Overfilling: malpractice or procedure error? Management of an acute apical abscess resulting from an extruding GP single cone obturation
03/08/2023
Marc Habib
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
From a medico-legal aspect, extrusion of root canal filling might be considered malpractice if there is excessive extrusion of material combined with incomplete obturation of the canal leading to failure of the root canal treatment.(1)
Acute Apical Abscess AAA is the most common form of dental infections and is caused by the infected root canal of the tooth.

Fig. 1
Warm vertical compaction obturation techniques are incriminated in a greater risk of extruded obturation material into the peri-radicular tissues. Extruded material can be gutta percha , gutta carriers and sealer regardless of its nature.
Today, the very popular single cone technique with calcium silicate BC sealer are creating enormous overfilling and sometimes reaching anatomical structure like the lower alveolar nerve and the maxillary sinus. Is this basically due to the sealer based principle of this obturation technique? Most likely, such extensive extrusion are not due to the flowability only of the premixed ready to use sealer but in fact mainly to the improper use of the material. It must be kept in mind, that traditional zinc based sealers might resorbs with time but calcium silicate sealers once set will most probably remain unchanged.
Does

Fig. 2
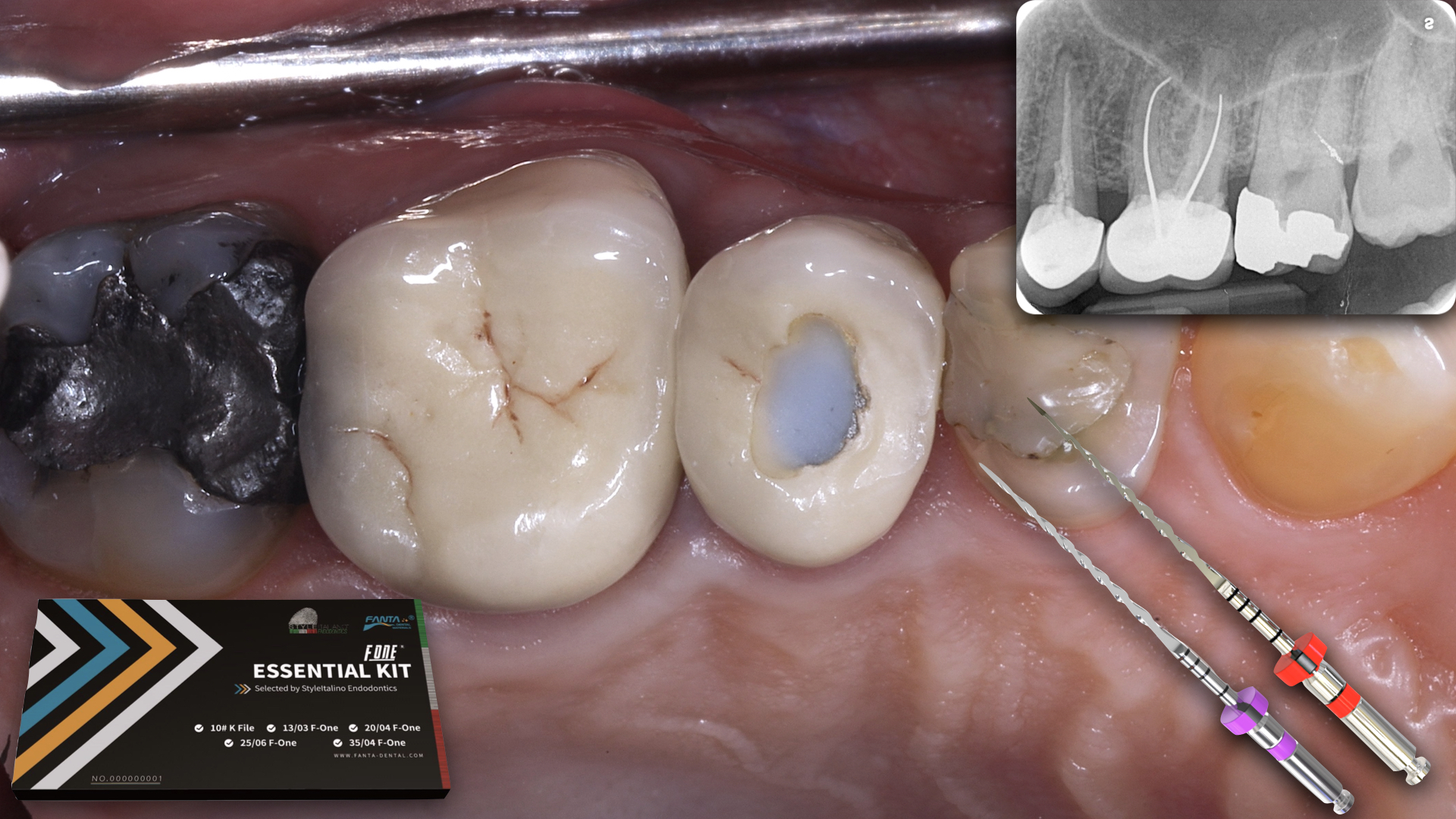
