Triple trouble
23/12/2023
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
In order to be able to perform a successful and predictable root canal treatment, the clinician knowledge regarding the root canal systems, anatomy variations and deal with obstacles to perform good shaping, cleaning and Obturation serves a strategic role.
Pulp stones are defined as foci of calcifications that form within the pulp chamber, more frequently in the coronal pulp cavity and sometimes in radicular pulp space. Classification of the dental pulp stones are either free where it lies on the pulp, adherent which it adheres to the walls of the pulp chamber, lastly it may be be embedded, in that case stones are embedded in the dentine.
This article will show the management of a case with adherent pulp stone.
Complex anatomy can lead to series of mishaps as perforation, ledges or separated instruments. Good knowledge and data evaluation would be crucial for the treatment outcome.
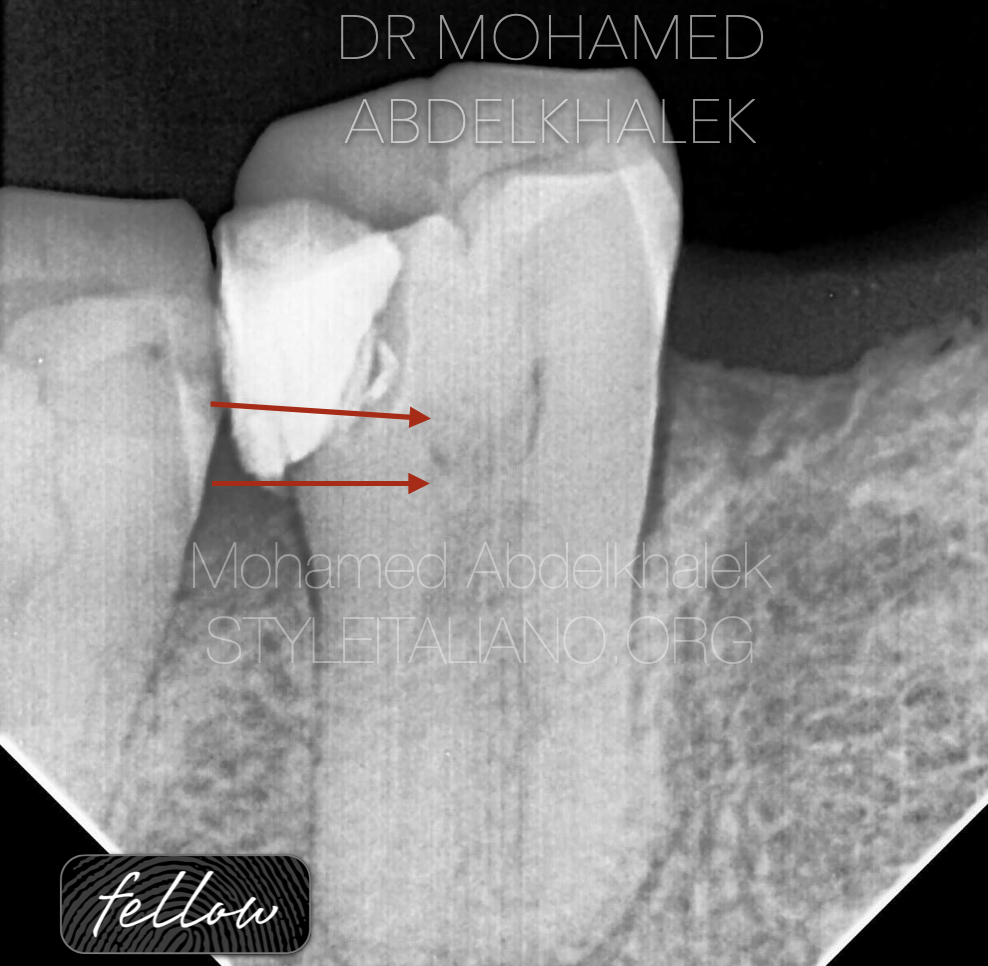
Fig. 1
In this article we will review a case showing the management of complex anatomy with pulp stone and unfortunately a separated instrument related to the mesio-lingual canal.
On clinical examination, it was observed that tooth number 47, which had history of restoration was symptomatic. The tooth was tender to percussion.
