Middle mesial canal – a case series
09/08/2024
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Middle mesial canal (MMC) is an additional canal found in mandibular first molars.
The knowledge of its presence and its detection, negotiation, disinfection and sealing plays paramount importance in the overall endodontic success.

Fig. 1
Case 1: Radix paramolaris and middle mesial canal (MMC)
18 year old female patient was referred to the practice for severe and spontaneous pain wrt 36.
On examination, 36 had deep caries and the tooth responded acutely to thermal test.
IOPA xray revealed large carious defect encroaching the pulp with no significant changes in periapical region.
Diagnosis of symptomatic irreversible pulpitis was made.

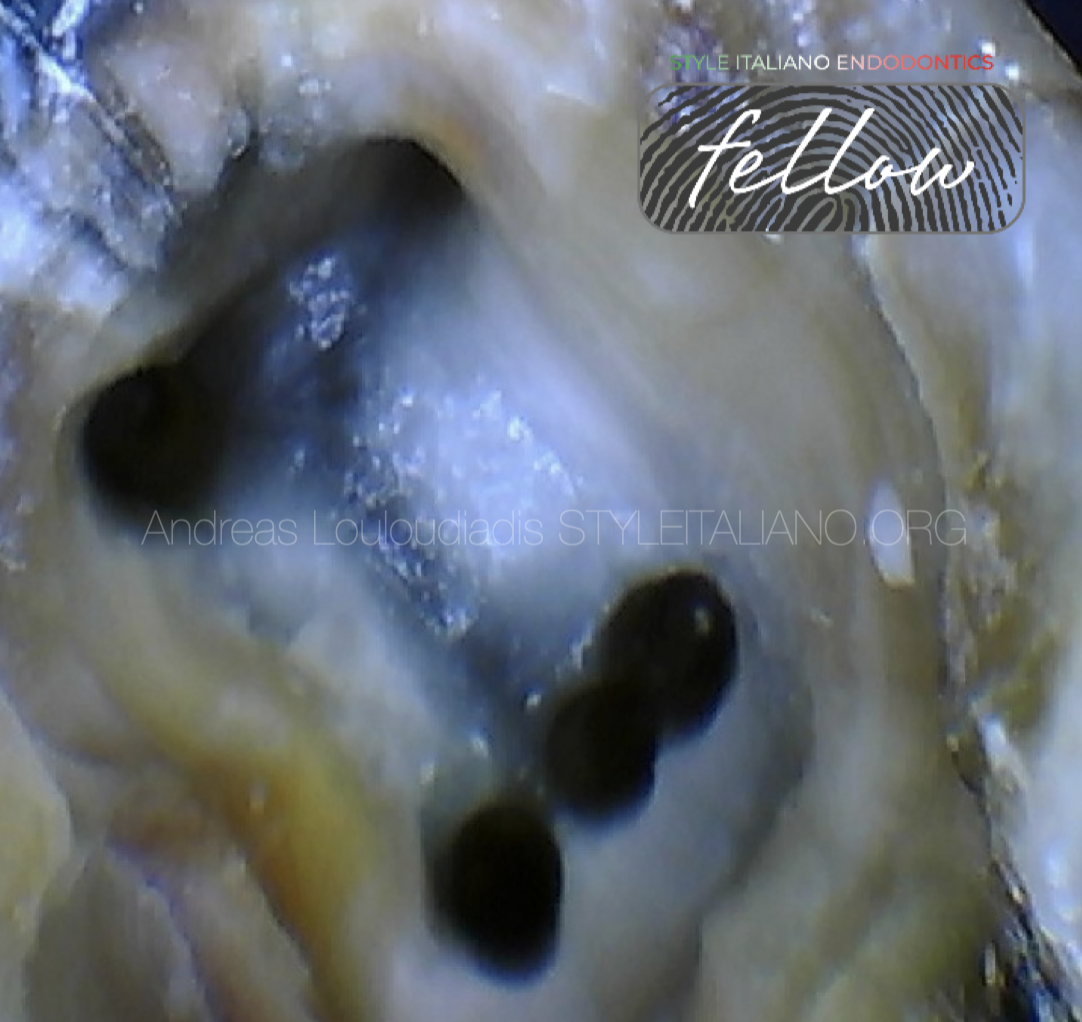
Fig. 2
Access opening and de-roofing the pulp chamber was done under rubber dam isolation and using dental operating microscope.
The groove on the floor of the pulp chamber between MB and ML canals was troughed 1 mm apically in mesio-axial region away from furcation/ danger zone to reveal MMC orifice.
Presence of MMC was confirmed by probing wih DG 16 probe looking for a “catch” sensation.
3 separate orifices were located on mesial side- MB, MM, ML.
D finders were used to negotiate the narrow MMC. All other canals were negotiated with K files.
MMC was confluent with ML canal, it originated as a separate orifice and joined ML canal 2-3 mm short of apex.
