Orthograde retrieval of a fractured instrument in a mandibular molar: loop technique as a predictable alternative in complex anatomy
23/04/2026
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Fractured instruments remain a major challenge in endodontic retreatment, particularly when located beyond canal curvature. This case describes the orthograde removal of a separated instrument in the mesiobuccal canal of a mandibular molar using a loop technique, after CBCT-based diagnosis and critical decision-making. Alternative approaches, including bypass, apical surgery, and extraction, were evaluated and discarded. After successful retrieval, the root canal system was disinfected and obturated using a three-dimensional approach. Two-year follow-up confirmed complete periapical healing. This case highlights the importance of case selection, magnification, and controlled dentin removal in achieving predictable outcomes.

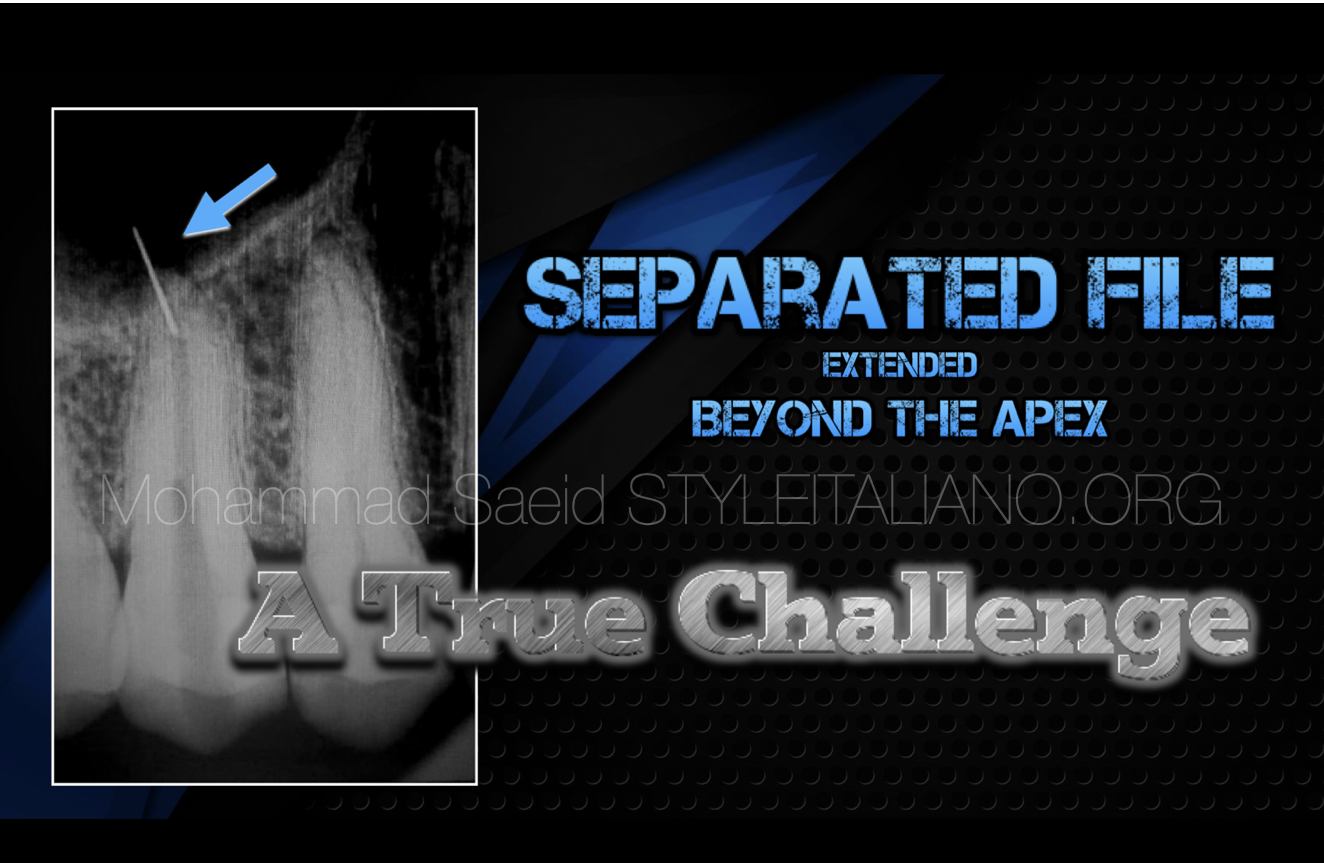
Fig. 1
37-year-old healthy patient referred for evaluation of tooth 37. Previous endodontic treatment complicated by a fractured instrument in the mesiobuccal canal.
