
Endo-resto management of a poorly treated premolar
13/10/2022
Francesca Cerutti
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
The successful outcome of root canal treatment in teeth with non-infected vital pulps depends on preventing root canal infection, while in teeth with infected necrotic pulps it relies on eradication or at least reduction of bacterial counts to levels compatible with peri-radicular tissue healing.
To do so, the first thing to do is to carefully examine the pre-operative X-ray, in order to evaluate the anatomy of the tooth and have an idea about the number of roots and root canals, the degree of curvature of the canals and the presence of any obstacles. This can give the clinician a preliminary idea of the difficulty of the treatment and address one to the best treatment option.
On the other hand, anatomical knowledge is mandatory if one wants to execute a root canal therapy properly. Otherwise, failure is likely to occur.

Fig. 1
A young man came to my attention complaining about pain on the second upper right premolar. He had pain for three months, both while chewing and while drinking cold beverages. The dentist who did the root canal treatment said everything was fine with the tooth, so he waited for some time, then he was addressed to my office.
The pre-operative x-ray showed an enlargement of the periodontal ligament space, and suggested the presence of an untreated root canal.
The existing restoration did not ensure a perfect seal.

Fig. 2
I decided to retreat the tooth, in accordance with the patient, and I was able to get the pre-operative x-ray the colleague took.
In this case the presence of a second root canal is evident, so I have no doubt that the retreatment will improve the status of the tooth and will lead to an improvement of the symptoms referred by the patient.

Fig. 3
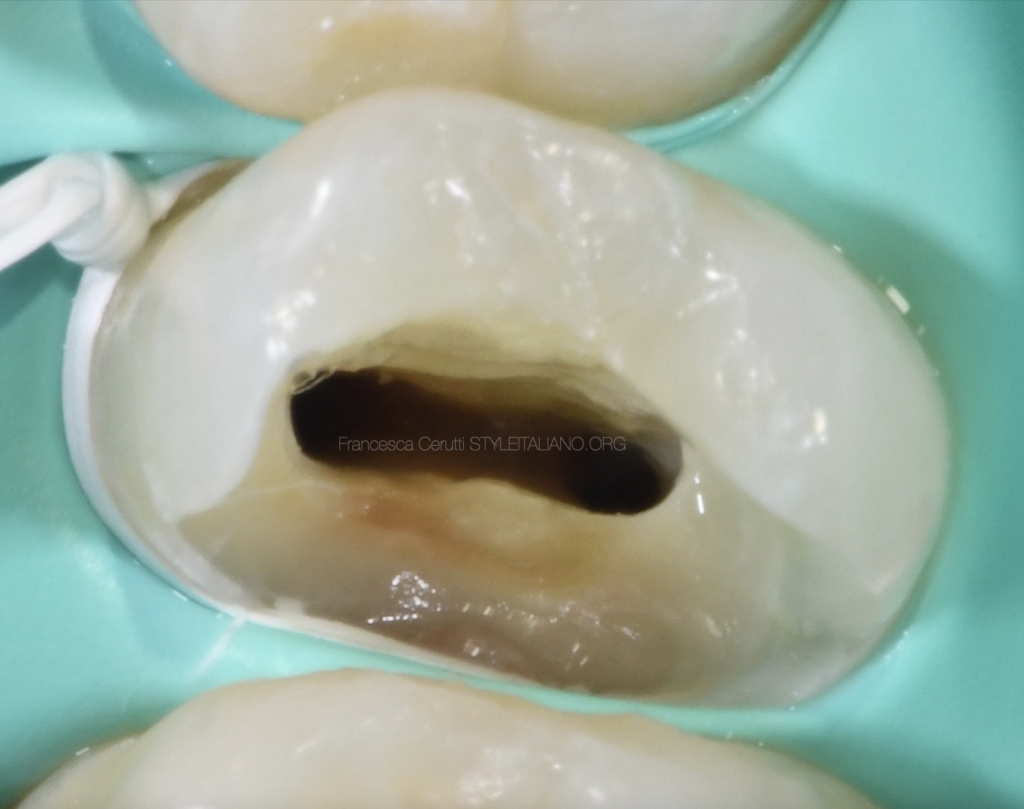
I wanted to do the endo-rstoratve treatment in a single session, so I did a multiple isolation in order to make the restorative procedures easier.
I completely removed the old restoration and I addressed the access cavity: The buccal canal only had been found and treated, but the position of the openings clearly suggests that there is another root canal, otherwise we would have found a single, central root canal opening.
I removed the existing gutta-percha with a rotary Ni-Ti file designer for retreatments, then I shaped both root canals.
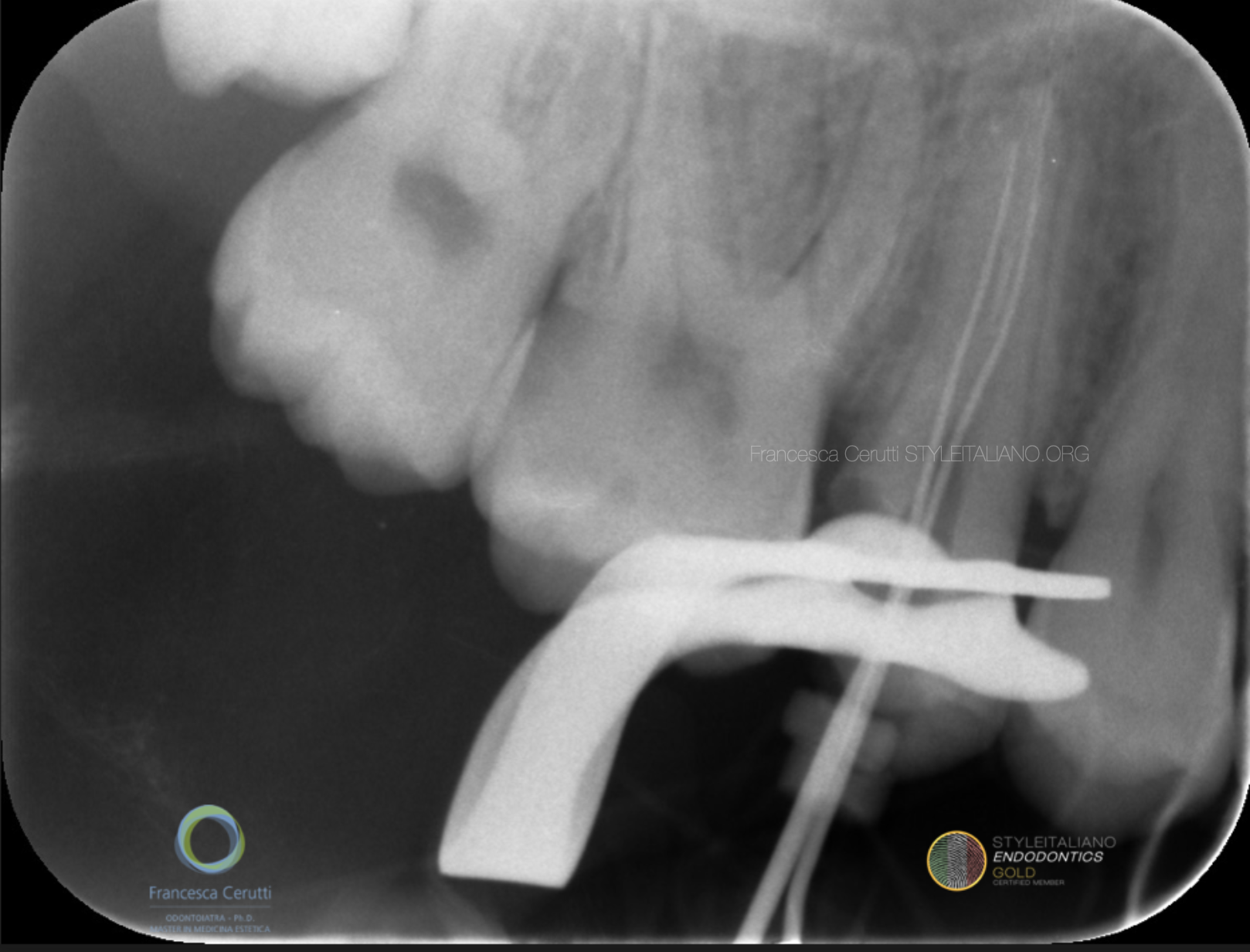
Fig. 4
The canals were straight, so it was not difficult to get to the working length in both of them, as shown by the intra operative x-ray.

