Management of C shaped canal in mandibular second molar
17/03/2025
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
C shaped root canal configuration is an aberrant canal anatomy, common in the mandibular second molars with prevalence ranging from 2.7% to 45.5% in different populations.
Failure of fusion of Hertwig’s epithelial root sheath (HERS) onto the buccal or lingual root surface results in a conical or prism shaped root. This, together with thin inter-radicular ribbon-shaped isthmus connecting them, forms the C-shaped cross-sectional anatomical configuration. The C-shape configuration can either follow the same course throughout the root length, or may present with two/three separate canals within the C-shaped groove.
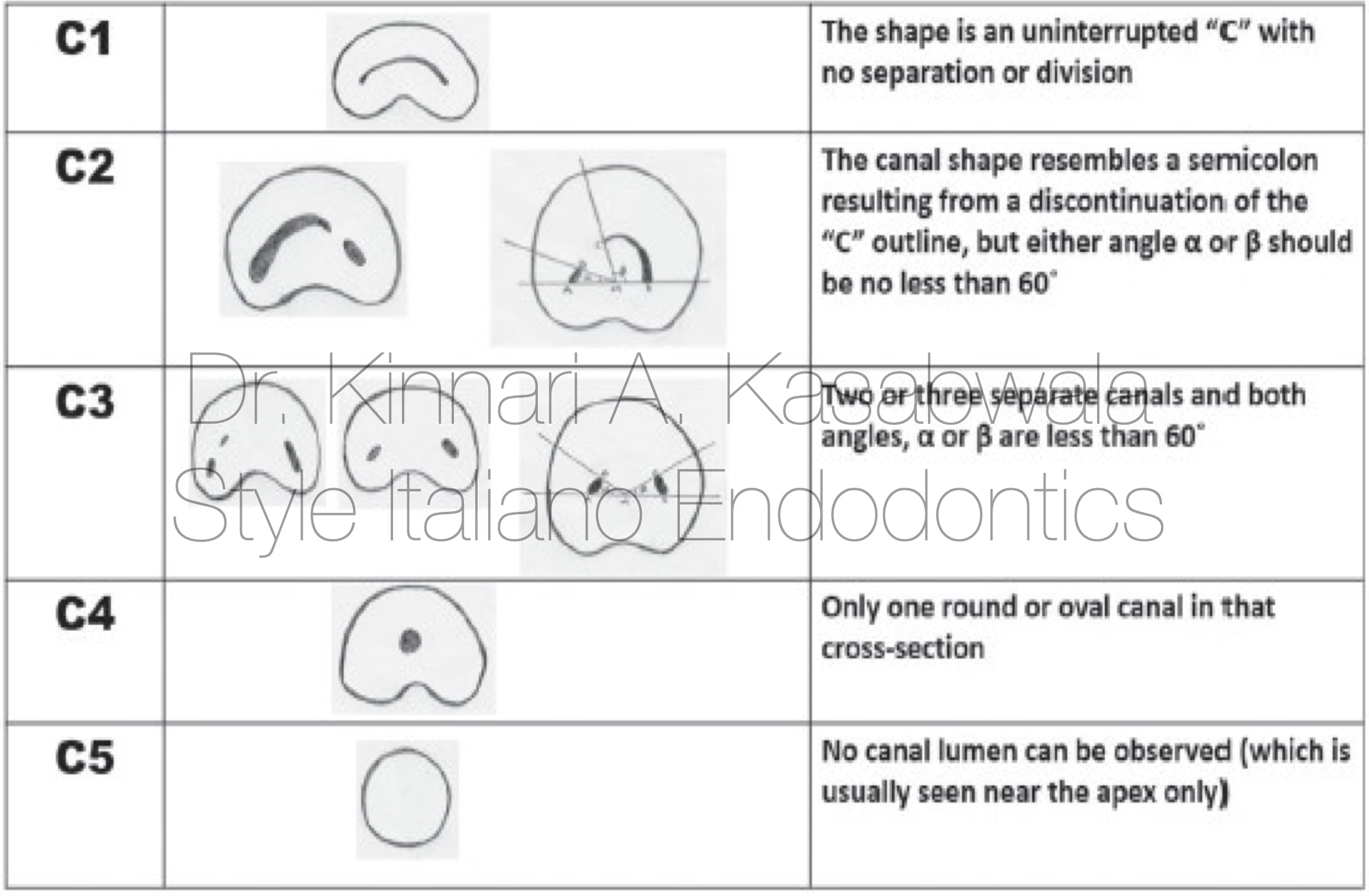
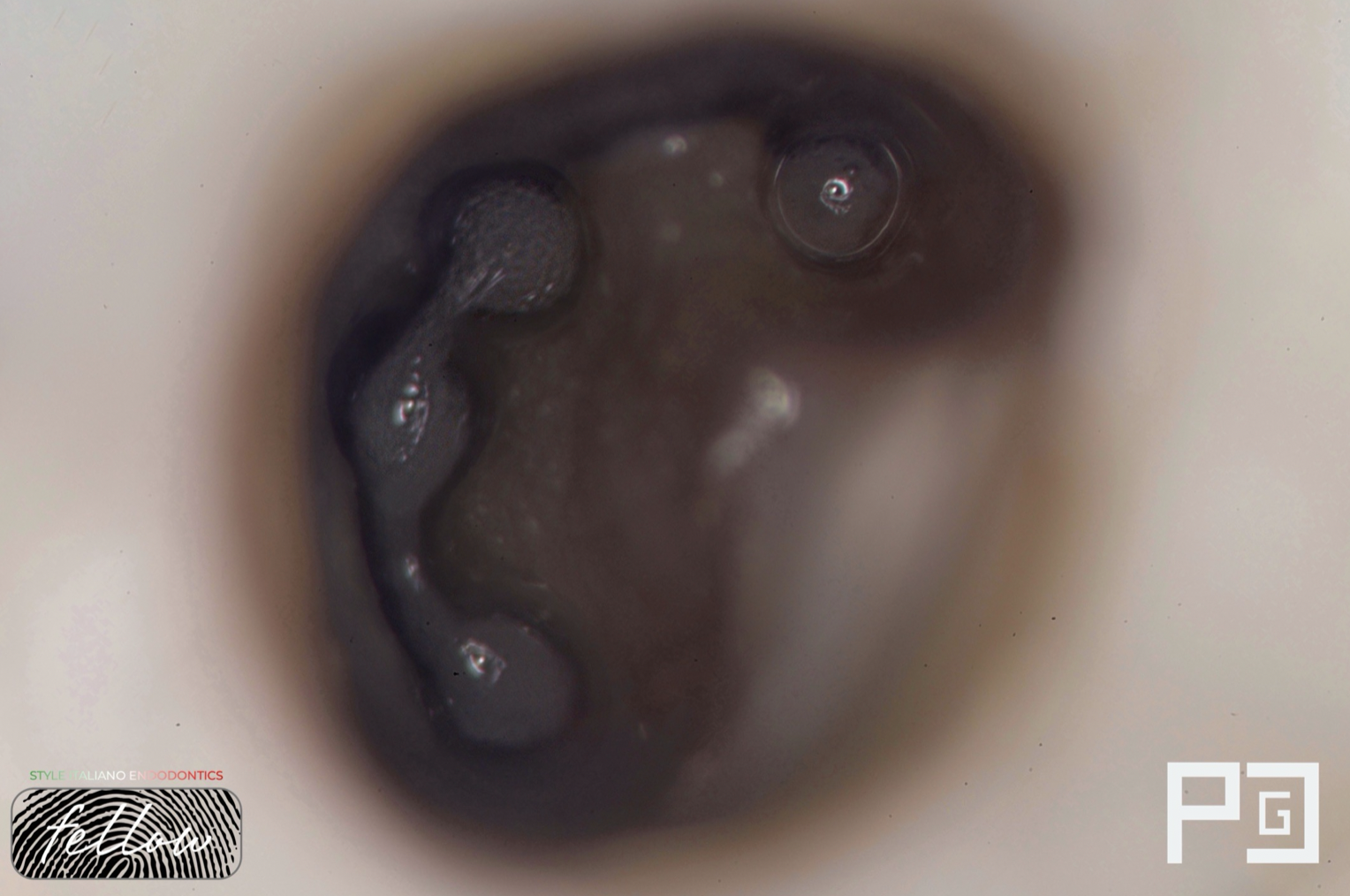
Fig. 1
Fan et al modified Melton’s method into the following categories:

Fig. 2
Patient reported with severe, throbbing, continuous pain in lower right back tooth region.