After enlarging the orifices, working length was determined with electronic apex locator and confirmed on IOPA xray.
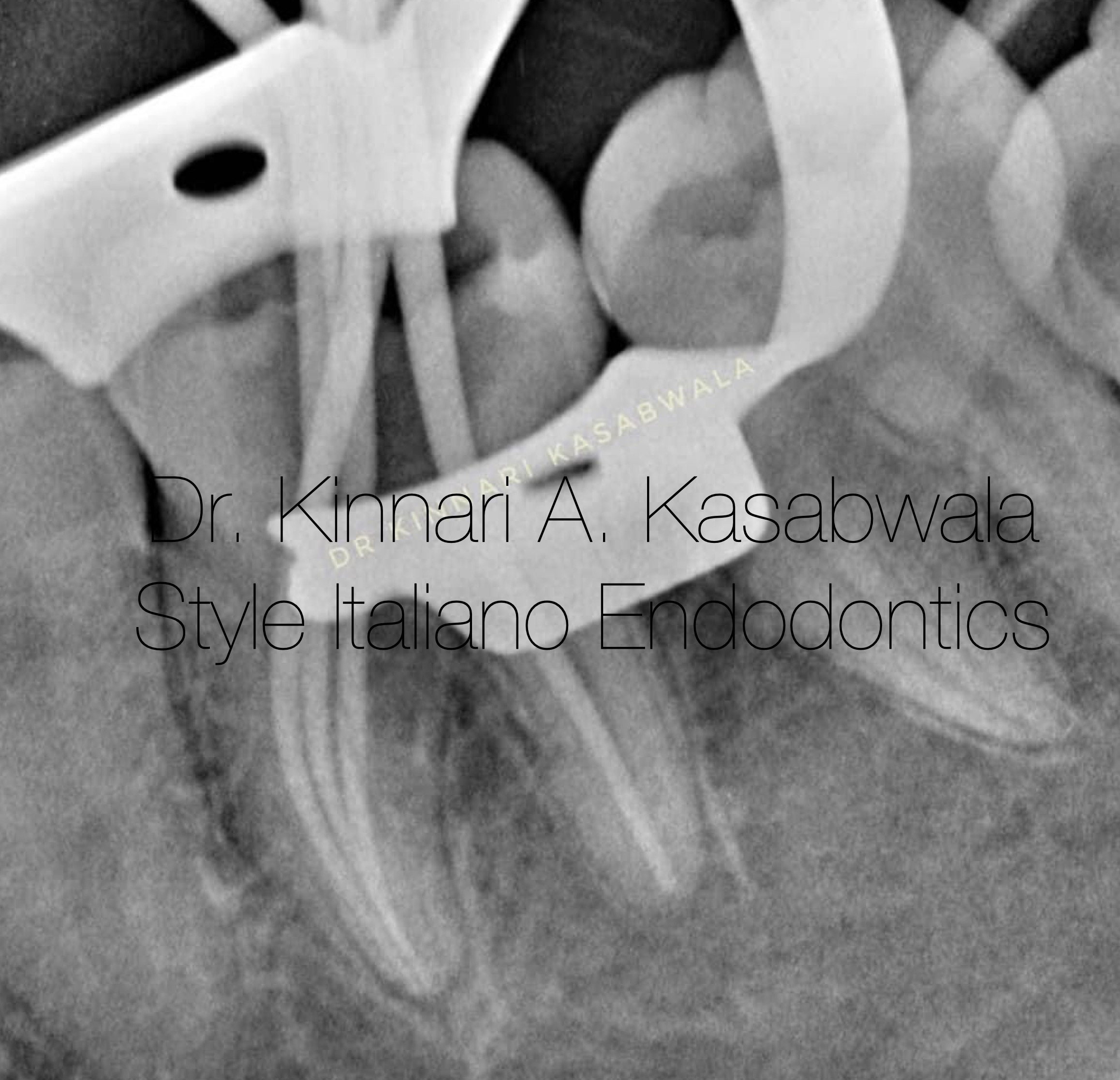
Fig. 3
Master cone xray:
4% tapered preparation was done in MB, ML & MM canals and 6% tapered preparation in D canal.
Corresponding master cones were used for cone fit xray.
Irrigation was done with 5.25% NaOCl and 17% EDTA and agitated with Endoactivator (Dentsply).

Fig. 4
Obturation was done with modified downpack technique using selected GP cones and CeraSeal bioceramic sealer.
Post endodontic restoration was done with composite. Patient was advised indirect crown prosthesis.
Final post-op xray:
Confluent anatomy- MMC seen converging with ML in apical third.