Pre-operative Radiographic evaluation revealed adherent pulp stone as shown in fig.2
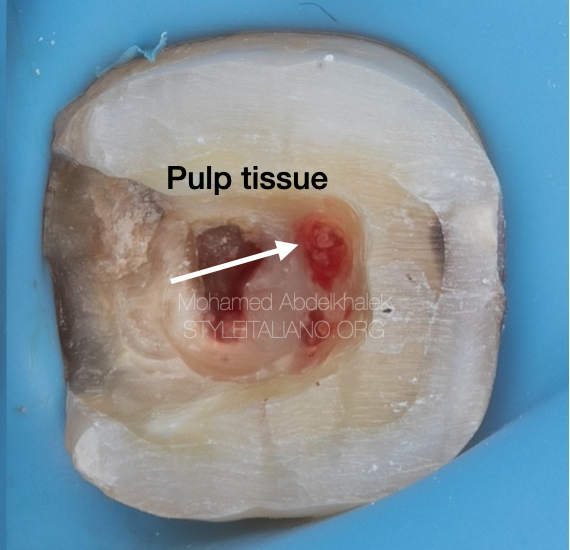
Fig. 2
The first step was to apply rubber dam for good isolation and better visualization for a successful root canal treatment, access cavity was done and the pulp stone (denticle) was exposed.
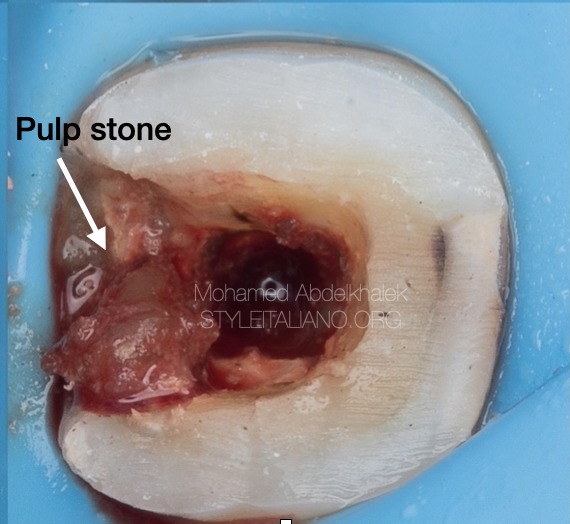
Fig. 3
Adherent pulp stone management was done using ultrasonic never with burs all around the walls then pulled as one part.

Fig. 4
Unfortunately, while shaping, one instrument probably separated due to torsional fatigue in the mesio-lingual canal.
Management of the separated instrument starts with good data analysis for predictable file retrieval with minimum dentinal loss.
The separated instrument was size 25 taper 4 with length not more than 4 mm in the apical third.
Master-file radio-graph shows adequate length to both mesio-buccal canal and distal system.
Briefly, the management of separated instrument involve the usage of thin ultrasonic for minimal dentin removal with low to medium power to avoid secondary fracture of the file. Irrigation with the help of the ultrasonics also creates acoustic waves lead the file to go towards the orifice with successful retrieval
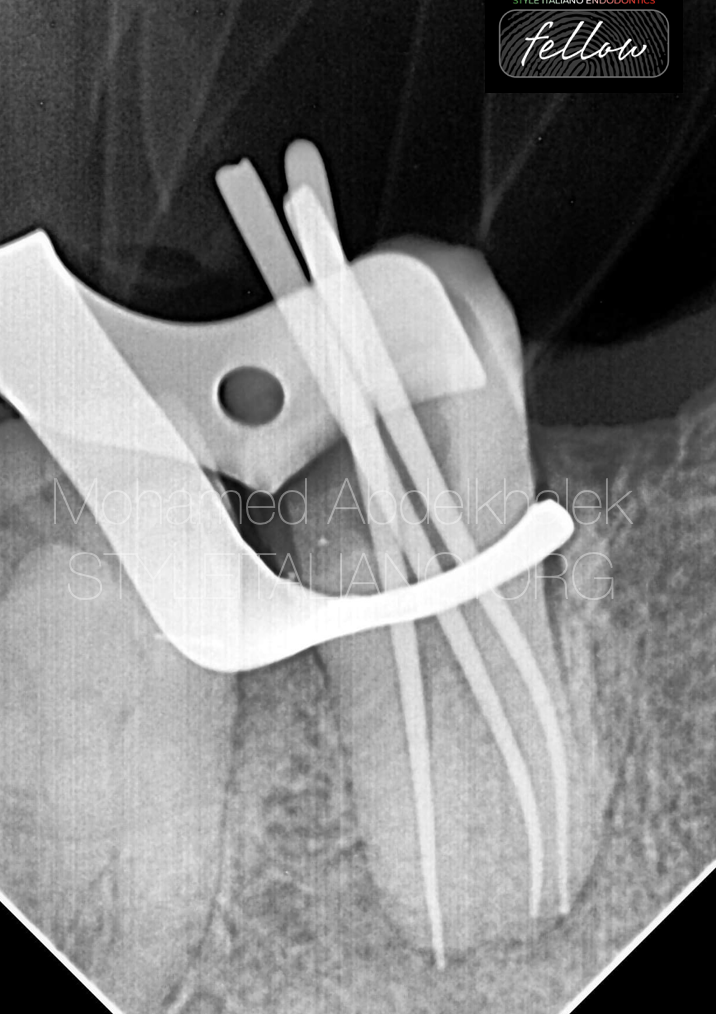
Fig. 5
The master-cone radiograph shows that in the mesial system the guttapercha is well fitted to the full working length. In the distal system the gutta-percha point is overextended by 1 mm beyond the apex, so it needs to be adjusted.
Obturation was done using resin sealer by WVC ( warm vertical compaction)

Fig. 6
The post-operative radiograph shows adequate obturation to the full working length in both mesial and distal systems.
Coronal seal was done in the same visit as it serves as a strategic role for a long-term successful root canal treatment, ready for final post endodontics restoration.

