

Endo - Resto Relationship
24/06/2020
Marino Sutedjo
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
The predictors of success and failure in endodontically treated teeth depends on several factors: Apical Pathosis, Bacterial status of the canal prior to obturation, Extent and quality of the obturation and Quality of the coronal restoration, Torabinejad 2008(1). These need to be emphasised since majority of endodontically treated teeth have a badly compromised tooth structure at initial state. Good endodontic treatment only will not be enough to increase the survival rate these teeth. It need to be followed by good final coronal restoration. Salehrabi in 2004 (2) conducting an epidemiological study involving more then 1,4 million of endodontically treated teeth, it showed that good endodontic treatment with good final restoration will increase the survival rate to 97% in 8 years period. Inadequate endodontic treatment and coronal restoration can also increase incidence of apical periodontitis.
In this article I would like to discuss a case of endodontically treated tooth that both endo and resto aspect has not been adequately done and revision must be performed to increase the healing and survival rate of this endodontically treated tooth.

Fig. 1
This is a case of Mandibular first molar (46), patient was referred for revision and he came with chief complain of having a heavy pain while biting and also food impaction all the time on distal of tooth 46.
From clinical findings tooth 46:
- There was a PFM crown placed previously
- No sign of soft tissue lesion
- Tooth was tender to percussion and palpation
- Probing depth was normal.
From radiograph findings tooth 46:
- Endo-perio lesion was seen with the possible of endodontic origin.
- Unfitted crown margin placement on distal area
- Inadequate root canal treatment
- Fiber post placed previously on distobuccal root
In this type of cases, disassembly of everything is crucial. With disassembly we can answer some important questions like: is there any crack or fracture line? how many healthy dentin tooth structure left? is there any missing canals? All of these questions can help us to decide whether this tooth is still saveable or not, how we do our procedure and how we should put our final restoration.

Fig. 2
Upon removing PFM crown we can see immediately there were a lot of food impaction at the distal area due to unfitted margin of its coronal restoration.

Fig. 3
In this case, the removal of all previous restoration material is important. By removing it all we can inspect some of important things such as all the hidden caries that need to be removed, possibility of crack sign and missed canal and also remaining healthy tooth structure.
As you can see after removal of all previous restoration and caries we can see that fiber post have been placed in DB canal that need to be removed, loss of 2 marginal walls, no crack sign was visible, and possible of missed canal in mesial.

Fig. 4
Root canal retreatment was done, found 5 canals on this mandibular molar: 3 mesial canals (MB,MM and ML) where MM and ML are joining at the apical part and 2 distal canals.
All canals were shaped using VDW Rotate up to 25/.06, NaOCl 5,25% were used for irrigation and activation with EDDY sonic tip were performed for all canals.
Fiber post was removed from DB using ultrasonic tip. And looking from the anatomical configuration of the orifices, this mandibular molar is Radix Entomolaris

Fig. 5
After root canal obturation of all 5 canals using warm vertical condensation technique.

Fig. 6
DB canal was prepared for fiber post insertion. For post selection make sure that we don’t remove additional dentin from our root canal. Choose the size of the fiber post that suit our instrumentation (4). Before insertion of post, make sure the canal are cleaned and dried to have better bonding with the post. Magnification is needed to make sure.

Fig. 7
Post op radiograph #1, we need to confirm not just our endodontic retreatment result but also our restoration result.

Fig. 8
Post op radiograph #2, here we can see :
- All canals has been revised to the appropriate working length.
- Fiber post insertion reaching the correct depth and leaving no space between the post and gutta percha. This is quite important since the presence of a gap between the post and gutta percha can make a failure in the future (3).
- Marginal restoration area stop at the correct margin and leave no void area as well. This is to ensure that we can minimise the risk of coronal leakage.

Fig. 9
Post op radiograph #3, another different angle to check mesial canals, as we can see all 3 canals have been packed and sealed, and we can still see the marginal restoration also in the correct margin.