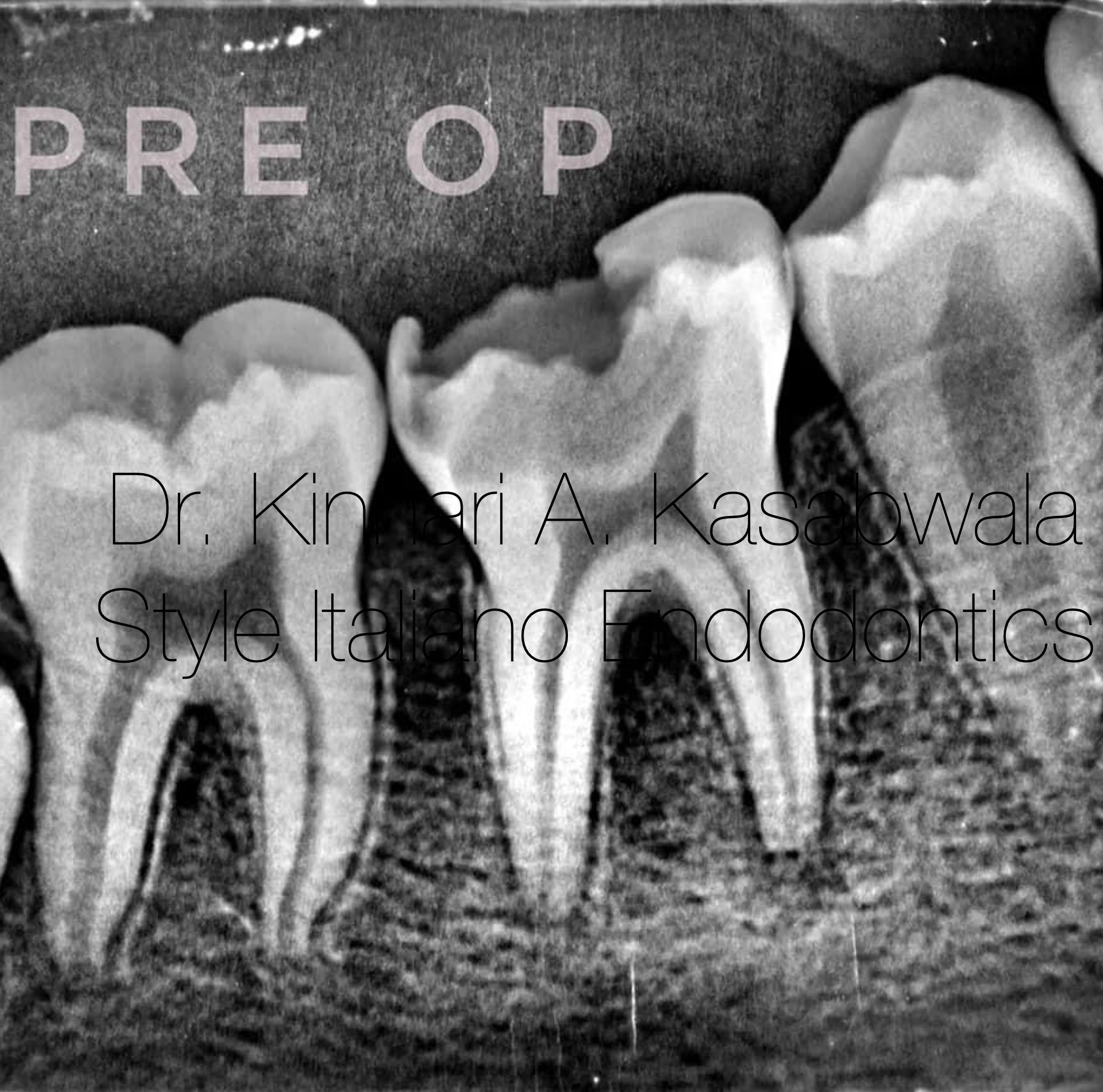
Fig. 5
Case 2:
14 year old patient was referred to the practice for continuous throbbing pain in 46.
On examination, 46 had deep caries and responded acutely to cold test.
IOPA xray revealed caries involving pulp with no significant changes in periapical region.
Diagnosis of symptomatic irreversible pulpitis was made.

Fig. 6
Access opening was done under rubber dam isolation using dental operating microscope.
Isthmus between MB and ML orifices was troughed and MMC was located and negotiated as described in the previous case.
A fin type morphology of MMC was seen, wherein the orifices merged after instrumentation and an instrument could freely pass between the 3 canals.