Periapical radiograph revealed a retained fragment associated with apical pathology .
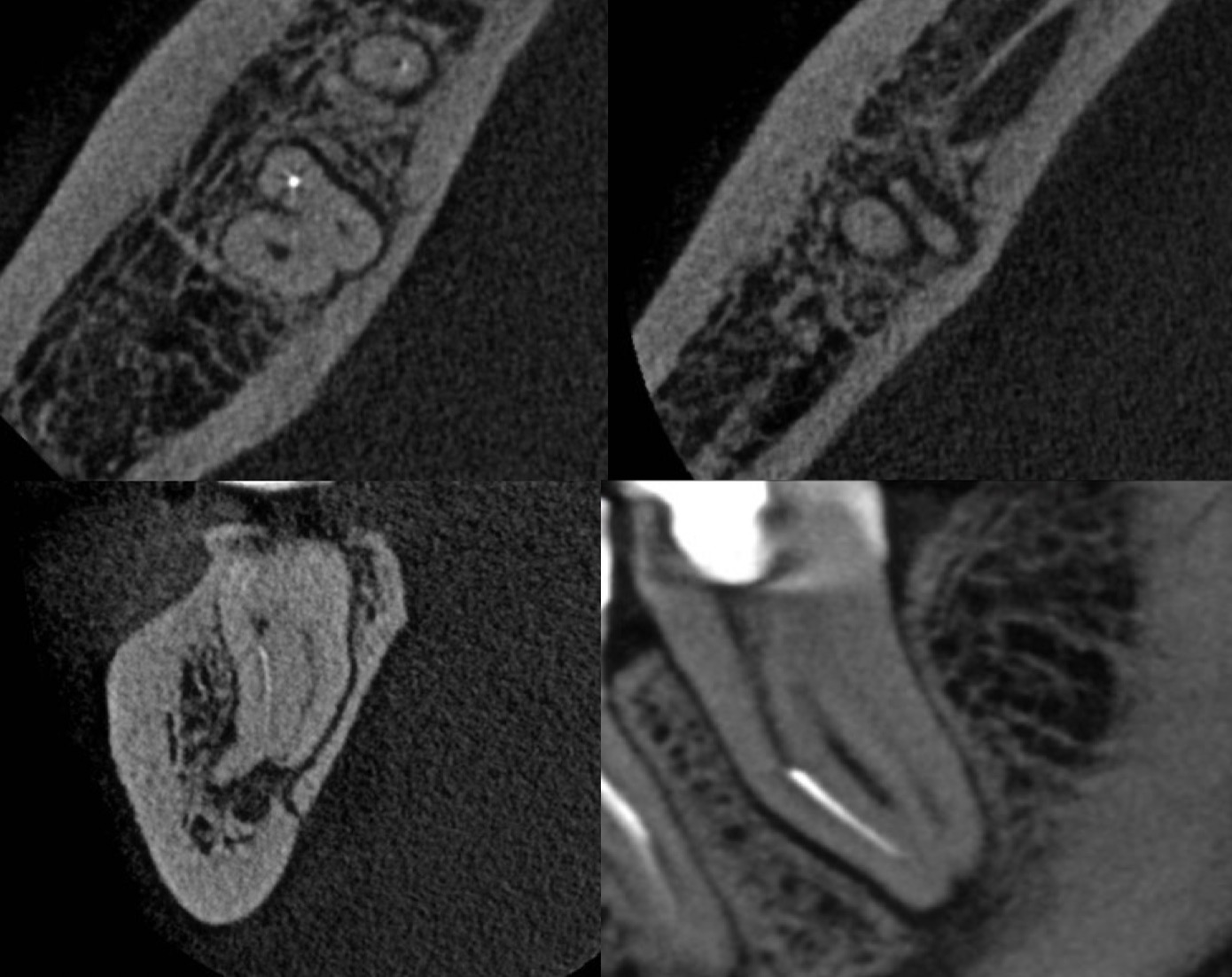
Fig. 2
CBCT Analysis
•Separated instrument beyond apical curvature (MB canal)
•Two independent mesial canals
•Thick buccal cortical plate → surgical approach limited
•Active periapical lesion close to inferior alveolar nerve
