
Management of an upper second molar with a restorative approach
23/09/2023
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Adhesive procedures have changed the way of restoring endodontically treated teeth.
Postless approaches have been proposed to improve and restore teeth.
The preservation of the dental structure of endodontically treated teeth is essential for this.
Before performing any endodontic procedure, one must know how the final restoration of that tooth will be handled and whether the procedure can be optimized during root canal treatment.

Fig. 1
A 52-year-old female is referred for the endodontic treatment of the upper second molar due to intense cold pain.The examination of the initial radiograph reveals very narrow canals.
Pulp diagnosis: symptomatic irreversible pulpitis.
Periapical diagnosis: normal periapical tissues
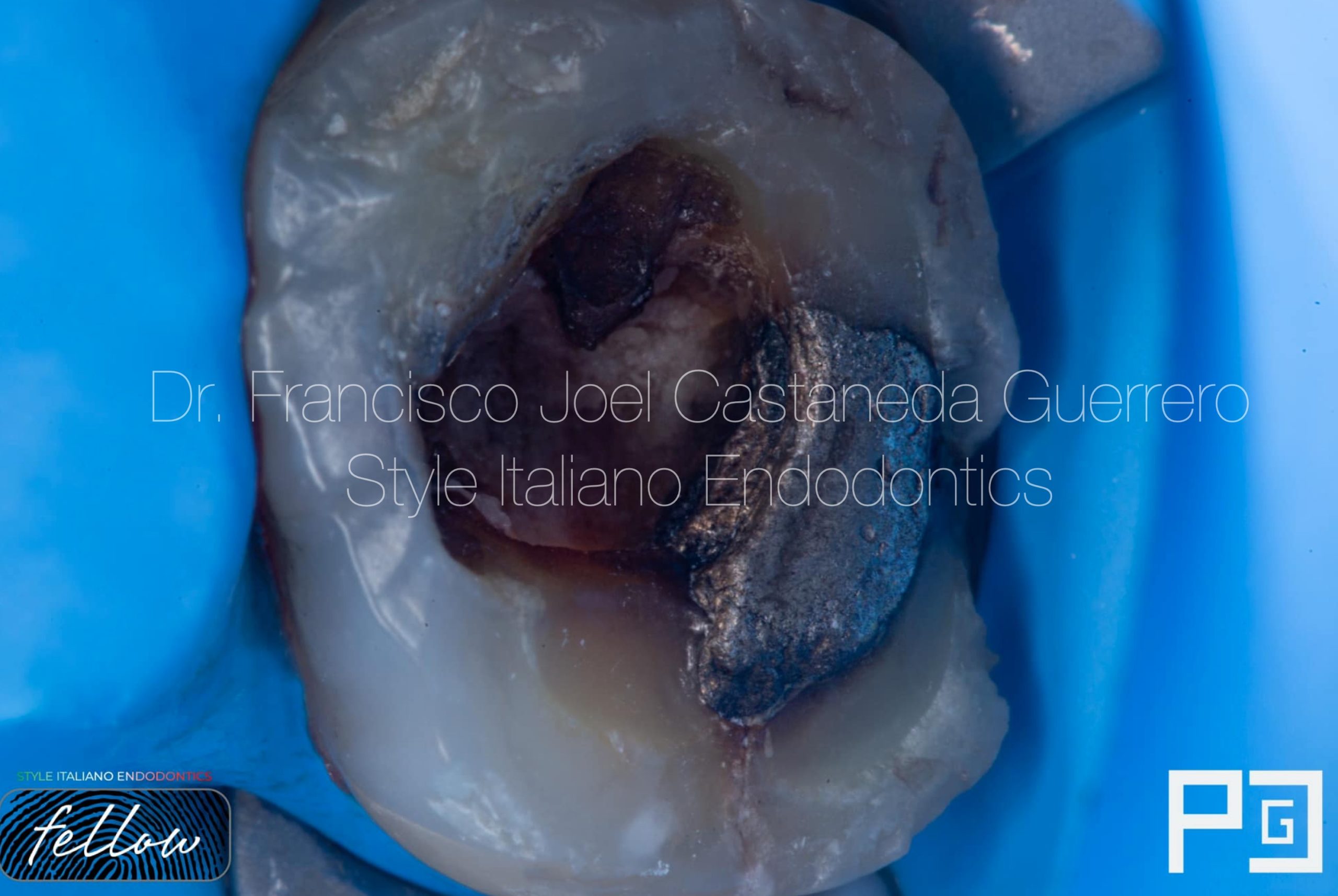
Fig. 2
Initial situation after anesthesia and rubber dam placement
As seen in the image, presence of caries and amalgam fracture.
