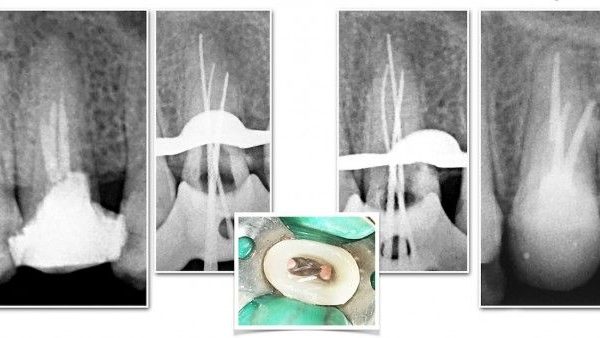
Fig. 6
Core build up post endodontic treatment was done using paracore (coltene).
The case was referred for further prosthetic rehabilitation to referring dentist.

Fig. 7
CASE REPORT 2-
A 37-year-old female patient reported to our hospital, with severe pain and tenderness in maxillary first premolar of right side for 20 days. On clinical examination, a deep carious lesion was observed in tooth number 14.
The tooth was tender on percussion. Radiographic examination confirmed the diagnosis of irreversible pulpitis in 14.
Radiographic evaluation revealed the following-
1. Deep disto proximal decay in 14 involving pulp.
2. An unusual anatomy in the buccal canal in apical third region.

Fig. 8
The tooth was isolated using rubber dam isolation and caries was excavated completely.
Access preparation was done. Initially only two main canals, that is buccal and palatal canals could be negotiated. Later on, angulated view radiograph was made using tube shift technique, and a point of “fast break” was seen after which the radiolucent canal outlines were not easily traceable on the x-ray.
This hinted towards presence of a split and an atypical canal anatomy. A buccal split was suspected and then it was scouted using an 8K and 10K files. The treatment was performed under magnification, using a dental operative microscope, which proved to be really helpful because of better magnified view and good illumination. Also, a detailed study of the pre-operative radiograph provided a clue for the presence of an unusual anatomy.