The following case report concerns a patient in his thirties who presented with pain symptoms corresponding to his maxillary left central incisor tooth #21.
Patient had a below nose swelling in the area of the apex of tooth #21, peri apical x-ray shows an overfilling with a gutta single cone and bone resorption around the apex of the tooth.The maxillary left lateral incisor was tested for vitality and was positively responsive. Patient describes a root canal treatment on his central incisor in a near by hospital three weeks earlier, he also highlights that it was at closing hours and the dentist was rushing things to finalize the treatment…A recipe for failure!
Many authors have reported high cytotoxicity for a variety of sealers and gutta-percha materials(2). This toxicity can induce inflammation and necrosis of the periradicular tissues(3).Consequently, overfilling can lead to failure of short term treatment like in this case or a negative long term prognosis.
pre Op Xray showing badly adapted obturation with gaps all around a single cone extruding something close to 3mm from the apex
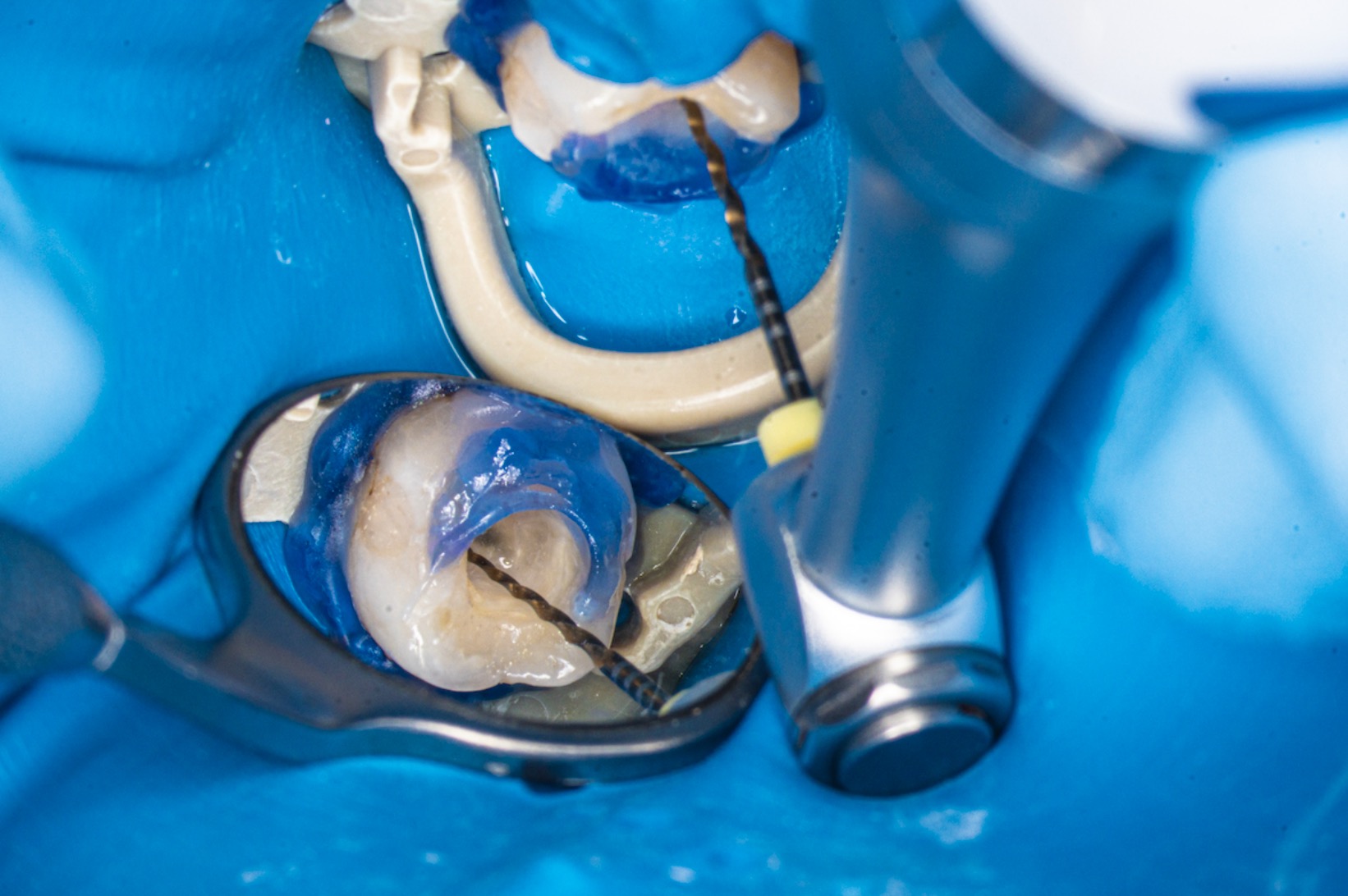
Step by step stages to gain access to the master cone and retrieve it without tearing it.
It is clearly visible that obturation was leaking with lots of fluids and gaps around the obturation material in the access cavity
Successful removal in one peace using Laschal file holder and stieglitz tweezers. Pus extrusion flushing from canal space explains pain generated from pressured pus underneath obturation.