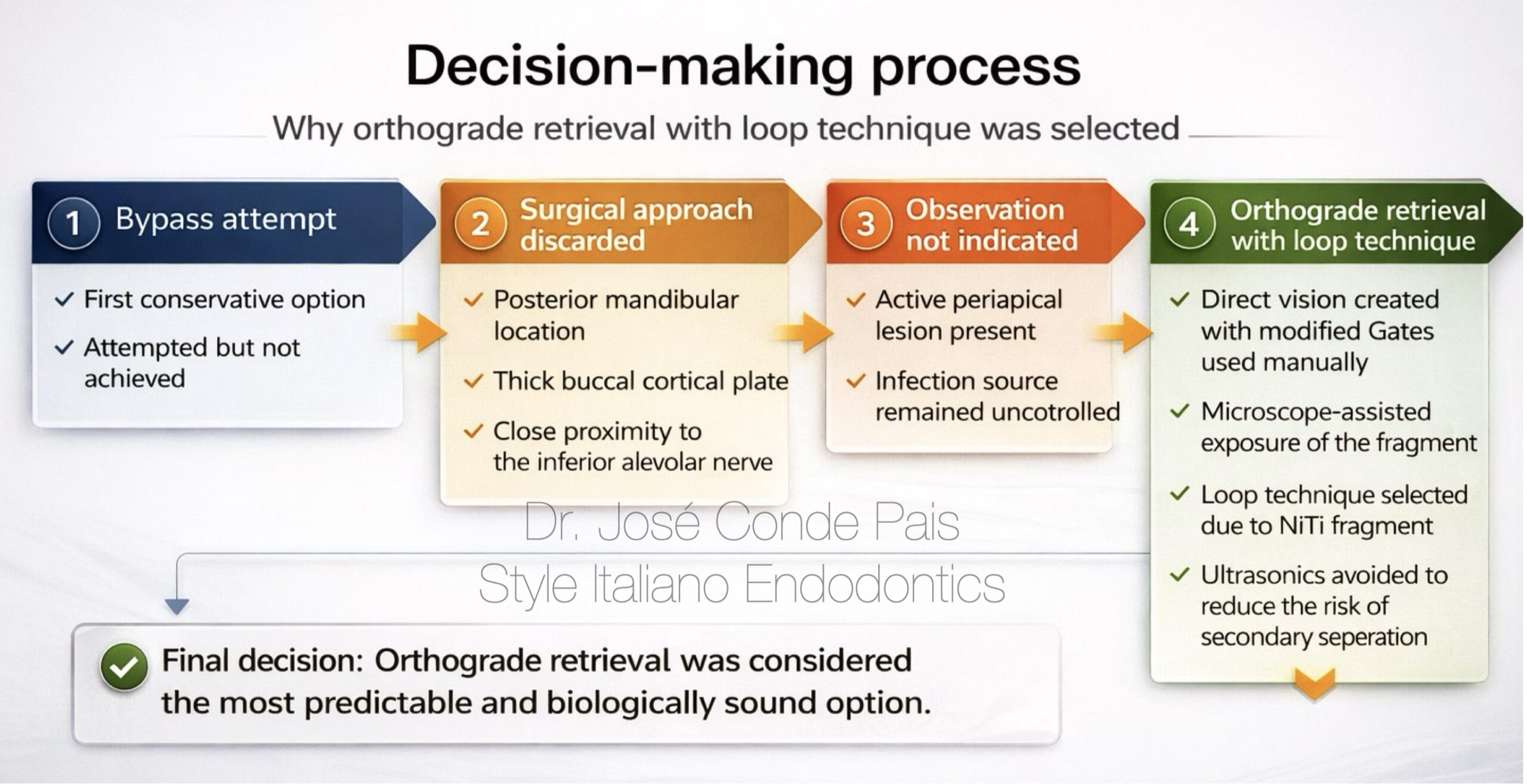
Fig. 3
Decision making

Fig. 4
Following local anesthesia and rubber dam isolation, a previously initiated access cavity was identified, sealed with a provisional IRM restoration.
After removal of the temporary material, the access cavity was re-evaluated, allowing proper visualization of the pulp chamber and underlying anatomy.