Fig. 10
Full coverage crown was immediately made. The distal margin of this tooth is pretty deep (subginggivally) and with the advantage of intra oral scanner we can determine our margin better directly after preparation.
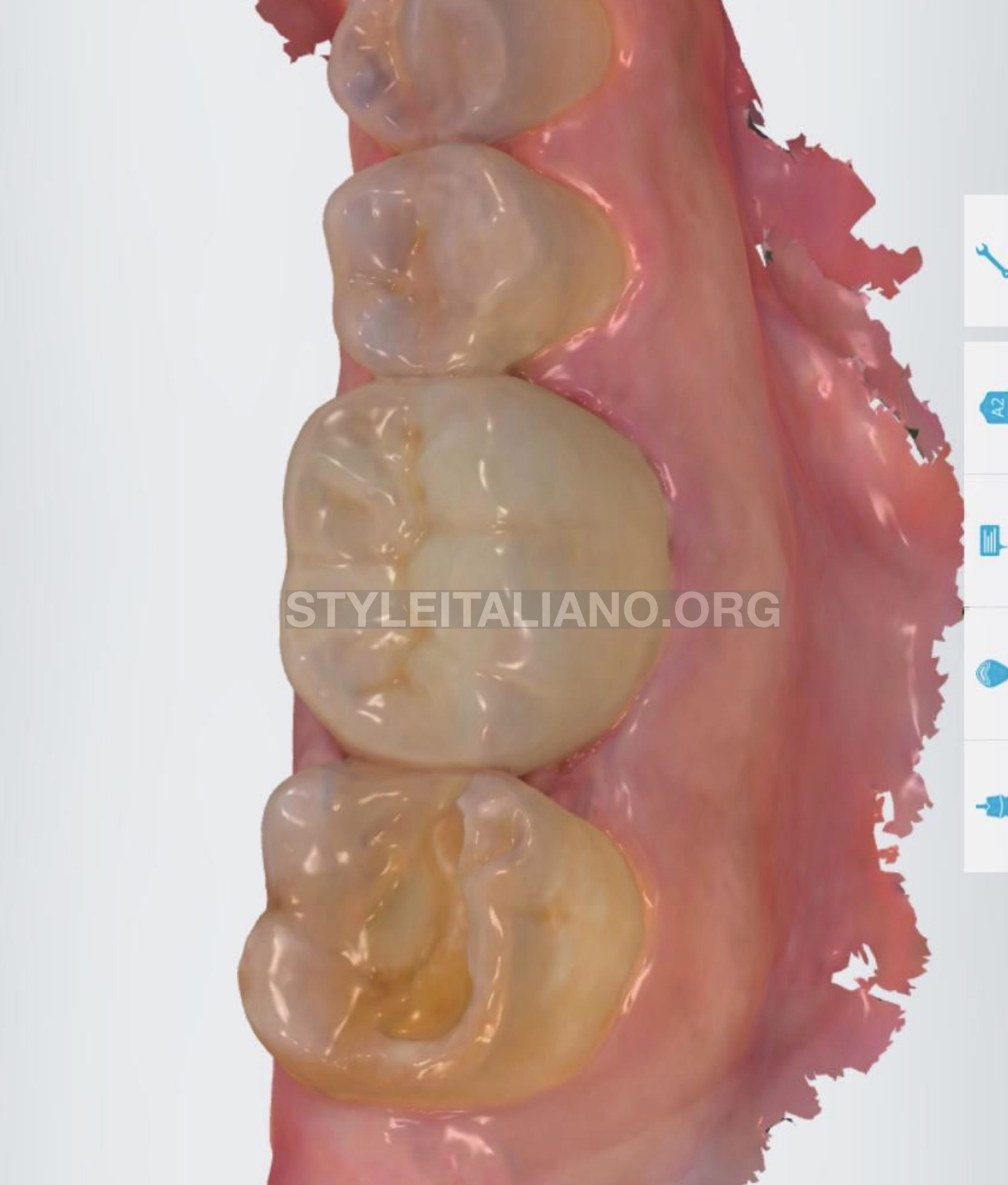
Fig. 11
After insertion of monolithic zirconia crown.

Fig. 12
Radiograph must be taken before cementation of new crown to make sure the marginal fit and proximal contact. Once it’s confirmed we can do our cementation.

Fig. 13
Final radiograph after crown insertion to check the adaptation of the crown both marginal and proximal contact.
Conclusions
The survival and success of endodontically treated teeth is not depend only from the endodontic aspect but also from the restoration aspect. When we need to perform primary endodontic treatment we need to think as well before we start the treatment, the restoration consideration and execute both well. As well as in endodontic retreatment, we need to address the restoration factors as one of the cause of failure. Removal of all restoration in retreatment cases is important as well as putting back the new coronal restoration. Always confirm and check both from clinical and radiograph evidence.
Bibliography
- Torabinejad M, Walton RE. Endodontics: Principles and Practice 4th Edition, 2008
- Salehrabi R, Rotstein I. Endodontic Treatment Outcomes in a Large Patient Population in the USA: An Epidemiological Study, Journal of Endodontic; 30: 864-850, 2004.
- Moshonov J, Slutzky-Goldberg I, Gottlieb A, et al. The Effect of The Distance Between Post and Residual Gutta-Percha on The Clinical Outcome of Endodontic Treatment, Journal of Endodontic; 31: 177-179, 2005
- Ree M, Schwartz R. The Endo-Restorative Interface: Current Concepts, Dental Clinics of North America; 54: 345-374, 2010