Fig. 3
Retrieval of GP single cone
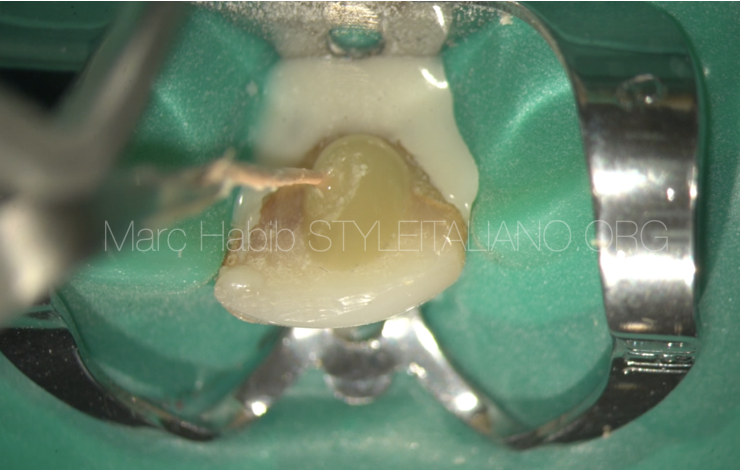
Cleaning and shaping were done with work length determination.
Root canal was still leaking some colored contaminated liquid.
Calcium hydroxide dressing was injected inside the shaped root and another appointment was scheduled in 10 days.

Fig. 4
Working length and Ca(OH)2 dressing

Fig. 5
After 10 days canal is dry due to the effect of calcium hydroxide high pH.
Master cone and obturation were completed and patient to be followed for the healing
Conclusions
According to the American Dental Association ADA, overfilling by more than 2mm past the radiological apex represents a technical error due to inadequate measurement of the working length, over-instrumentation or a lack of an apical stop.(1)This is widely accepted but what about sealer extrusion beyond 3-4mm of the apex?
Endodontic procedural errors are not the direct cause of treatment failure, it is rather the presence of pathogens in the poorly treated or untreated root canal system is the primary cause of periradicular pathosis. Procedural errors increases the risk of treatment failure, especially in teeth with necrotic pulps and periradicular lesions.
Overinstrumentation, in particular, may extrude infected material contained in the canals beyond the apex, inhibiting the healing process of the periapical tissue. Gutta percha cones which had been extruded past the apices and subsequently examined under a scanning electron microscope, have demonstrated the presence of a “biofilm” on the cones (2-3). The consequences of overfilling can, therefore, result in infective periapical periodontitis caused by the transport of bacteria beyond the apex and an incomplete cleansing of the root canal space. (4-5).
Different from this clinical case situation, cases of invasion of material beyond the apex with proximity to critical anatomical structures, such as the maxillary sinus or the mandibular canal, will produce undesirable complications and symptoms like sinusitis or neurological damage from neurotoxicity or mechanical compression. Even when using the latest and best techniques like warm vertical compaction or single cone with BC sealer for achieving the best results, the dentist is responsible for any possible risks connected with their treatment, as well as any errors made. It remains necessary, therefore, to establish the amount of overfilling allowed, in order to determine if an error has indeed occurred.
Bibliography
- Lin LM, Rosenberg PA, Lin J. Do procedural errors cause endodontic treatment failure? J Am Dent Assoc. 2005;136:187–93.
- Gutierrez JH, Brizuela C, Villota E. Human teeth with periapical pathosis after overstrumentation and overfilling of the root canals: a scanning electron microscopic study. Int Endod J. 1999;32:40–8.
- Pascon A, Leonardo MR, Safovi K, et al. Tissue reactions to endodontic materials: criteria, assessment and and observations. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1991;72:222–37.
- Bergenholtz G, Lekholm U, Milthon R, et al. Influence of apical overinstrumentation and overfilling on retreated root canals. J Endod. 1979;5:310–14.
- Costerton JW, Stewart PS, Gerenberg EP. Bacteria biofilms: a common cause of persistent infections. Science. 1999;284:1318–24.