Instrument Retrieval
Step-by-Step
1. Access refinement
→ Access cavity redefined to achieve optimal straight-line access
2. Direct visualisation
→ Fragment exposed under magnification
→ Selective dentine removal using modified Gates (manual)
3. Staging platform creation
→ Stable working base created around the coronal portion of the fragment
4. Space preparation
→ Circumferential space developed to allow safe loop positioning
5. Loop engagement
→ Loop system carefully advanced and engaged around the fragment
6. Instrument retrieval
→ Gentle and controlled traction applied
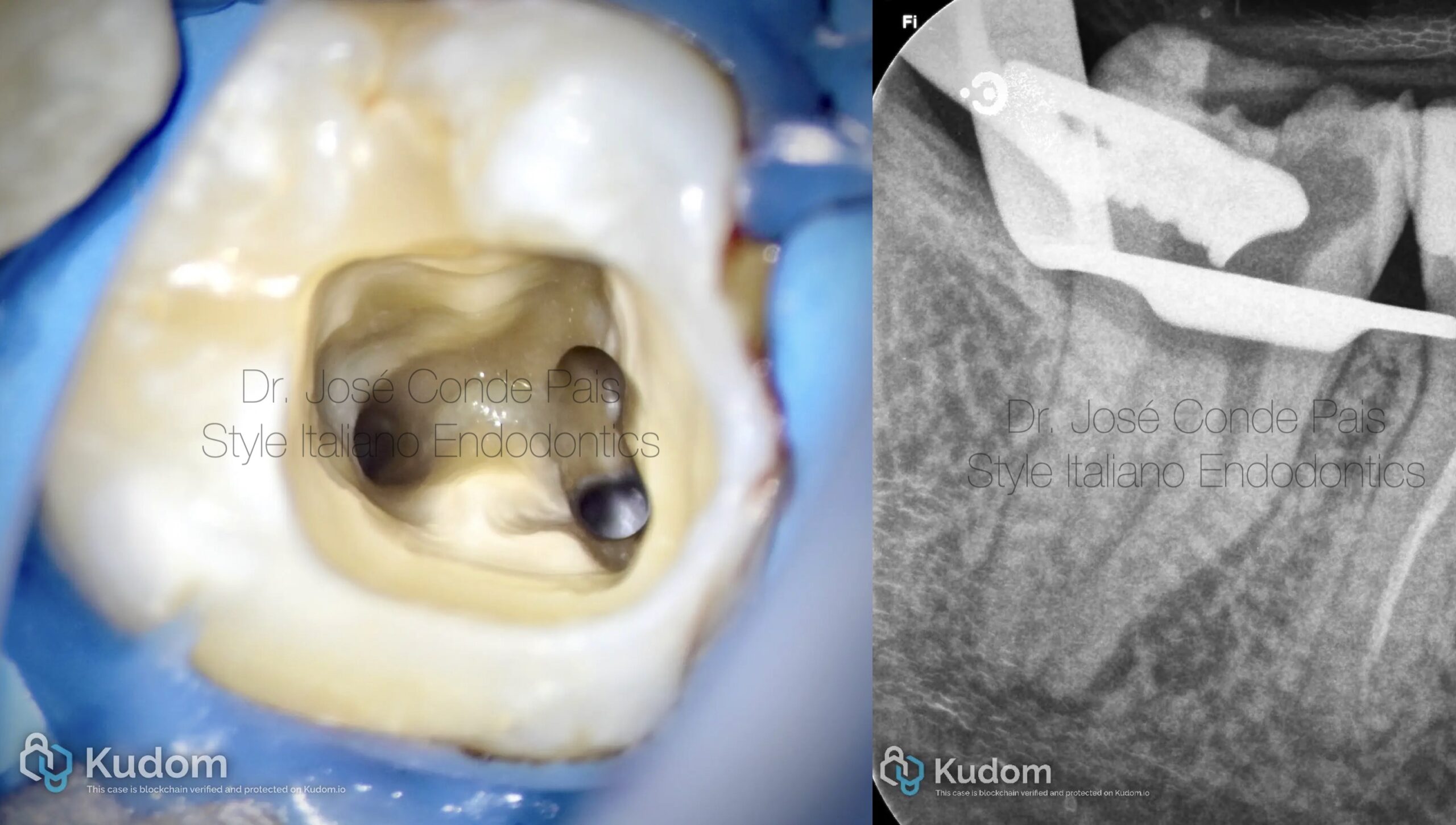
Fig. 5
Clinical aspect after successful instrument retrieval.
A clean chamber and controlled dentine removal can be observed, preserving the original canal anatomy and maintaining structural integrity.
Successful instrument retrieval is not only about removal, but about preservation.