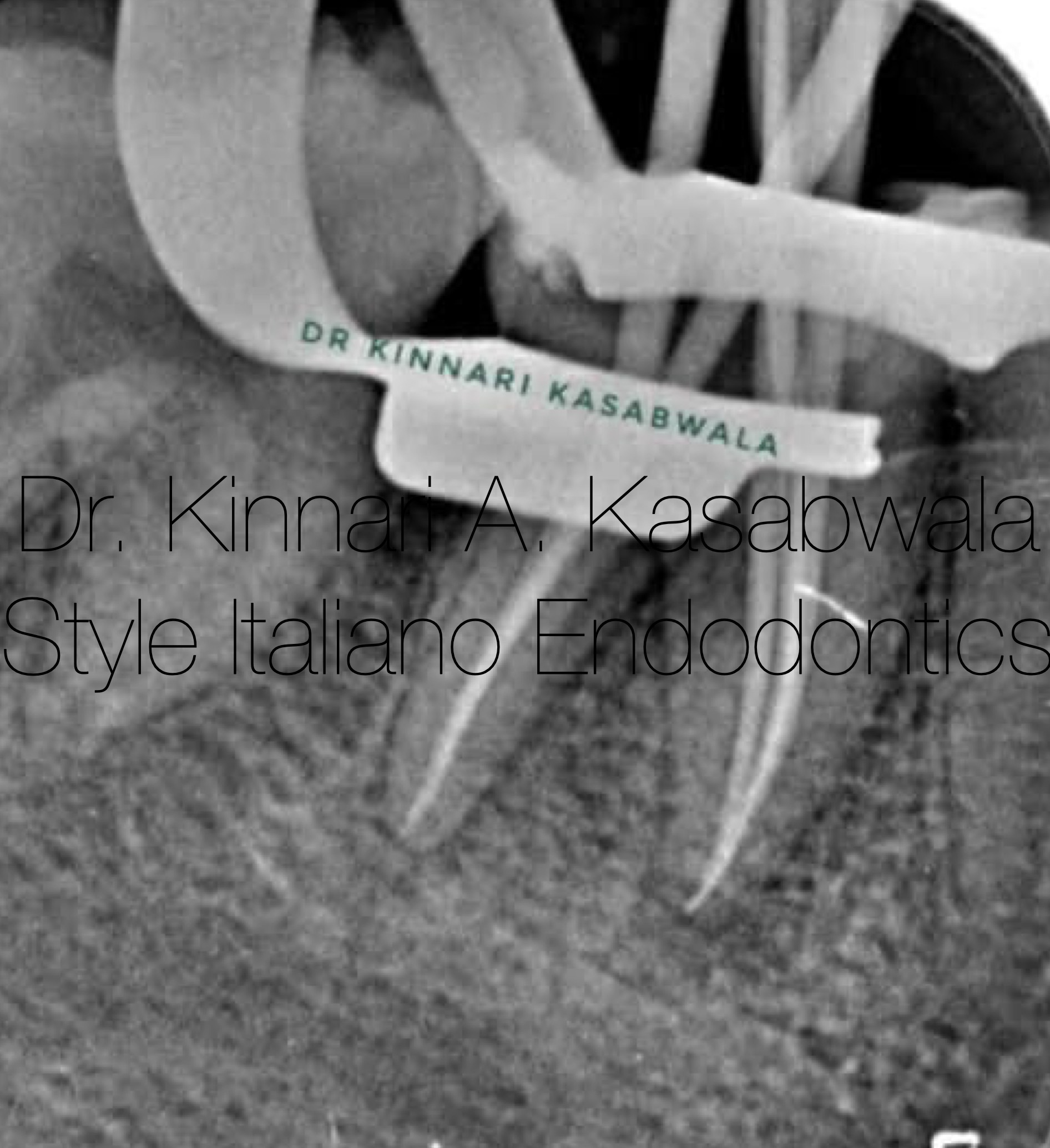
Fig. 7
All canals were shaped till 6% taper, MMC was shaped till 4% taper.
MB,ML, MMC were confluent at the apical third, same confluent anatomy was noted for DB, DL canals.
Corresponding master cones were used and cone fit IOPA xray was taken.
Ceraseal bioceramic sealer injected in MB canal is seen extruding out from MMC and ML canals signifying communication between all 3 canals and confirming fin type configuration coronally and confluence apically.

Fig. 8
Obturation was done with modified downpack technique using selected GP cones and CeraSeal bioceramic sealer.
Post endodontic restoration was done with composite.
MMC seen converging with MB and ML in apical third. Negotiated and scouted lateral canal filled with sealer.
