Retrieval of a long fragment separated file using a loop system
13/04/2023
Xavier-Fructuós Ruiz
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
The separation of a file during a root canal treatment is a complication with an incidence ranging from 0,4-5% of cases. The evidence has shown that the outcome of root canal treatment lowers if the broken file doesn’t allow a proper disinfection and obturation of the root canal space or if the file breaks at the beginning of the treatment.
Different treatment options are available when facing teeth with separated instruments such as referring the patient to a more skillful specialist, bypassing the instrument, attempt the removing of the fragment, leaving the fragment in situ or considering a surgical approach.
The success of removing a file will depend on several factors such as location of the separated instrument, the root canal curvature, the canal diameter, the endodontist skills, and the length of the file.
In cases where the separated fragment is longer than 4.5mm, the use of ultrasonic tips won’t be enough to remove the file in a predictable way. Therefore, the use of other devices like loop systems have been recently recommended.
The present case shows a file removal procedure of a long separated fragment in a mandibular canine using ultrasonic tips and a loop system.

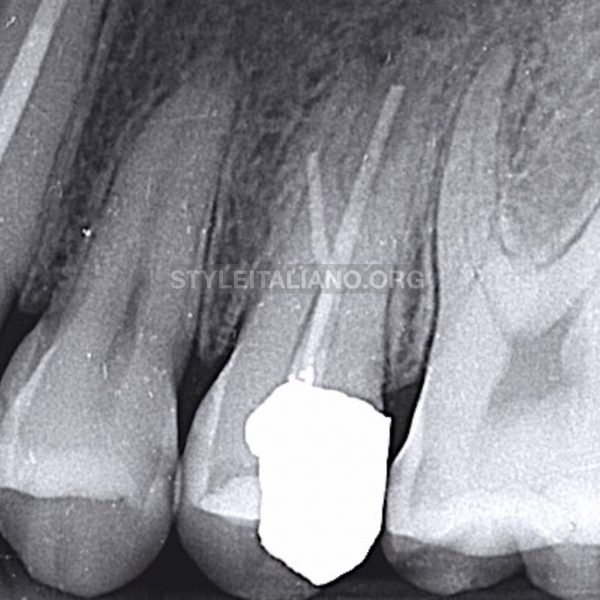
Fig. 1
A 45-year-old male was referred from another clinic because the previous dentist separated a file in a mandibular right canine at the beginning of a treatment (tooth 4.3).
The clinical examination showed that tooth 4.3 had a temporary restoration and was painful upon percussion test.
The radiographic examination showed a long separated file extending from the coronal to the apical third. Furthermore, the radiograph showed a considerably dentin removal surrounding the instrument which meant that there had been a previous attempt to remove the fragment. Even though the tooth responded painfully after percussion test, there was no radiolucency around the periapical tissues.
The final diagnosis was previously initiated therapy with symptomatic apical periodontitis.
The established treatment plan considering the length of the file was to try to remove it using ultrasonic tips, although due to the length of the separated instrument a loop system was chosen.
After rubber dam isolation, canal inspection showed the head of the file which was clearly visible. An endodontic explorer was used to assess the broken instrument mobility. The first attempt was to use an ET25 ultrasonic tip and perform a direct vibration to try to dislodge the file. Due to the length of the fragment, it was decided to use a loop system (BTRPen) with a 0.5mm loop wire.
The full broken file removal procedure was performed in 17 minutes.
After that, patency was achieved and working length was determined. A manual glide-path was performed with a 10k,15k, 20k manual file (31mm) and the root canal was instrumented with a Reciproc 25.08 file.
Apical gauging was then performed and the canal was instrumented up to a 40.04 Profile file. Copious irrigation with sodium hypochlorite 4.25% was done and the canal was then dried with paper points.
Thermocompaction with Guttaconsendor was the obturation technique used with a 6% tapered gutta-percha and a resin-based sealer.