Fig. 7
About the author:
Dr Mohamed Abdelkhalek
I'm a dentist was born and raised in Alexandri, I'm really passionate about endodontics and digital dentistry.
Proudly I'm providing elite services to my patient, also have been sharing knowledge with other colleagues inwebinars and local conference.
EDUCATION
2012- 2017
University of Pharos
WORK EXPERIENCE
Dental derma dreams
Full time conservative dentist related to microscopic and digital dentistry
• Advanced endodontic in Mazen
dental clinic
Microscopic dentist
Digital dentistry
ADA certificate in endodontics
Conclusions
Endodontic Treatments are strategy based treatments rather than just procedural steps.
The clinician must integrate knowledge about tooth complex anatomy and how to get over obstacles with suitable armamentarium for a successful long term root canal treatment.
Bibliography
1.Ten Cate’s Oral Histology (Eighth Edition), 2013
2.Brad W. Neville DDS, Angela C. Chi DMD- Color atlas of oral and maxillofacial diseases, 2019.
3.Goga R, Chandler NP, Oginni AO. Pulp stones: A review. Int Endod J. 2 0 0 8 ; 41( 6 ) : 4 5 7– 4 6 8 .
4.Schaffner, M.; Stich, H.; Lussi, A. Denticles: Dental pulp calculi. Swiss Dent. J. 2014, 124, 416–417
5.Jannati, R.; Afshari, M.; Moosazadeh, M.; Allahgholipour, S.Z.; Eidy, M.; Hajihoseini, M. Prevalence of pulp stones: A systematic review and meta-analysis. J. Evid. Based Med. 2019, 12, 133–139
6.Kronfeld R, Boyle PE. Histopathology of the Teeth and Their Surround- ing Structures. 4th ed. London, UK: Henry Kimpton; 1955.
7. Goga R, Chandler NP, Oginni AO. Pulp stones: A review. Int Endod J. 2 0 0 8 ; 41( 6 ) : 4 5 7– 4 6 8 .
8.Plotino, Gianluca & Pameijer, Cornelis & Grande, Nicola & Francesco, Somma. (2007). Ultrasonics in Endodontics: A Review of the Literature. Journal of endodontics. 33. 81-95. 10.1016/j.joen.2006.10.008.