One canal, two broken files
01/07/2024
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
The position and anatomy of upper molars can make root canal treatment challenging, and instrument separation is common.
In the presented case, tooth 1.6 had an abscess, and an attempt at root canal treatment was made. Unfortunately, the previous dentist encountered difficulties and broke a paste carrier approximately 4 mm beyond the apex. In the attempt to remove it, another instrument separated in the canal. Additionally, there was a missed Mb2 canal and a large lateral canal in the palatal root.
The main challenge with instruments broken beyond the apex is that it is quite difficult to remove them with either ultrasonic tips or file retrieval systems, often leaving surgery as the only option. Ultrasonic tips are particularly unhelpful with paste carriers due to the flexibility of the instrument.
The distal canal was approached by enlarging the coronal portion and retrieving the smaller separated instrument. Unfortunately, this was not enough to allow the removal of the paste carrier with a "lazo system," as the spirals were stuck beyond the apex. Therefore, manual shaping of the apical portion was carried out using stainless steel files size 6, 8, and 10 before twisting the paste carrier with the lazo system.
The entire root canal system was then shaped, cleaned, and obturated with gutta-percha and hydraulic cement.
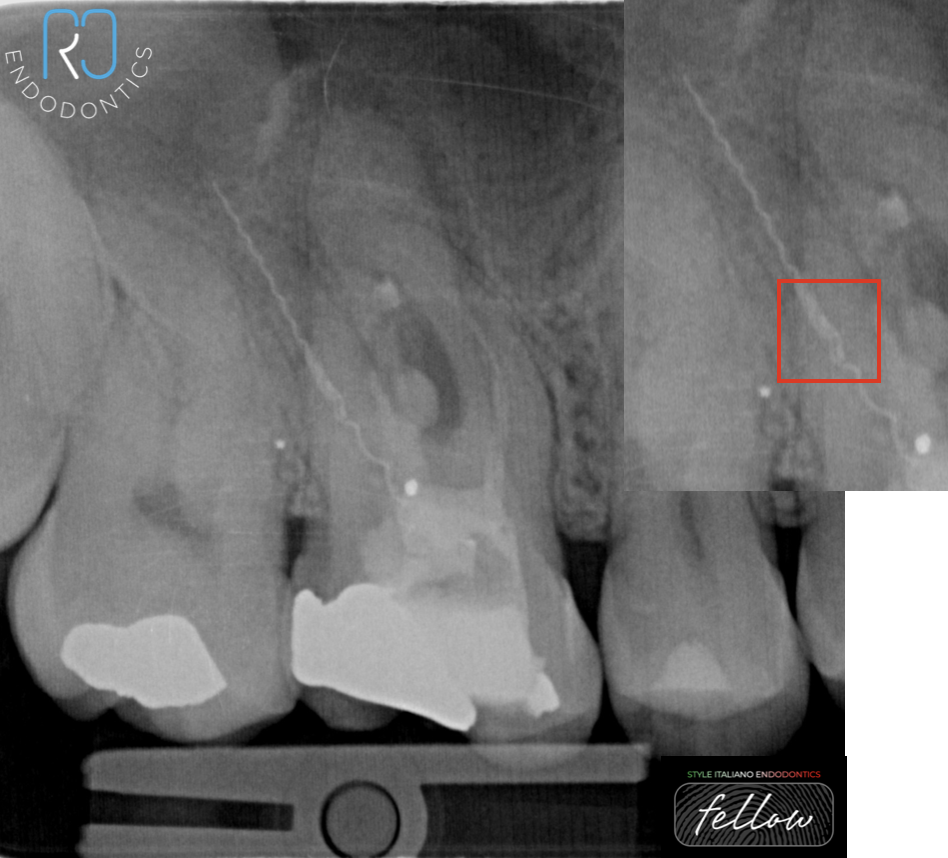