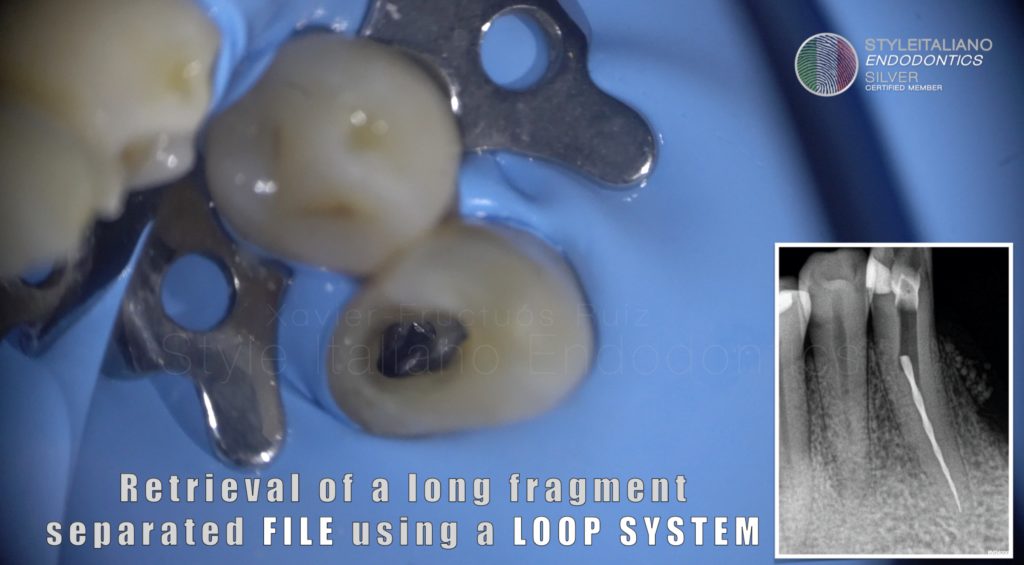
Fig. 2
Loop system picture with the long file fragment removed

Fig. 3
Radiograph after broken file removal
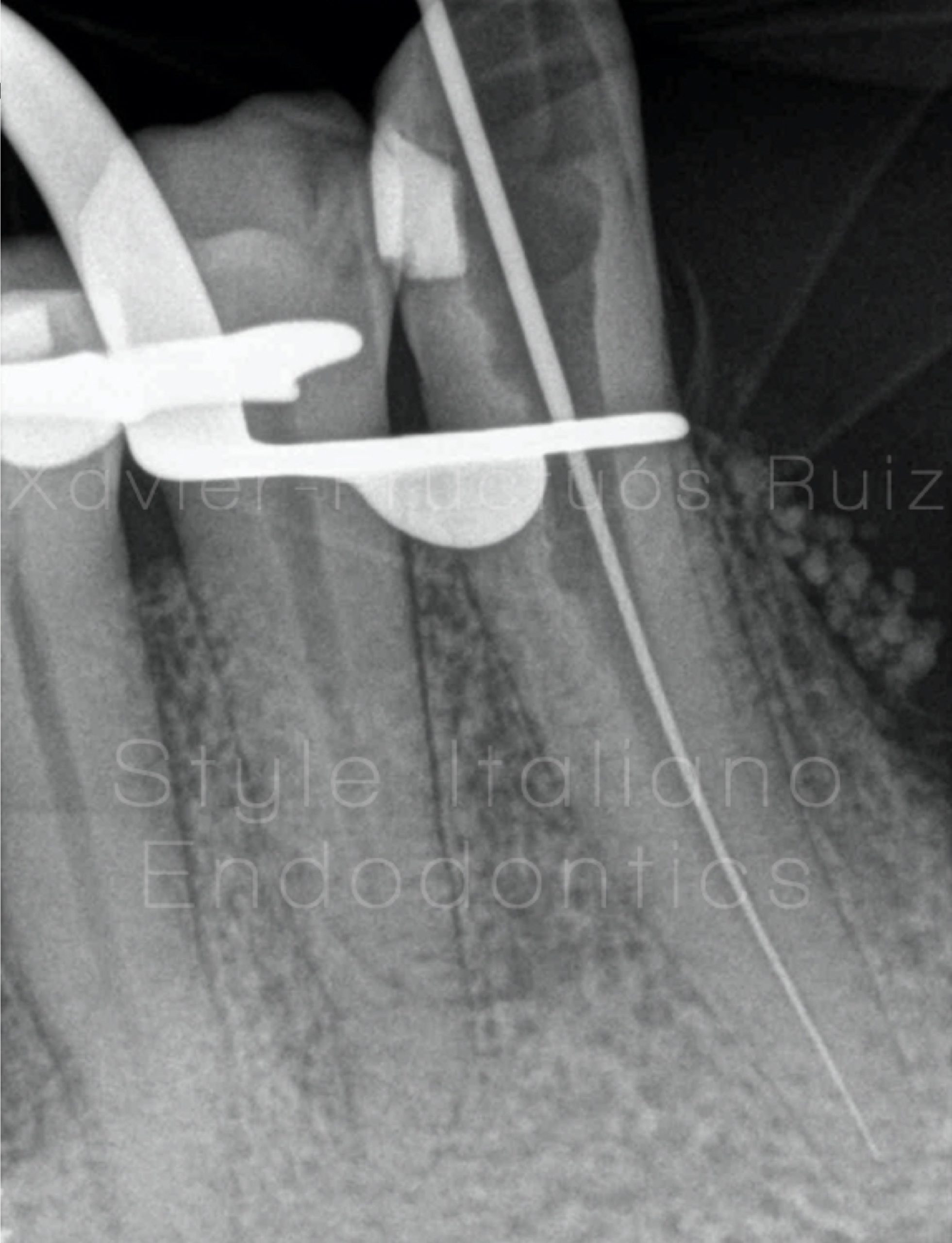
Fig. 4
Working Length Radiograph
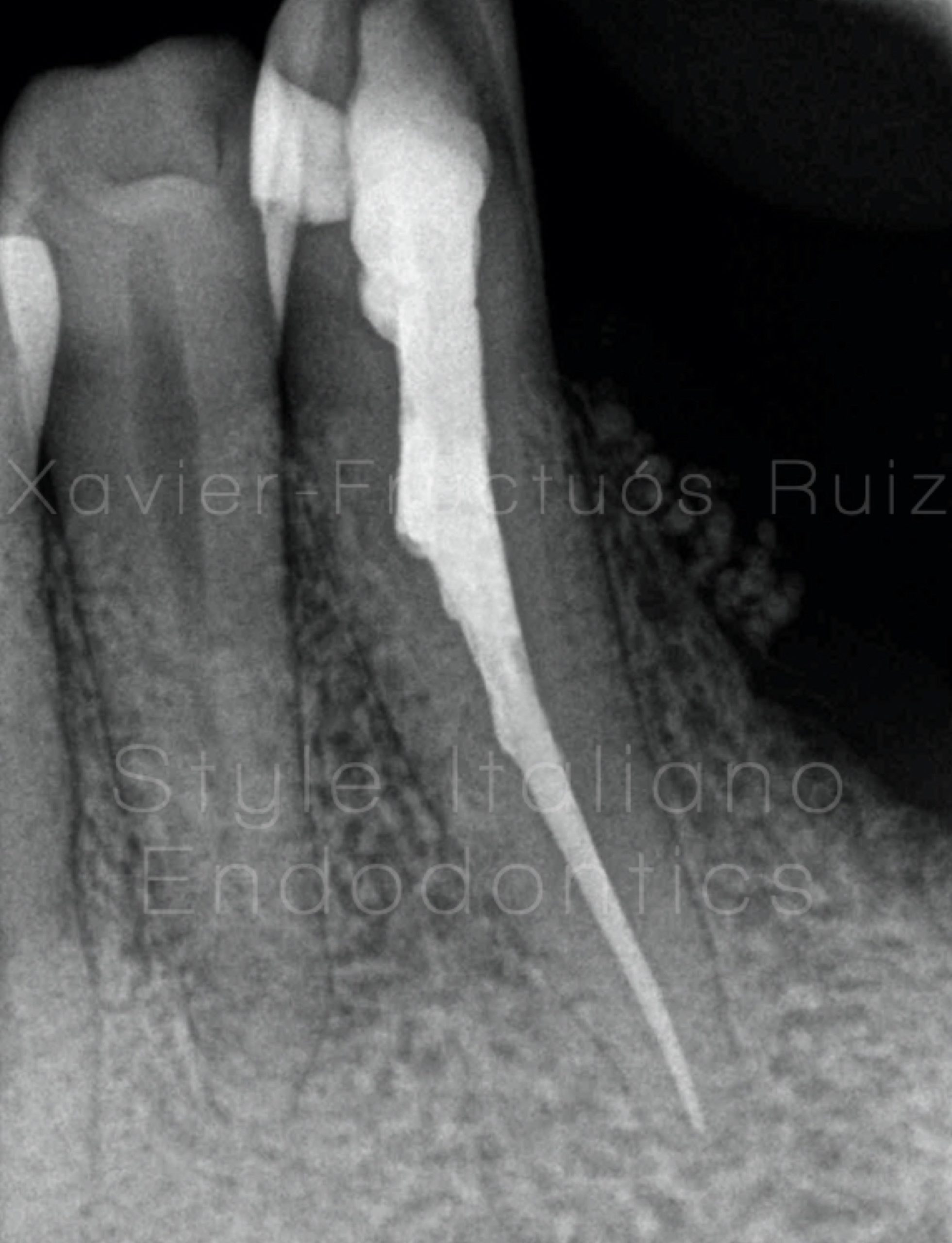
Fig. 5
Post-operative radiograph

Fig. 6
Photographic Sequence
1- File inspection.
2- Loop placement.
3-File retrieved.
4- Root canal obturation.
Conclusions
Loop systems can be used in a more conservative and predictable way for broken file removal minimizing dentin damage.