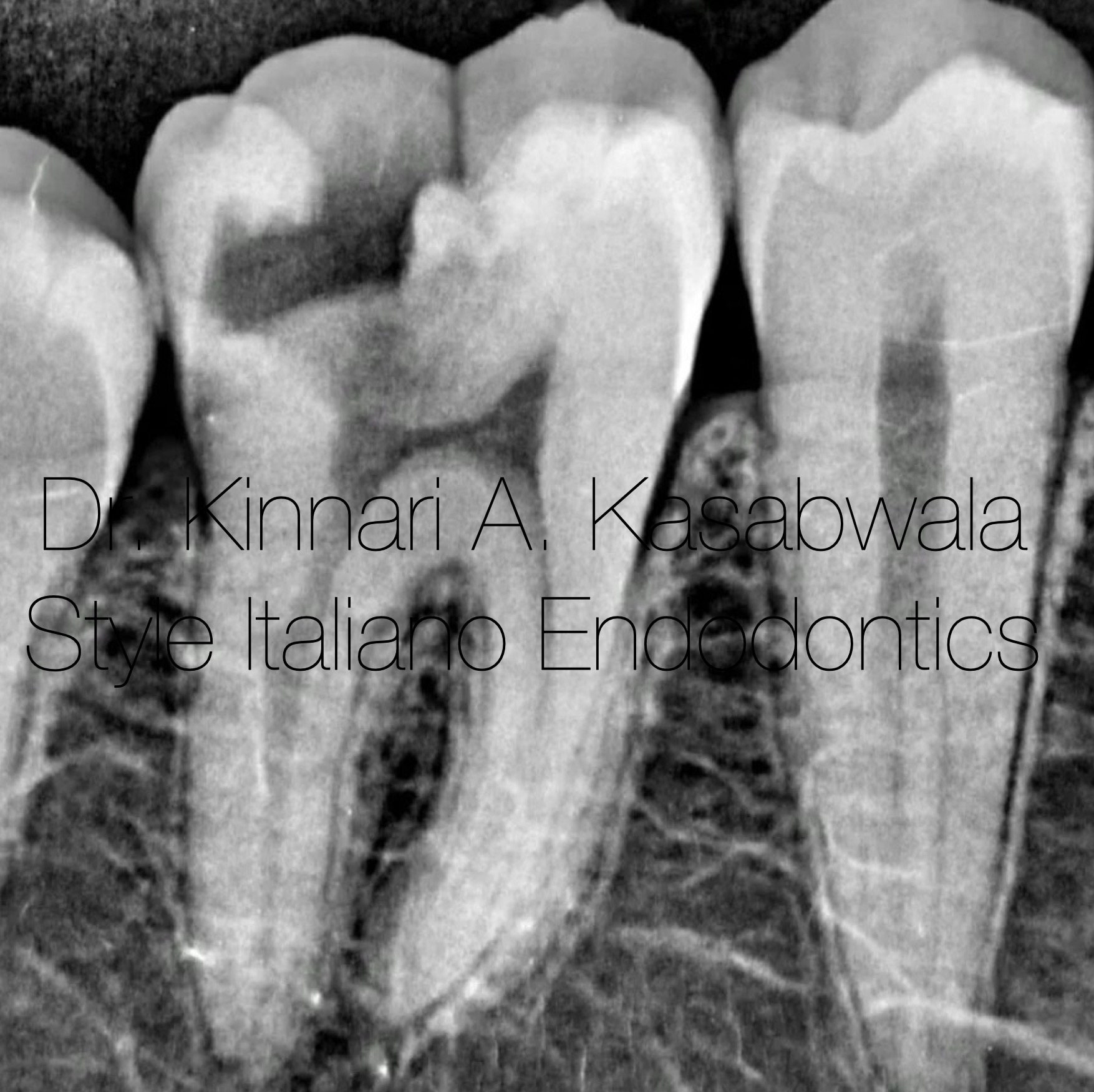
Fig. 9
Case 3: Radix paramolaris and middle mesial canal (MMC)
46 year old male patient came to the practice with severe spontaneous pain and pain on chewing due to food lodgement.
On examination, deep occlusal caries seen, tooth was tender on percussion and gave a strong response to cold test.
IOPA xray revealed deep caries approaching the distal pulp horn with minor changes in apical periodontium.
Diagnosis of symptomatic irreversible pulpitis with symptomtic apical periodontitis was made.

Fig. 10
Access opening was done under rubber dam isolation and using dental operating microscope.
After locating, MB and ML canal, minor troughing was done in the groove connecting them as previously described. “Catch” was noticed for MMC near ML canal using DG 16 probe, orifice was enlarged and the thin MMC was negotiated with D finder file.