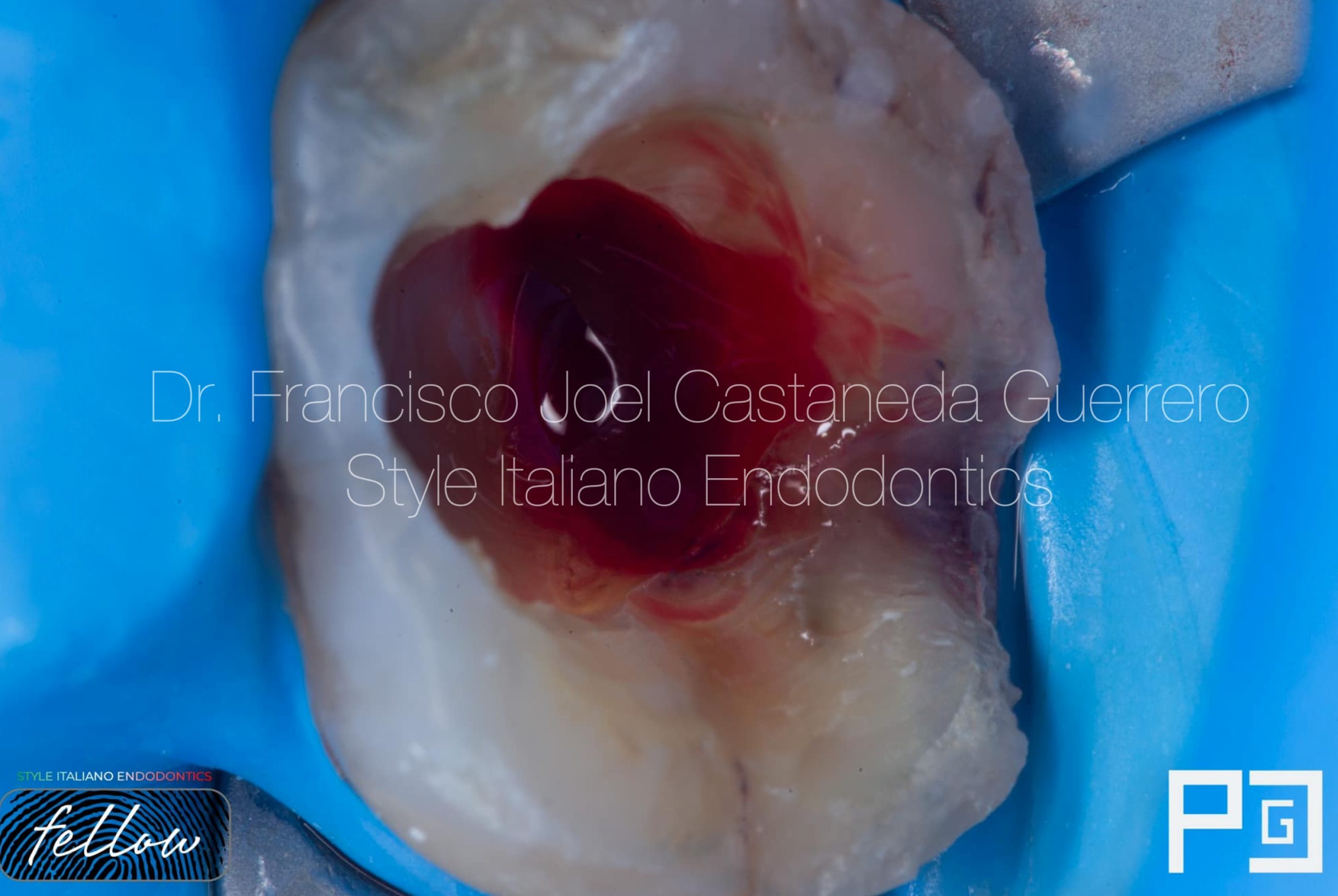
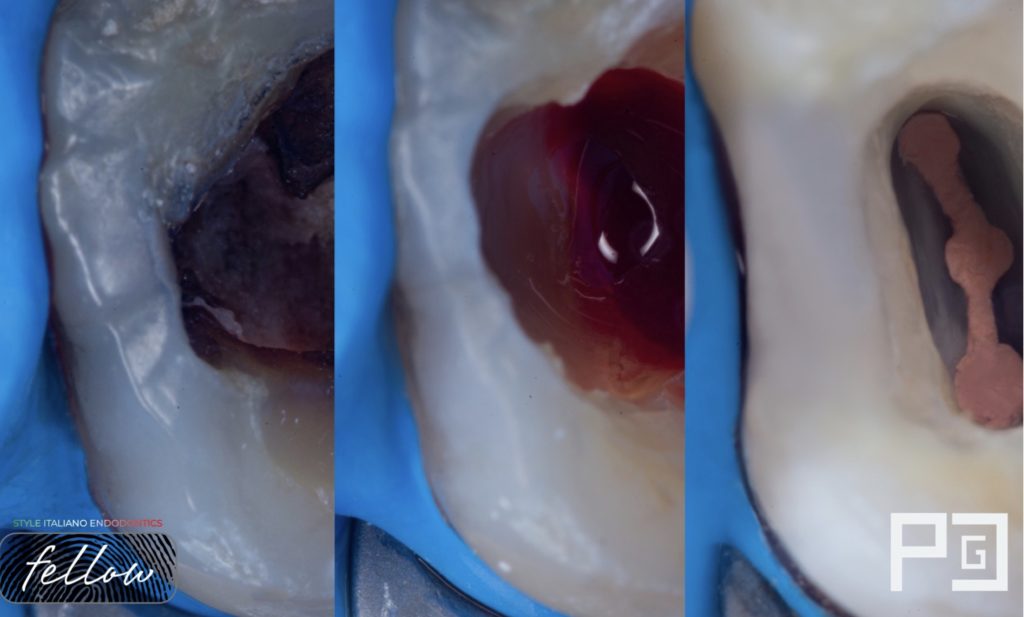
Fig. 3
After removing the carious tissue and the bad restoration, access to the cavity was made, in this case profuse bleeding, for this the cervical third was instrumented a little to remove the pulp tissue and contain or reduce the bleeding, it was irrigated with hypochlorite sodium or saline preference only in this step.
Unsupported enamel was removed from the mesial surface and the edges were smoothed.
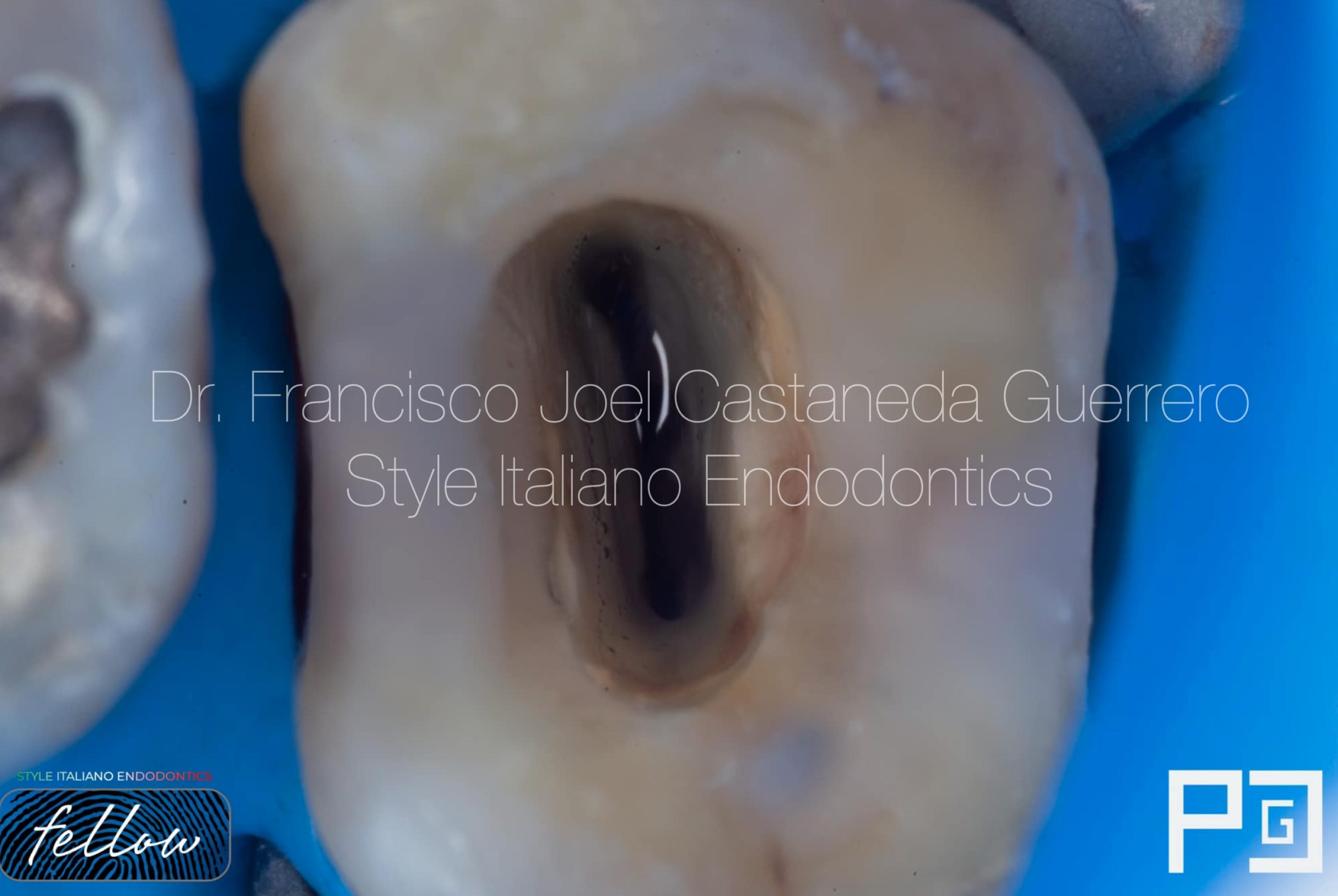
Fig. 4