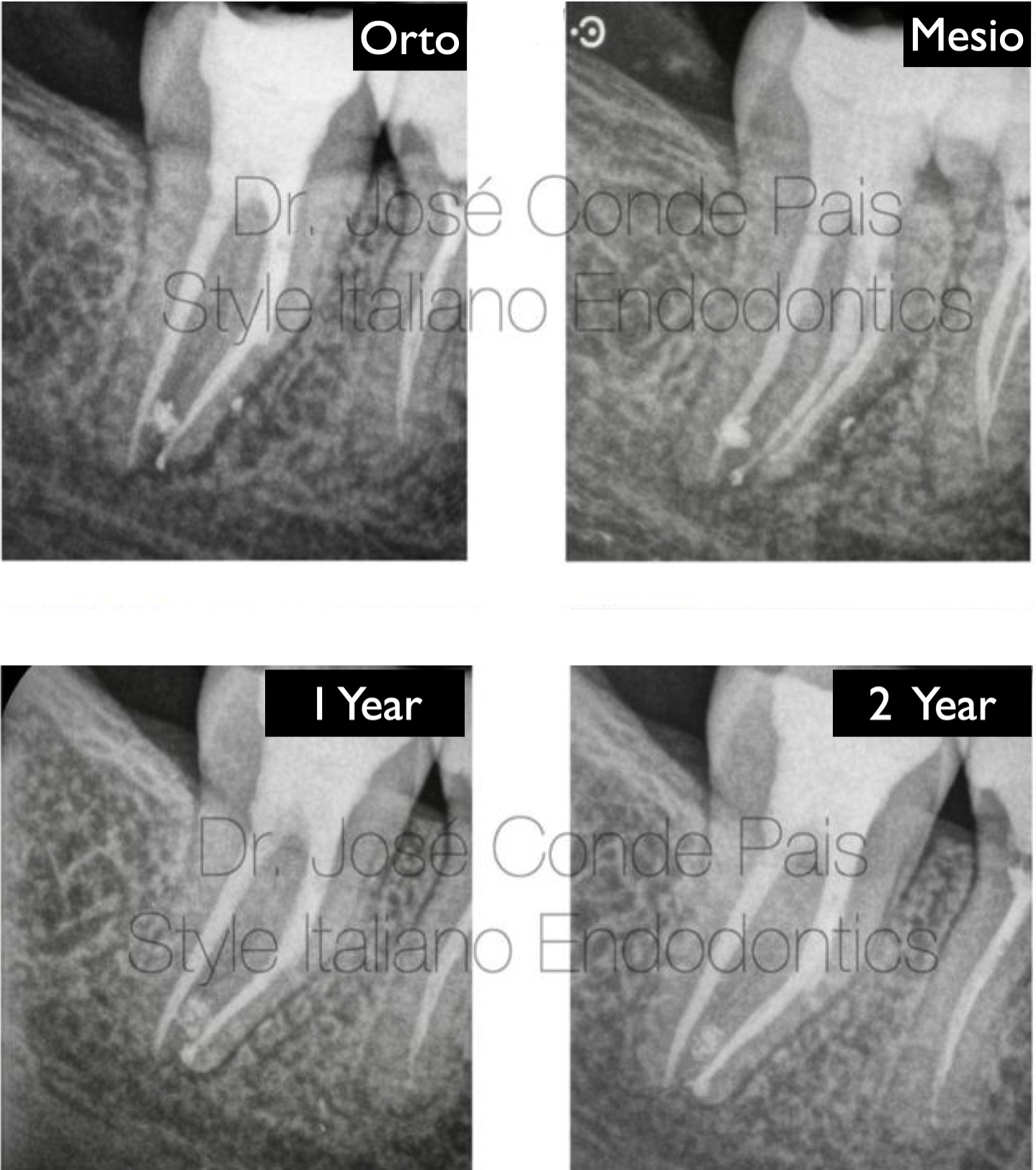
Fig. 6
Healing dynamics and 2 years outcome
Following successful orthograde retrieval, the case was completed with three-dimensional cleaning and obturation of the root canal system.
The immediate postoperative radiograph shows an adequate obturation, respecting the original anatomy.
An angled radiograph was also taken to better assess the complexity of the mesial root system and confirm the quality of the treatment.
At the 1-year follow-up, a clear reduction in the periapical radiolucency can be observed, indicating favourable healing.
At 2 years, complete radiographic resolution of the lesion is evident, confirming long-term success.

Fig. 7
Respecting the original anatomy is the foundation of long-term endodontic success.