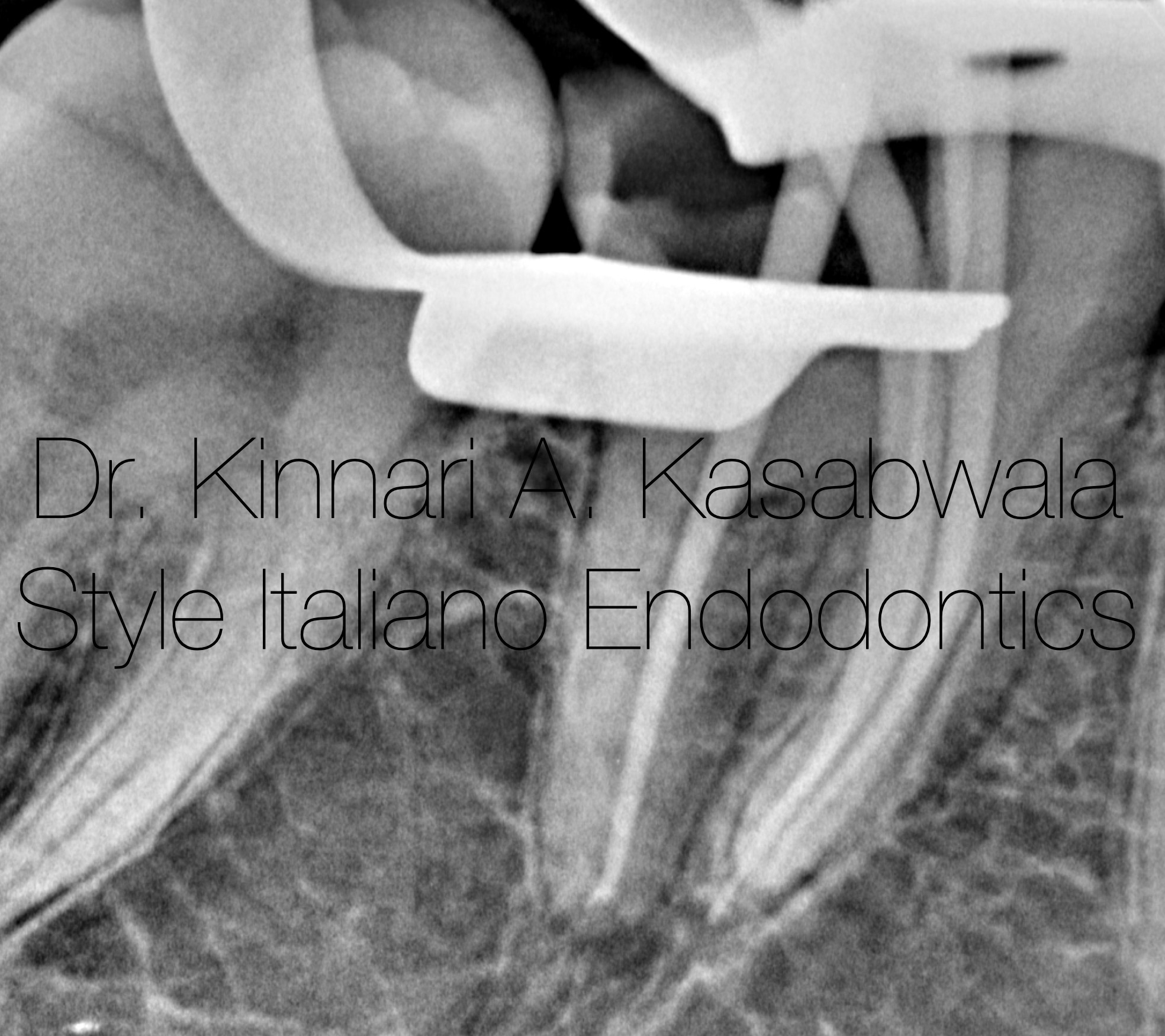
Fig. 11
Shaping was done with 4% tapered Hero Gold files for MB,ML,MMC and 6% tapered preparation was done for D canal.
Corresponding master cones were selected and cone fit IOPA xray was taken
Ceraseal bioceramic sealer injected in MMC expressed out through ML canal confirming anastomosis and confluent configuration.
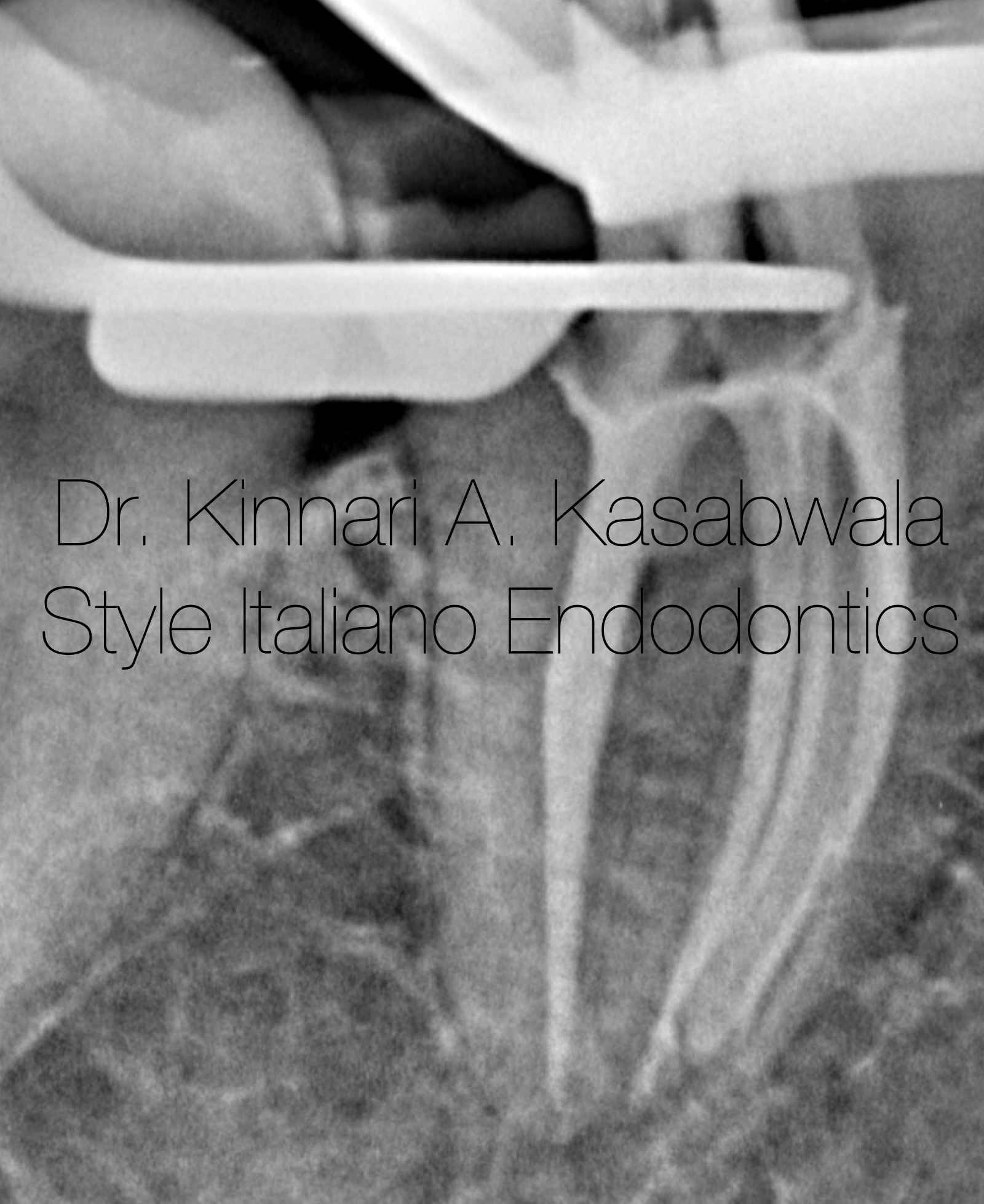