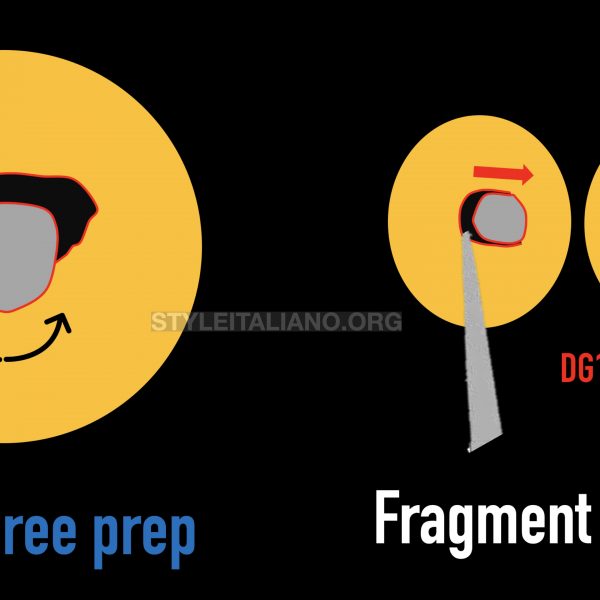
The most important factors to succeed when attempting to remove these instruments are: 1) having clear vision of the head of the file and 2) having enough space around the file to place the loop. In cases where there is not enough space surrounding the file, the use of ultrasonic tips is mandatory to create a platform.
Bibliography
Panitvisai P, Parunnit P, Sathorn C, Messer HH. Impact of a retained instrument on treatment outcome: a systematic review and meta-analysis. J Endod 2010;36:775–80.
Terauchi Y, O’Leary L, Kikuchi I, et al. Evaluation of the efficiency of a new file removal system in comparison with two conventional systems. J Endod 2007;33:585–8.
Madarati AA, Hunter MJ, Dummer PM. Management of intracanal separated instruments. J Endod 2013;39:569–81.
Terauchi Y, Sexton C, Bakland LK, Bogen G. Factors Affecting the Removal Time of Separated Instruments. J Endod. 2021;47:1245-52.