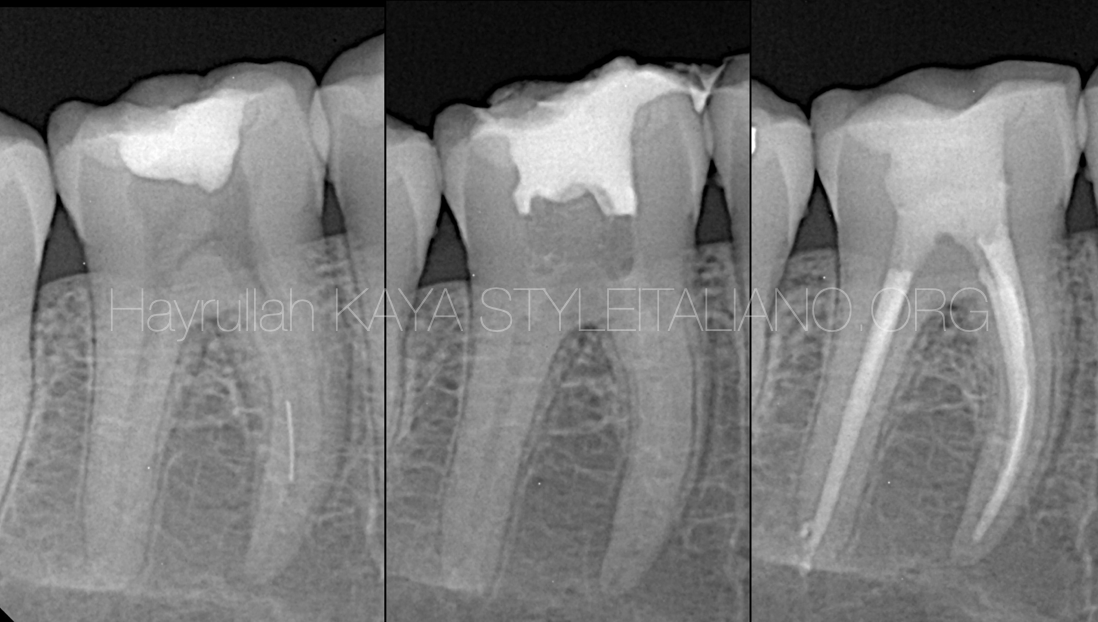
Fig. 1
Tooth 16 was treated for apical pathosis.
During the treatment, a paste carrier separated approximately 4 mm beyond the apex of the distal root.
Another small instrument was then broken in the middle third
of the canal.
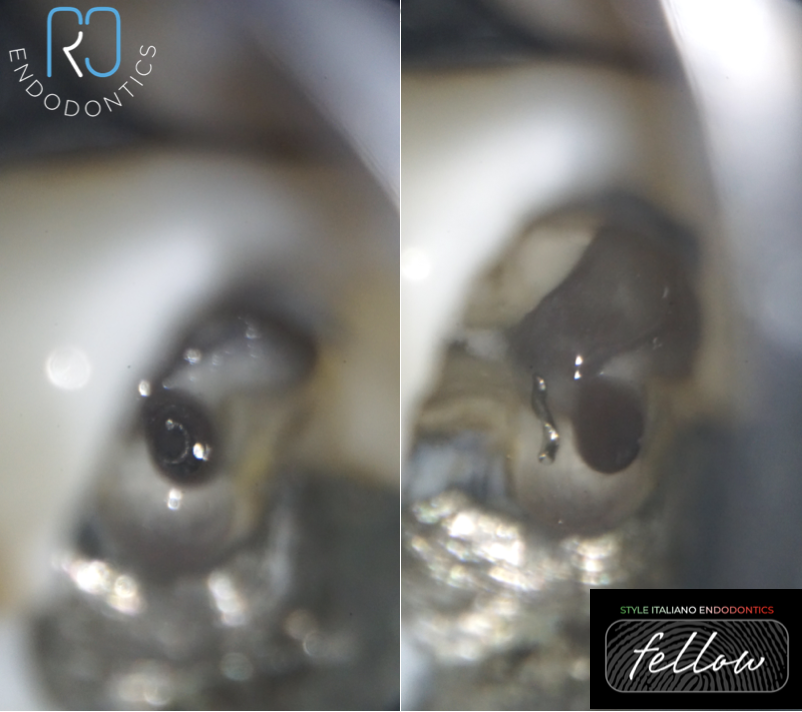
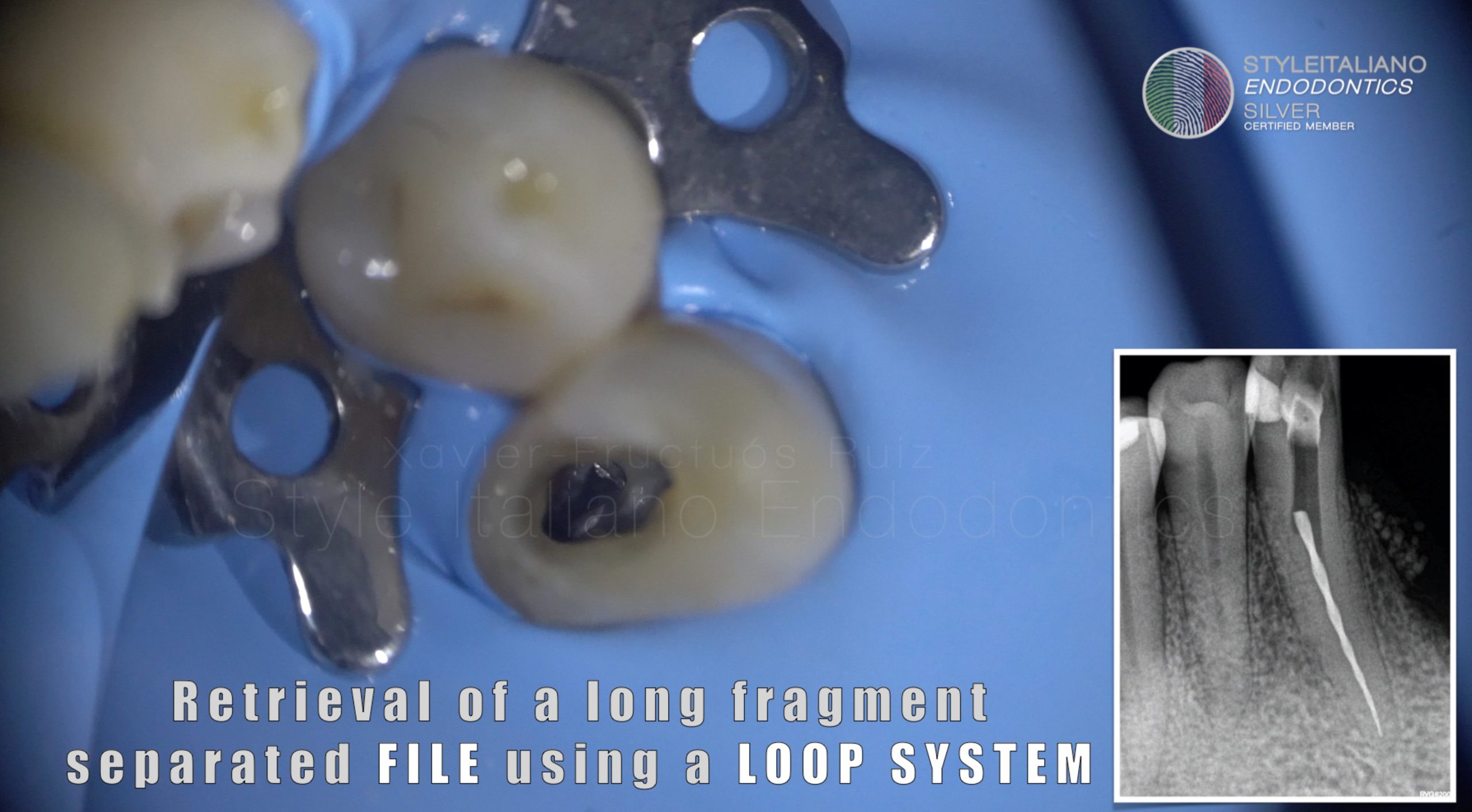
Fig. 2
The tip of an hand file was removed with ultrasonic tips, manual files and microscopic probes.
On the left image both the file and the paste carrier are visible.
On the right image the tip of the file was removed, however in order to take it out from the canal the coronal portion of the paste carrier had to be cut, making more difficult its engagement to a lazo system.

