Management of a separated instrument beyond the apex
16/09/2023
Mohammad Saeid
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Management of separated instruments usually involves on the following options:
- Bypass
- Retrieval
- Obturation to the level of separation
Choice of the management option depends on:
- Level of separation (coronal, middle or apical third)
- Location in relation to the root canal curvature
- The type of separated instrument; its length; the degree of canal curvature and the tooth type.
Concerning the removal of a separated instrument, a variety of techniques and systems have been developed. Ultrasonics, in combination with the operative microscope constitute the most effective and reliable tools for removing a separated endodontic instrument from a root canal.

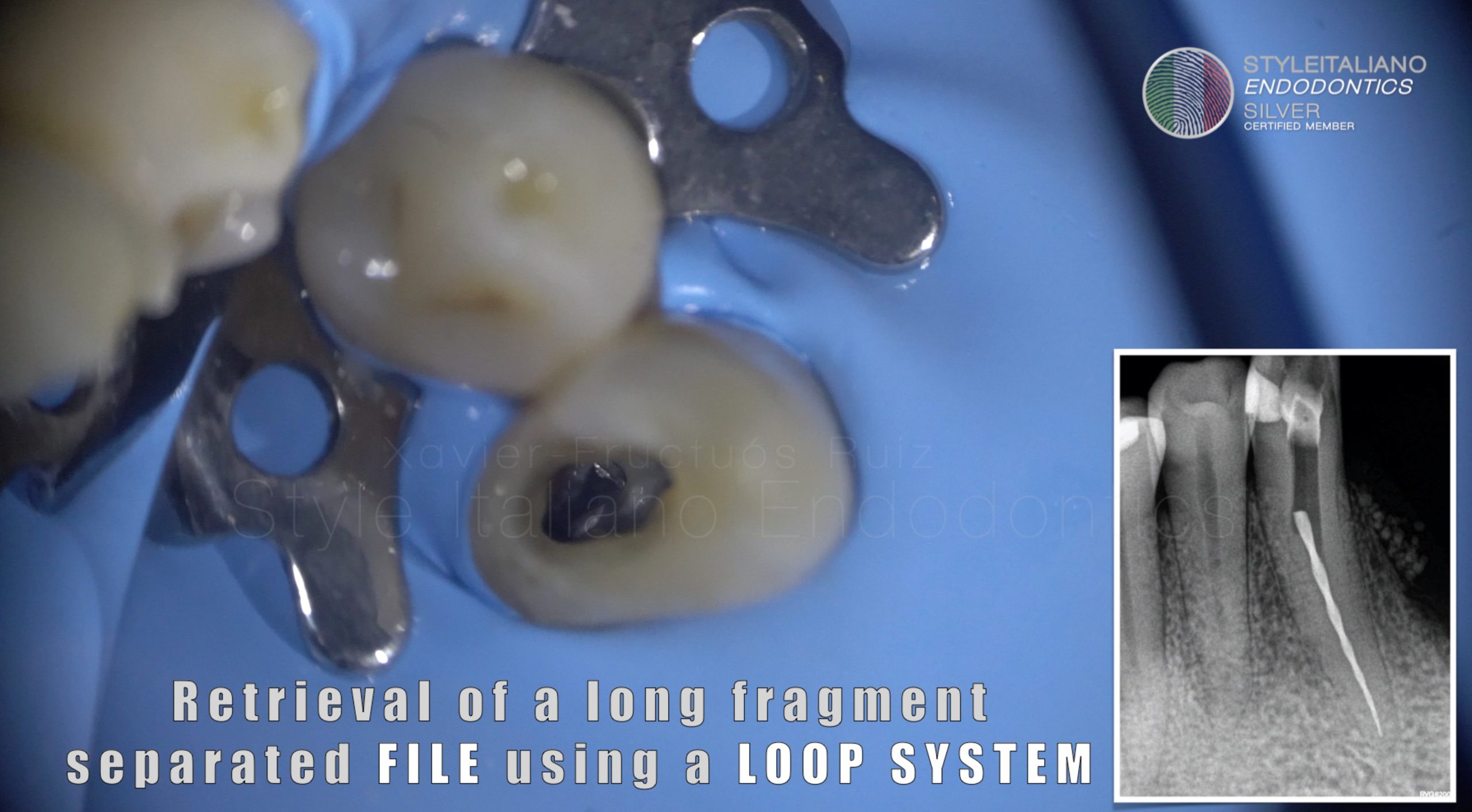
Fig. 1
A Breathtaking and adrenaline rising case was referred after several trials of bypassing ended up with pushing the file beyond the apex.
Usually the portion of the file beyond the apex is not engaged and almost loose and in this case the less taper of the file was the cause of its extension beyond the apex.
Analysis of radiographic image shows the instrument is in a curved position.
Usually the proper technique of retrieval in such cases is grasping as using ultrasonic here is kind of risky and may push the file more apically or it may even cause its extrusion out of the tooth but due to the very deep location of the file I was not able to insert a grasping tool due to lack of space and the laying of coronal portion of the file on the outer wall and being the file not engaged the process went easier.
So I started to trough a little in the outer wall with an extreme caution not to touch the file.
All focus was to cut from dentine on the outer wall to create space between the file and the canal wall.
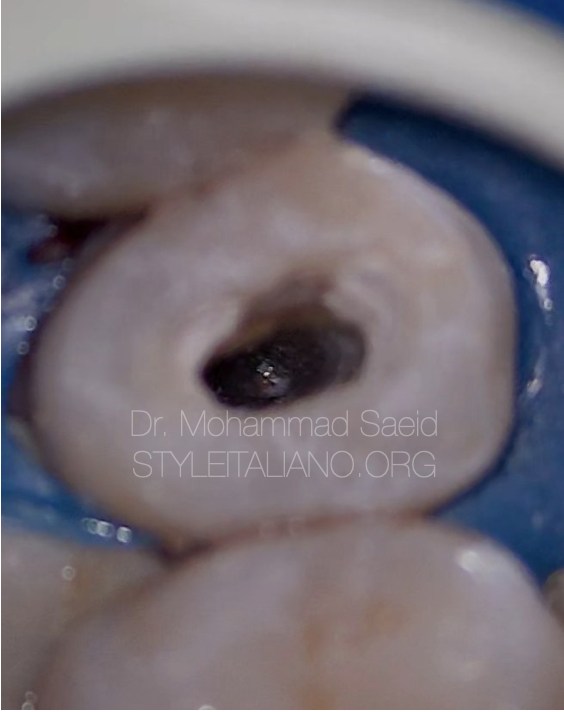
Fig. 2
With the help of ultrasonics the file now in an upright position and not engaged.
Then the file was retrieved with the help of an ultrasonic tip used at the lowest power

Fig. 3
The apical one third of the canal was obturated with MTA and the tooth was restored with composite then sent back to the referring doctor.
Conclusions
Separated instruments during shaping root canals is a real nightmare and frustration so we should take all the precautions to avoid it and know how to deal with it if happens.
Bibliography
McGuigan MB, Louca C, Duncan HF. Endodontic instrument fracture: causes and prevention.
Rzhanov EA, Belyaeva TS. Design features of rotary root canal instruments.
Walia HM, Brantley WA, Gerstein H. An initial investigation of the bending and torsional properties of Nitinol root canal files.