Shaping Protocol -
Coronal flaring was done using One Flare File (Micromega, France).
10K file was used to instrument the canal till in became loose in both the splits
Glide path preparation was done with the help of One G File (Micromega, France).
The palatal canal and mesio buccal canals were shaped using One-Reci Files (25-06%) (Micromega, France). The distobuccal split was negotiated first using manual K files number 8 and 10 and then with the help of a gyromatic hand-piece – K400, further shaping was done till 20K file for this split.
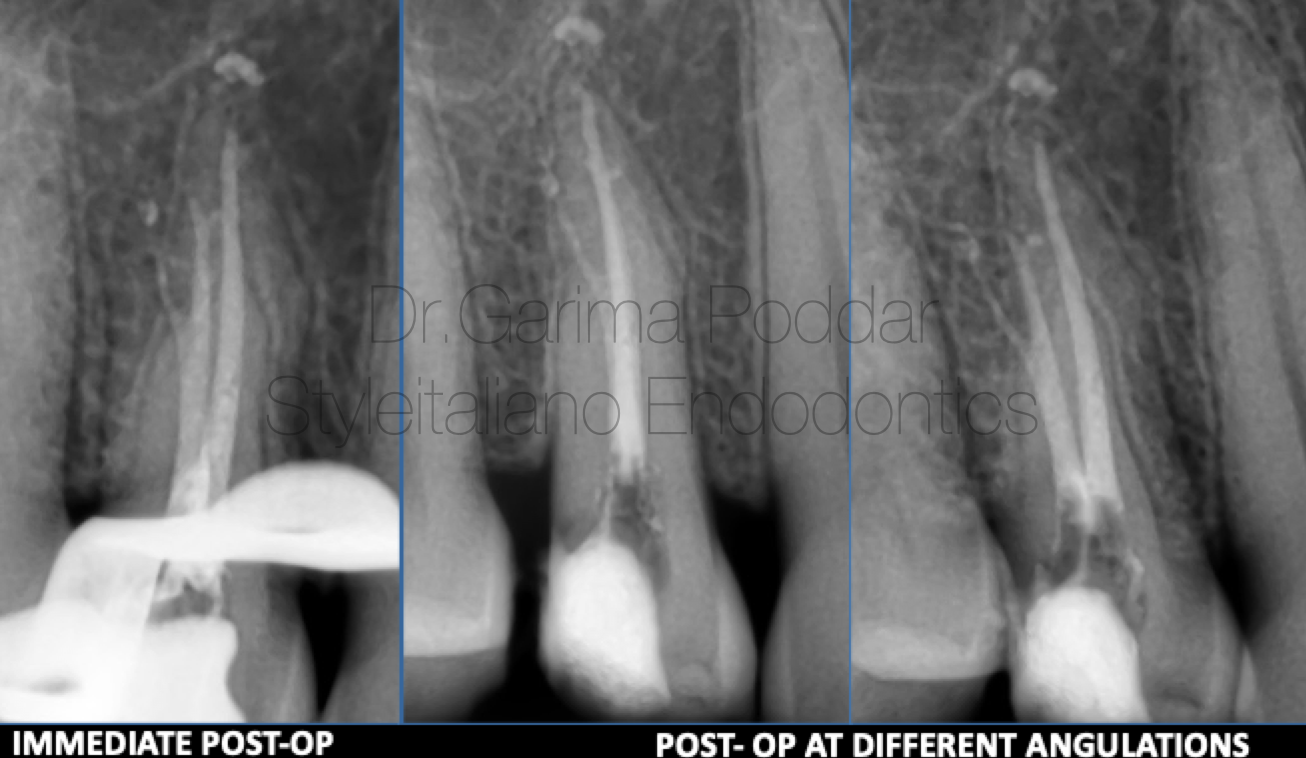
Fig. 9
Irrigation Protocol
Throughout shaping, 5.25% sodium hypochlorite was used after each file. Side vented 30 gauge needles were used for irrigation.
After shaping, the following protocol in each canal, was used for irrigation and activation of irrigants-
1. 17% EDTA – 1ml per canal – ultrasonic activation.
2. Distilled water used to flush the canals.
3. 5.25 % sodium hypochlorite - ultrasonic activation. (4 such cycles repeated per canal)
4. Distilled water.
Obturation Protocol
Canals were dried with paper points. Cone fit intra oral radiograph was made.
One split was blocked by inserting a paper point and gutta percha cone was inserted in the other split and then the paper point in the other split was also replaced with cone. Canals were obturated with warm vertical compaction technique using EQ-V (Meta Biomed). Sealer used was Ah Plus (Dentsply Maillefer).