On examination:
Deep restoration wrt tooth 47
47 was tender on percussion
Sensibility test- No response on cold test
Provisional diagnosis: Pulp necrosis with symptomatic apical periodontitis in 47.
Access opening was done under rubber dam isolation
Deep pulp chamber was widened using ultrasonic tips (Start X, Dentsply Sirona).
DG-16 probe was used to examine the floor of pulp chamber and look for a “catch” feeling
Distal canal was patent, narrow opening of ML canal was appreciable on probing, MB canal had sclerosed canal opening.
Canals were negotiated with 8 &10K file (Mani) with gentle watch winding motion.
Troughing was done using ultrasonic tips (Start-X, Dentsply) between ML and D canal orifices to remove dentinal shelf and provide straight line access to initial curvature of canals.
Orifice enlargement was done initially in ML and D canals using SX orifice opener (Dentsply)
Path files were used to create a glide path - 14,4% Easy path file (Endostar)
(MB canal opening was subsequently located and negotiated)
Sequential enlargement of canals was done with Hero Gold files (Micro Mega) in the following manner:
17,4%
20,4%
25,4%
30,4%
Video shows shaped ML and D canals with appreciable dentinal shelf removal in between the orifices
Troughing was done with ultrasonic tip to discover MB canal orifice (sclerosed)
Followed by sequential shaping steps as described previously.
Irrigation was done with 5.25% NaOCl in all 3 canals using side-vented needle.
Negative aspiration in video shown to confirm apical anastomosis between all 3 canals.
Activation of 5.25% NaOCl in all 3 canals was done using Endoactivator (Dentsply) for 4 cycles, 40 seconds/ canal.

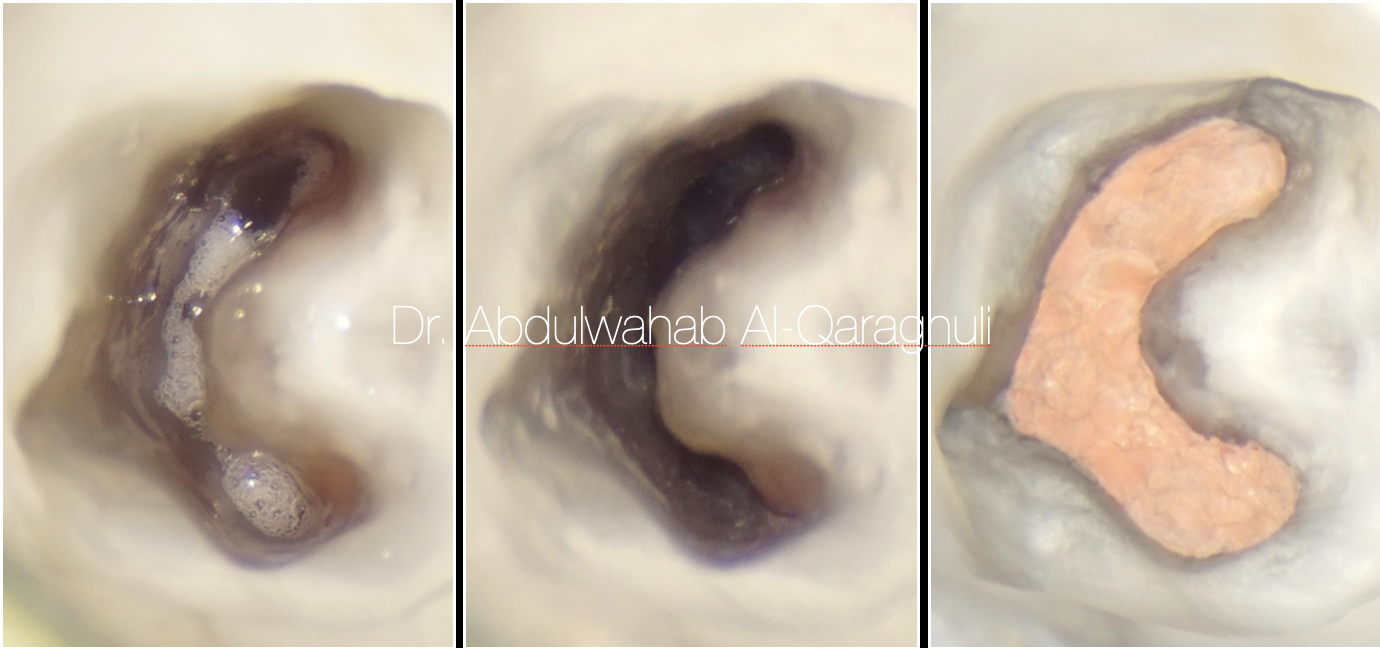
Fig. 3
Master cone IOPA
Shaped and cleaned canals ready for obturation
Injection of Ceraseal bioceramic sealer (Meta Biomed) and insertion of master cones was done sequentially in all 3 canals