A mesial and distal margin elevation and a pre-endodontic sealing of the dentin or a resing coating were performed.
This will help a lot in the adhesive strength, since the sodium hypochlorite will not be in contact with the collagen of the dentin.
Access was refined with the help of ultrasound tips.
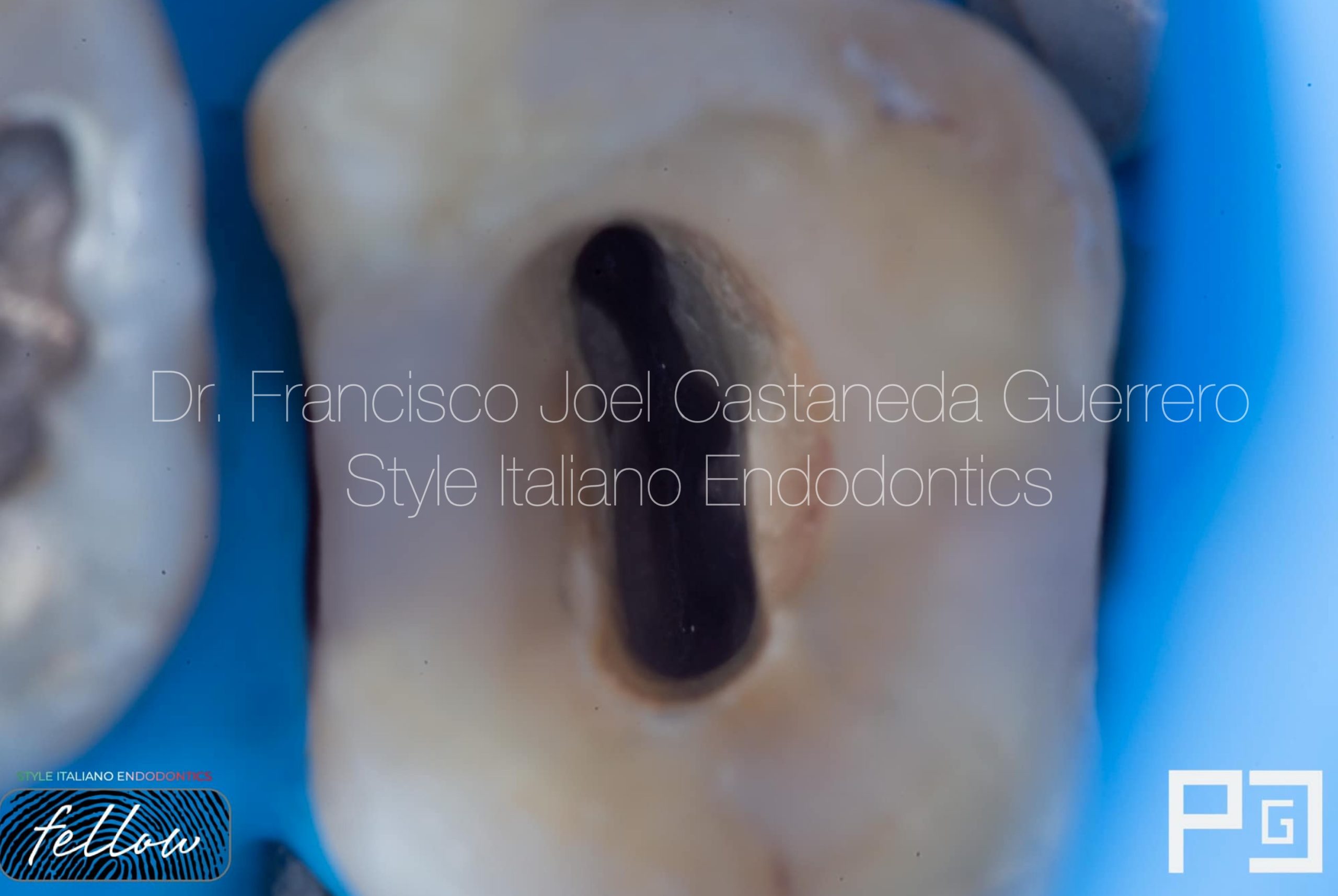
Fig. 5
It was instrumented with rotary martensitic files with taper 04 due to the anatomy of the canals up to a caliber 35.04.
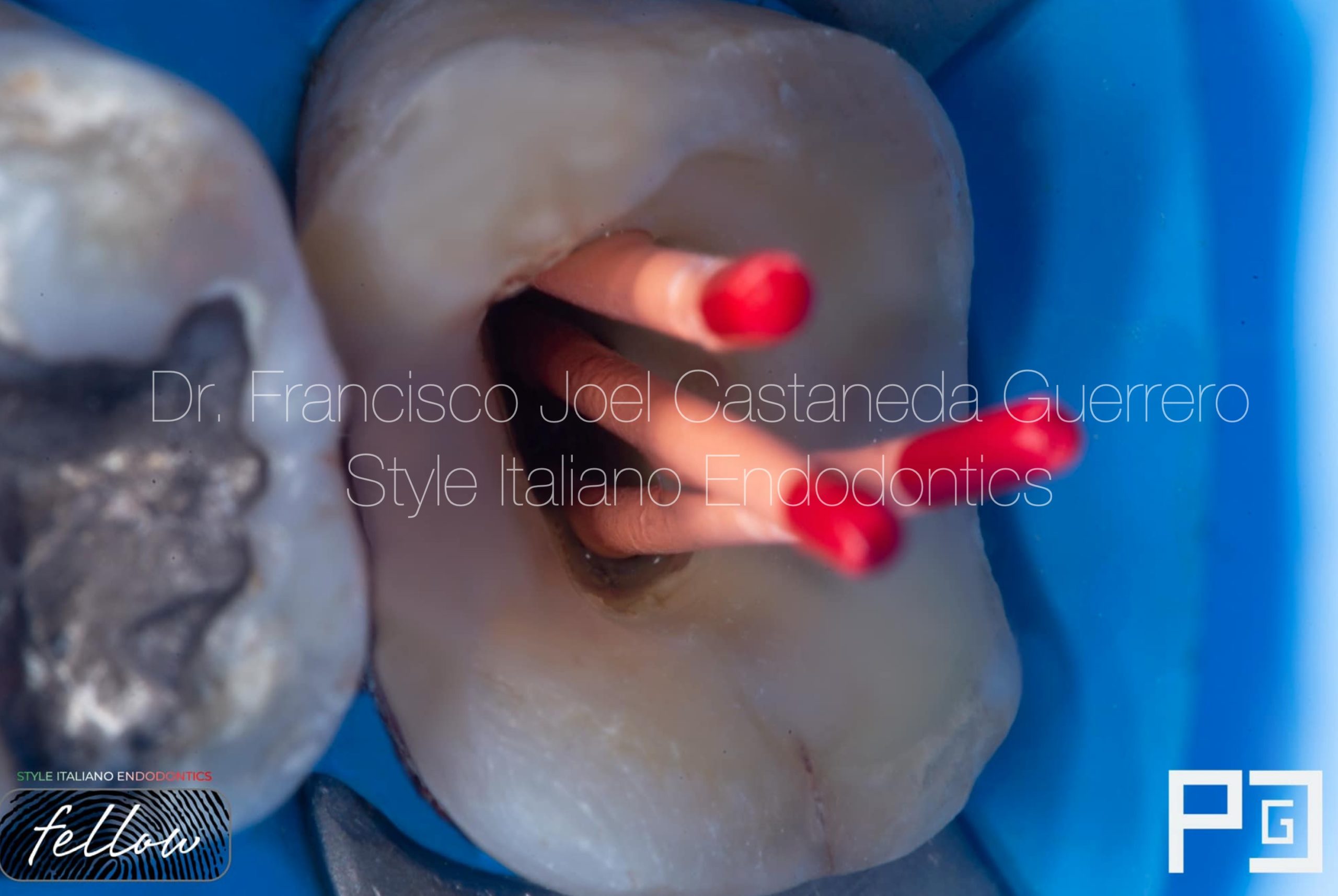
Fig. 6
Cone fit photograph
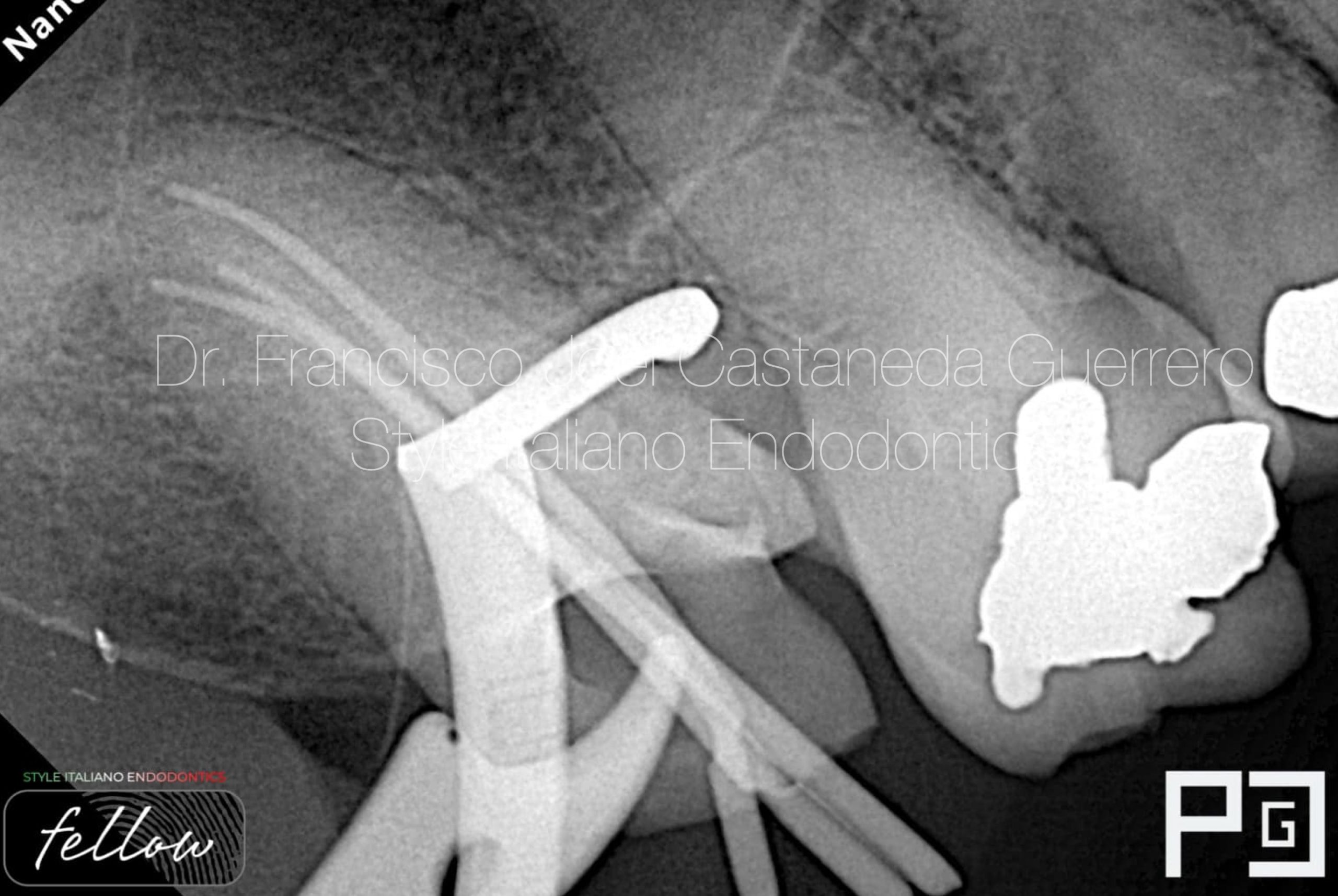