Fig. 10
Post Endodontic Restoration
Core build up was done for 14, using composites. A full coverage crown was given on 14.
Fig. 11
Sometimes, the two buccal canals emerge from a common narrow canal which originates from the pulp chamber.
In this case also, same configuration was encountered.
Pre-flaring the canal orifice, makes the negotiation and instrumentation of such deep splits easier.

Fig. 12
CASE REPORT 3-
A 44 year old male patient reported with pain and tenderness since 10 days in maxillary left posterior tooth to our hospital.
On examination it was observed that the patient has continuous pain and tooth number 24 was tender on percussion. There was a deep proximal decay present, and patient also complaint of food lodgement.
A diagnosis of acute irreversible pulpitis was made.
On pre-operative radiographs the following details were observed-
- Deep disto proximal decay with pulp exposure.
- Sudden loss of radiolucency in the pulp chamber.
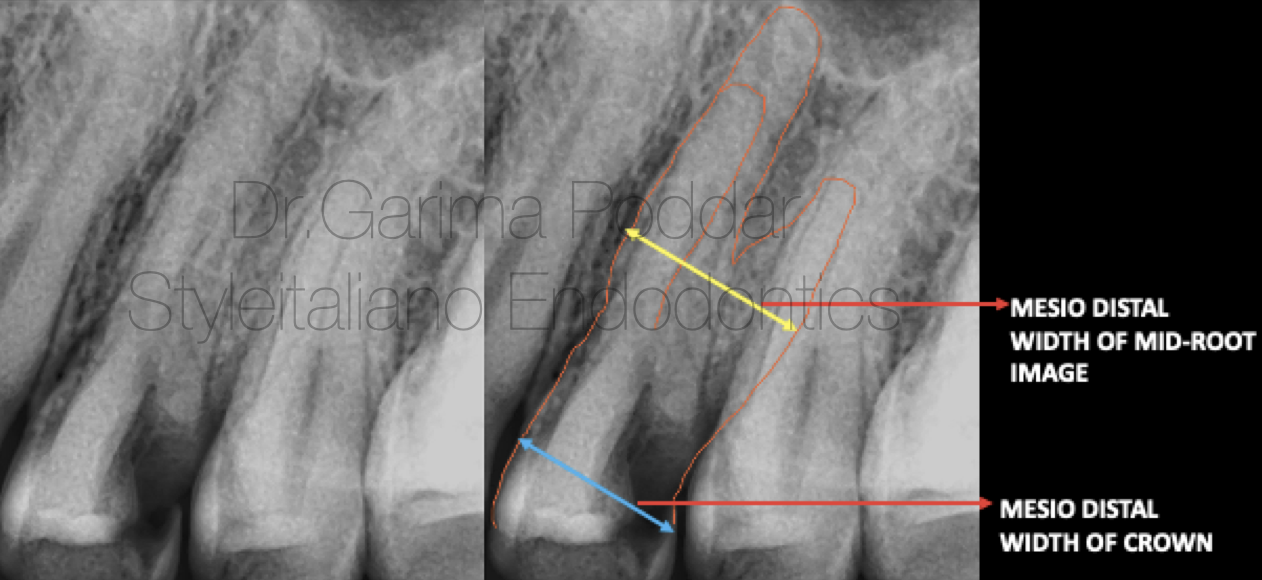
Fig. 13
Mesio-distal width of mid root greater than the mesio distal width of the crown.

Fig. 14
Local anesthesia was administered.
Rubber dam isolation was done.
Caries was excavated and access preparation was done. The access cavity was modified into a ”T ” shaped design with more widening than usual of the buccal aspect.
Three canals, namely- mesio buccal, disto buccal and palatal were found.
Shaping Protocol
Coronal flaring was done using One Flare File (Micromega, France).
Hand instrumentation was done with 8 and 10 K files followed by which glidepath was prepared with the help of one G file( Micromega).
Shaping was done using 2 shape files ( Micromega, France).

Fig. 15
Obturation protocol-
Master cones were finalised after confirming their tug backs.
Bioceramic sealer (Ceraseal, Meta biomed) with single cone was used for obturation.

Fig. 16
Post endodontic core build up was done using warm composites.
Conclusions
In depth knowledge of variations in the root canal anatomy is important in order to not miss an anatomy during endodontic treatment of a tooth.
In today’s practice, due to use of advanced tools like magnification, good illumination and radiography tools like CBCT, chances of diagnosing and treating atypical anatomy has increased by many folds.
However, a basic intra-oral radiograph also, when utilized properly could divulge the required details for endodontic management of a maxillary premolar.
Appropriate access cavity refinement is always helpful in identifying extra canals and also aids in easy instrumentation and hassle free obturation of the canals.
Bibliography
1. Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol. 1984;58:589–99.
2. Vertucci FJ, Gegauff A. Root canal morphology of the maxillary first premolar. J Am Dent Assoc. 1979;99:194–8.
3. Walker RT. Root form and canal anatomy of maxillary first premolars in a southern Chinese population. Dent Traumatol. 1987;3:130–4.
4. Senan, E.M., Alhadainy, H.A., Genaid, T.M. et al. Root form and canal morphology of maxillary first premolars of a Yemeni population. BMC Oral Health 18, 94 (2018). https://doi. org/10.1186/s12903-018-0555-x
5. B. Dadresanfar, Z. Khalilak, and S. Shahmirzadi, “Endodontic treatment of a maxillary first premolar with type IV buccal root canal: a case report,” Iranian Endodontic Journal, vol. 4, no. 1, pp. 35–37, 2009.
6. Sieraski SM, Taylor GN, Kohn RA. Identification and endodontic management of three-canalled maxillary premolars. J Endod 1989;15(1):29–32.
7. Ingle J, Bakland L, Baumgartner JC. Ingle’s Endodontics, ed 6. BC Decker Inc, Hamilton; 2008.