Sheering of GP was done at the level of orifice followed by modified downpack technique (EQ-V system, Meta Biomed)
Modified downpack of GP was done till level of orifices and intervening isthmus downpacked
Followed by backfill with thermoplasticised GP

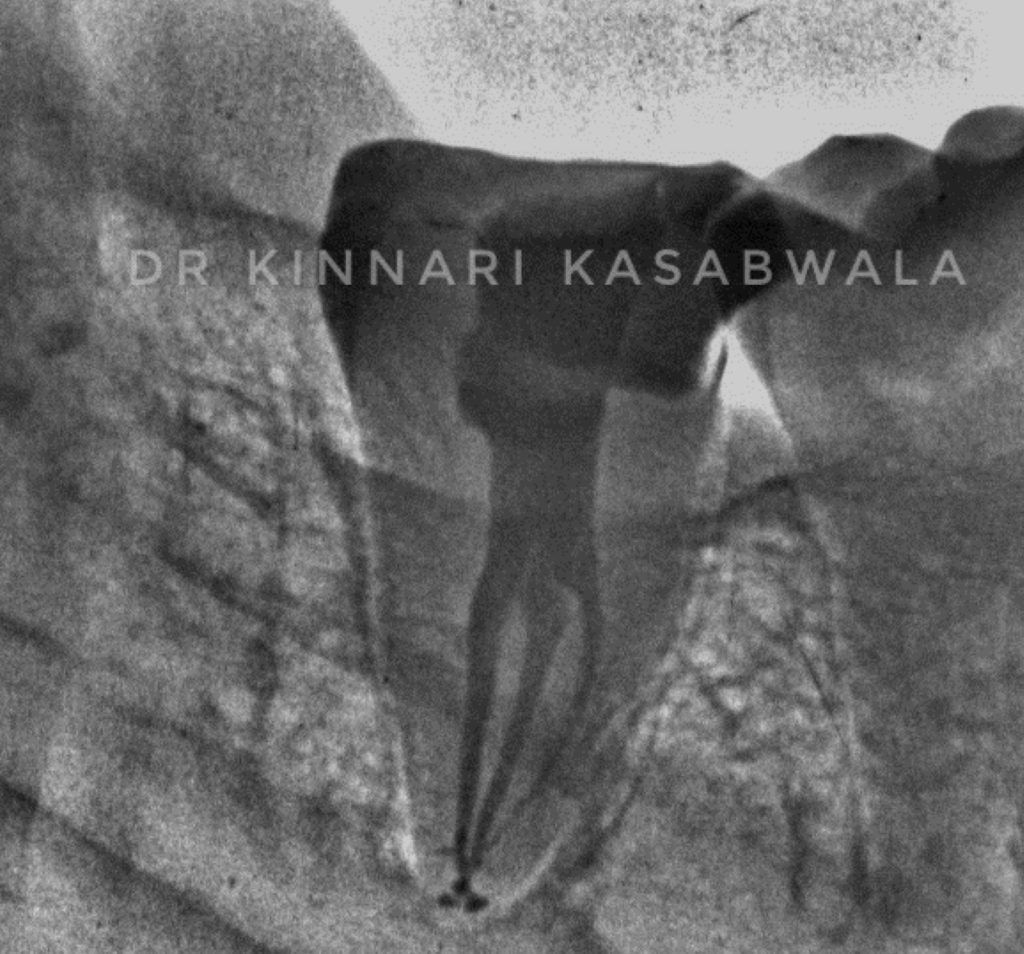
Fig. 4
Post-op IOPA- Straight and mesial angulation
- 2 portals of exit
- 1-3-2 anatomy
- Lateral canal fill distally

Fig. 5
Post-op IOPA- Straight and mesial angulation (inverted)

Fig. 6
About Dr Kinnari Abhilash Kasabwala
- B.D.S. from Nair hospital dental college, Mumbai (2011-2016)
- M.D.S. specializing in Conservative dentistry and Endodontics from Meenakshi Ammal dental college and hospital, MAHER University, Chennai (2017-2020)
She is awarded with the following:
- "Emerging star 2019" for being the outstanding postgraduate by Conservative dentistry and endodontics association of Tamil Nadu
- Selected as top finalist at the National level in Endodontics for "Young Achiever award 2020" by Indian association of conservative dentistry and endodontics IACDE.
- Gold medal from MAHER university for securing first position in MDS final examination.
- "Best outgoing student" for year 2020 by Conservative dentistry and endodontics department of Meenakshi Ammal dental college and hospital, Chennai
- Awarded "Best student of the year" for years 2017-2018, 2018-2019, 2019-2020 amongst the post graduate students at Endodontics department Meenakshi Ammal dental college and hospital
She is a patent holder of "Indigenous cost-effective biofilm flow cell model and bubble trap" under Intellectual property India, Government of India.
She has authored and co-authored several publications in National and International journals.
She is recently inducted as a national key opinion leader with Bombay dental surgical.