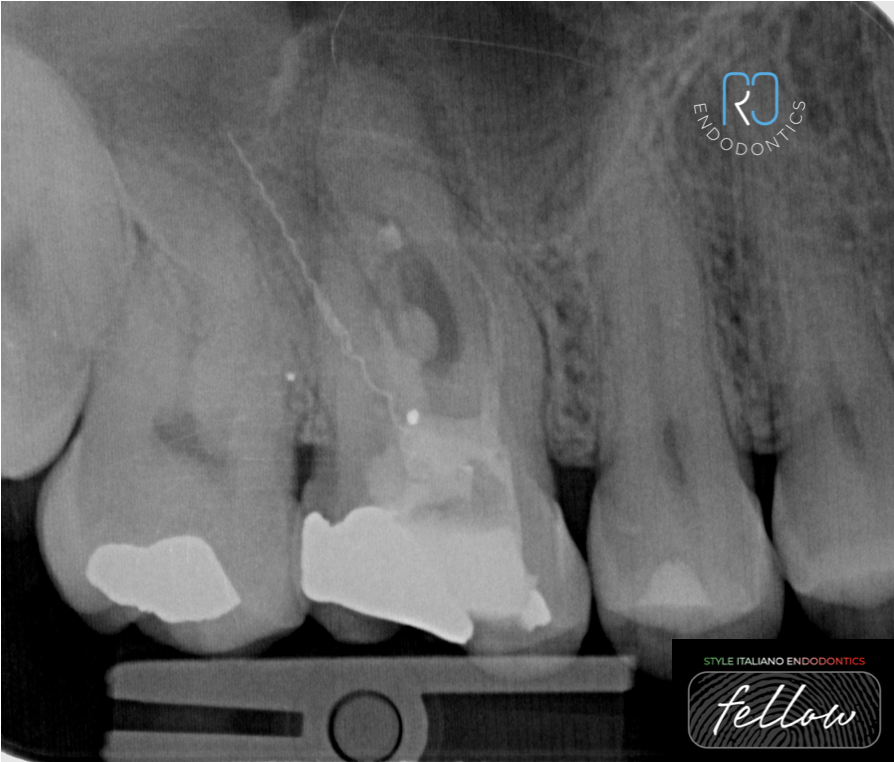
Fig. 3
Xray after 1st instrument removal

Fig. 4
Paste carrier removed after enlarging manually the apex with K files number 6, 8 and 10 and then twisting the instrument using a lazo system.

Fig. 5
The missing Mb2 was found and all the canals were shaped and cleaned with NaOCL and EDTA activated.

Fig. 6
The tooth was then sealed with HCSC and gutta-percha, palatal root shows a large puff of material in the middle third. That extrusion is due to a large lateral canal.
The tooth was temporised and the patient was then seen by a restorative dentist for permanent restoration.

Fig. 7
The tooth was initially restored with a core filling and subsequently with an overlay.
The patient reported complete absence of symptomatology and the post cementation X-ray shows the progression of the healing process

Fig. 8
About the author;
Roberto Careddu
I was born in Sardinia (Italy) and I graduated with Honors from the University of Cagliari (Italy). My endodontic journey started with a Master in Clinical Endodontics and continued with courses and univeristy programs in different countries. I recently completed my PhD at Trinity College of Dublin.
I live in Dublin, where I work as Endodontist in private practice and I am Clinical Supervisor in the Dublin Dental University Hospital.
I have authored scientific articles and I serve as an international conference speaker.
I am Member of the Faculty of Dental Surgery of the Royal College of Surgeons of Ireland, Member of the Committee and President Elect of the Irish Endodontic Society (IES) and the Irish representing for the European Society of Endodontology (ESE).
Conclusions
Paste carriers should be carefully used after estimating the working length in order to avoid their extrusion over the apical portion.
When removing paste carriers it is useful to have at hand instrument removal kits such as Endocowboy, BTR pen or similar as the ultrasonic tips may not work.
Bibliography
Madarati AA, Hunter MJ, Dummer PM. Management of intracanal separated instruments. J Endod. 2013 May;39(5):569-81. doi: 10.1016/j.joen.2012.12.033. Epub 2013 Mar 15. PMID: 23611371.
Bhuva B, Ikram O. Complications in Endodontics. Prim Dent J. 2020 Dec;9(4):52-58. doi: 10.1177/2050168420963306. PMID: 33225854.
Terauchi Y, Sexton C, Bakland LK, Bogen G. Factors Affecting the Removal Time of Separated Instruments. J Endod. 2021 Aug;47(8):1245-1252. doi: 10.1016/j.joen.2021.05.003. Epub 2021 May 14. PMID: 34000326.