Fig. 12
Obturation was done with modified downpack technique using GP cones and Ceraseal bioceramic sealer.
Confluent anatomy- MMC seen anastomosing with ML in apical third.

Fig. 13
Post-op IOPA xray after obturation and composite post endodontic restoration.
Indirect prosthetic crown advised.
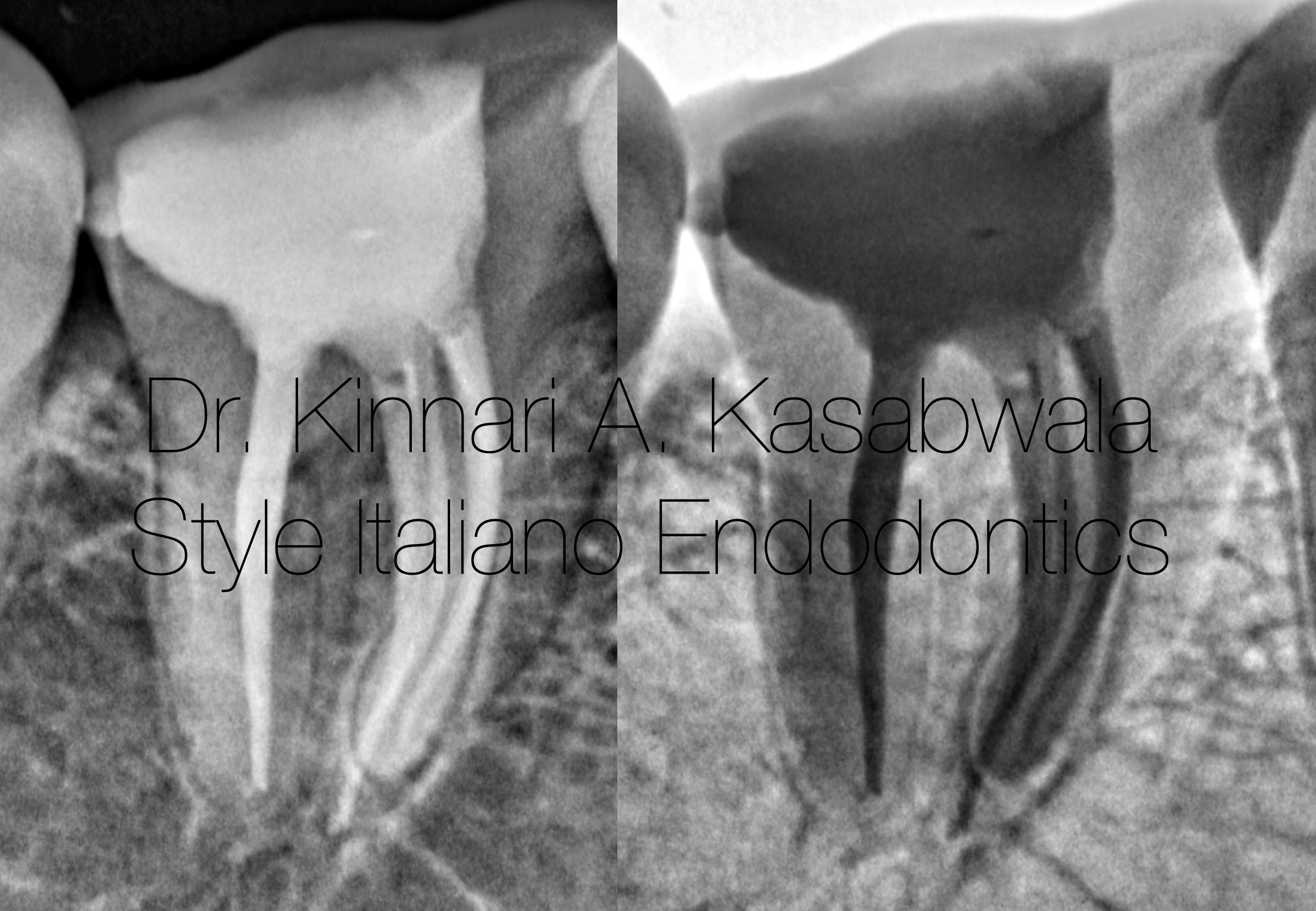
Fig. 14
Distal shift angulated post-op IOPA xray.