Fig. 7
Cone Fit X-ray
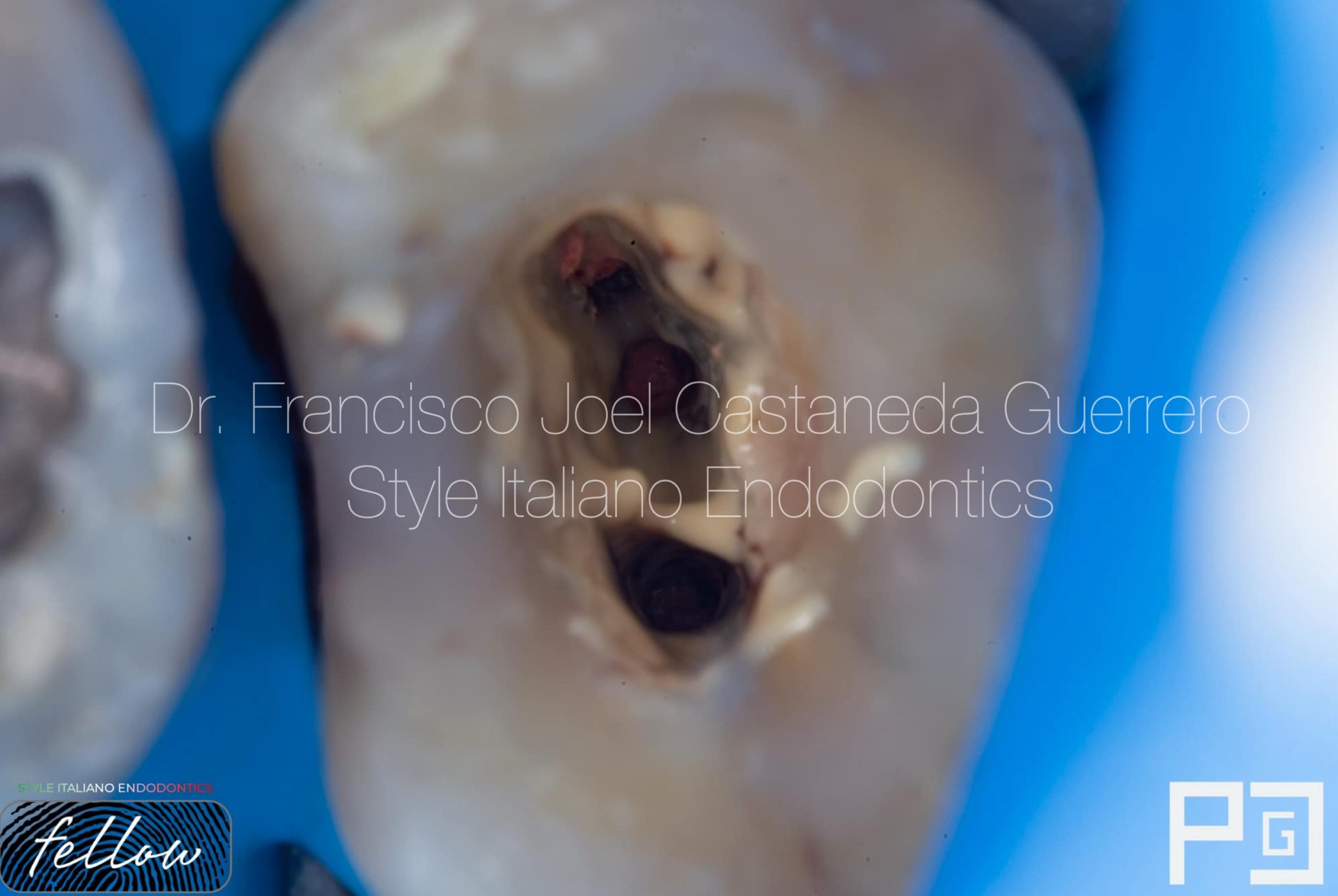
Fig. 8
Downpack was made leaving 3-5 mm of guttapecha

Fig. 9
Whenever the continuous wave technique is performed, the adjustment must be verified with an x-ray, this test is known as downpack.

Fig. 10
The backfill was finished and the pulp chamber was cleaned without excess cement or gutta-percha.
For this part, alcohol is used to better remove the resin-based sealer.
A build up was made with short fiber reinforced composite and the preparation for an indirect restoration was finished