She is recently inducted as a fellow with Style Italiano endodontics forum from May 2023.
Dr. Kinnari Kasabwala is currently practising as a private practioner, specializing in micro-endodontics at Dr Kasabwala dental speciality clinic in Mumbai.
Her interests are Endodontics, Dental aesthetic procedures and multi-disciplinary dentistry.
Conclusions
Recognition of a C-shaped canal configuration before treatment can facilitate effective management.
Cleaning, shaping and obturation of C-shaped canals is difficult due to the resulting intricate root canal system with presence of numerous inaccesible fins or isthmi that connect individual canals.
CBCT, magnification, rotary and hand instrumentation assisted with activated irrigation and modified obturation techniques have positively influenced the prognosis of this anatomical variant.
Bibliography
Cooke HG, 3rd, Cox FL. C-shapedcanal configurations in mandibular molars. J Am Dent Assoc. 1979;99:836–9.
Fan B, Cheung GS, Fan M, Gutmann JL, Bian Z. C-shaped canal system in mandibular second molars: part I - anatomical features. J Endod. 2004;30(12):899-03
Fan B, Cheung GS, Fan M, Gutmann JL, Fan W. C-shaped canal system in mandibular second molars: Part II: Radiographic features. J Endod. 2004
Weine FS. The C-shaped mandibular second molar: Incidence and other considerations. Members of the Arizona Endodontic Association. J Endod. 1998;24:372–5.
Jin GC, Lee SJ, Roh BD. Anatomical study of C-shaped canals in mandibular second molars by analysis of computed tomography. J Endod. 2006;32:10–3.
Zheng Q, Zhang L, Zhou X, Wang Q, Wang Y, Tang L, et al. C-shaped root canal system in mandibular second molars in a Chinese population evaluated by cone beam computed tomography. Int Endod J. 2011;44:857–62.
Fernandes M, de Ataide I, Wagle R. C-shaped root canal configuration: A review of literature. J Conserv Dent. 2014