Fig. 15
- D.S. from Nair hospital dental college, Mumbai (2011-2016)
- D.S. specializing in Conservative dentistry and Endodontics from Meenakshi Ammal dental college and hospital, MAHER University, Chennai (2017-2020)
She is awarded with the following:
- "Emerging star 2019" for being the outstanding postgraduate by Conservative dentistry and endodontics association of Tamil Nadu
- Selected as top finalist at the National level in Endodontics for "Young Achiever award 2020" by Indian association of conservative dentistry and endodontics
- Gold medal from MAHER university for securing first position in MDS final examination.
- "Best outgoing student" for year 2020 by Conservative dentistry and endodontics department of Meenakshi Ammal dental college and hospital, Chennai
- Awarded "Best student of the year" for years 2017-2018, 2018-2019, 2019-2020 amongst the post graduate students at Endodontics department Meenakshi Ammal dental college and hospital
She is a patent holder of "Indigenous cost-effective biofilm flow cell model and bubble trap" under Intellectual property India, Government of India.
She has authored and co-authored several publications in National and International journals.
She is recently inducted as a national key opinion leader with Bombay dental surgical.
She is recently inducted as a fellow with Style Italiano endodontics forum from May 2023.
Dr. Kinnari Kasabwala is currently practising as a private practioner, specializing in micro-endodontics at Dr Kasabwala dental speciality clinic in Mumbai.
Her interests are Endodontics, Dental aesthetic procedures and multi-disciplinary dentistry.
Conclusions
The MM canal can be detected by careful probing between the MB and ML canal along the pulp chamber floor and looking for a “catch” or a “stick” feeling using a sharp endodontic explorer (DG 16 probe), a small stiff stainless steel K-file or Micro-openers.
In vital cases, bleeding points from orifices or the flow of blood into the isthmus and fins can serve as a roadmap to recognize the underlying anatomy referred to as the Red Line Test.
The guided troughing technique involves using ultrasonics tips and troughing under magnification, from the ML canal, progressing within the groove to the MB canal . This 1-2 mm troughing should be done in an apical direction at the expense of the mesial–axial wall away from the furcation area (danger zone) to avoid the chances of strip perforation. While troughing with ultrasonic tips, the grooves in the pulp chamber floor get packed with dentin chips which helps in the identification of hidden orifices (White Line Test).
MM canal can also be identified by champagne bubble test and methylene blue test.
Most MMCs are narrow, tortuous, curved, or joined to one of the primary root canals; establishing a good glide path and preparing these canals to smaller sizes with 4% taper is preferable.
Missing out on identifying and negotiating MMCs can lead to endodontic failure if considerable amount of infected pulp tissue is left in the canal.
Bibliography
Bukhary S, Alkahtany S, Bukhari A, et al. Prevalence of middle mesial canal using cone beam computed tomography: A systematic review and meta-analysis. The Saudi Dental Journal, 2023.
Penukonda R, Pattar H, Nambiar P, Al-Haddad A. Middle mesial canal in mandibular first molar: A narrative review. The Saudi Dental Journal, 2023
Yang, Y., Wu, B., Zeng, J. et al. Classification and morphology of middle mesial canals of mandibular first molars in a southern Chinese subpopulation: a cone-beam computed tomographic study. BMC Oral Health, 2020.
N. Akbarzadeh, A. Aminoshariae, N. Khalighinejad, J.M. Palomo, A. Syed, J.C. Kulild, G. Ghazal Sadeghi, A. Mickel
The association between the anatomic landmarks of the pulp chamber floor and the prevalence of middle mesial canals in mandibular first molars: an in vivo analysis
J. Endod. 2017.
Jabali AH. Middle Mesial and Middle Distal Canals in Mandibular First Molar. J Contemp Dent Pract 2018.