Fig. 11
Final X-ray

Fig. 12
Mesial shift

Fig. 13
Inverted Xray
Conclusions
Knowing how the management of the endodontically treated tooth will be is important, it has a relationship to how we are going to make the access, how it should be instrumented, if space will be made for a post or not, if an indirect restoration will be made, if onlay or overlay, if it will only be reconstructed with composite resin or if a crown will be made
So we must think about what the final restoration will be like and based on that, address it endodontically.
Bibliography
- Ree M, Schwartz R. The Endo-Restorative Interface: Current Concepts, Dental Clinics of North America; 54: 345-374, 2010
- The Effects of Endodontic Access Cavity Preparation Design on the Fracture Strength of Endodontically Treated Teeth: Traditional Versus Conservative Preparation Taha Özyürek, Özlem Ülker, Ebru Özsezer Demiryürek, Fikret Yılmaz
- Bhuva B, Giovarruscio M, Rahim N, Bitter K, Mannocci F. “The restoration of root filled teeth: a review of the clinical literature” Int Endod J. 2021 Apr;54(4):509-535. doi: 10.1111/iej.13438. Epub 2021 Jan 5. PMID:33128279.
- Isufi A, Plotino G, Grande NM, Ioppolo P, Testarelli L, Bedini R, Al-Sudani D, Gambarini G. Fracture resistance of endodontically treated teeth restored with a bulkfill flowable material and a resin composite. Ann Stomatol (Roma). 2016 Jul 19;7(1-2):4-10. doi: 10.11138/ads/2016.7.1.004. PMID: 27486505; PMCID: PMC4955920.
- Shah EH, Shetty P, Aggarwal S, Sawant S, Shinde R, Bhol R. Effect of fibre-reinforced composite as a post-obturation restorative material on fracture resistance of endodontically treated teeth: A systematic review. Saudi Dent J. 2021 Nov;33(7):363-369. doi: 10.1016/j.sdentj.2021.07.006. Epub 2021 Jul 14. PMID: 34803275; PMCID: PMC8589613.
- Magne P, Kim TH, Cascione D, Donovan TE. Immediate dentin sealing improves bond strength of indirect restorations. J Prosthet Dent. 2005 Dec;94(6):511-9. doi: 10.1016/j.prosdent.2005.10.010. PMID: 16316797.
- Magne P. M-i-M for DME: matrix-in-a-matrix technique for deep margin elevation. J Prosthet Dent. 2021 Dec 25:S0022-3913(21)00655-7. doi: 10.1016/j.prosdent.2021.11.021. Epub ahead of print. PMID: 34961611.