Fig. 5
I shaped the root canals up to 040.06 and filled them with the warm vertical compaction of gutta-percha

Fig. 6
The tooth ready to be restored

Fig. 7
I etched and rinsed the enamel, then applied a self-etching primer on the dentine and a separated layer of bonding. Then, I applied a sectional matrix with a wooden wedge and a Garrison ring and put a thin layer of flowable composite to seal the access cavity.

Fig. 8
The restoration immediately after the removal of the rubber dam

Fig. 9
The post operative X-ray.
At the 1 week follow up, the patient referred the symptoms had completely disappeared.
Conclusions
The outcome of endodontic treatment can be seriously jeopardized by a lack of anatomical knowledge and a poor attention in the exam of the pre-operative x-ray.
The operator should try to pay attention to the elements that suggest the location of the root canals, both pre and intra operatively.
Bibliography
Azim AA, Griggs JA, Huang GT. The Tennessee study: factors affecting treatment outcome and healing time following nonsurgical root canal treatment. Int Endod J. 2016;49(1):6-16.
Basmadjian-Charles CL, Farge P, Bourgeois DM, Lebrun T. Factors influencing the long-term results of endodontic treatment: a review of the literature. International dental journal. 2002;52(2):81-6.
Bernstein SD, Horowitz AJ, Man M, Wu H, Foran D, Vena DA, et al. Outcomes of endodontic therapy in general practice: a study by the Practitioners Engaged in Applied Research and Learning Network. J Am Dent Assoc. 2012;143(5):478-87.
Burry JC, Stover S, Eichmiller F, Bhagavatula P. Outcomes of Primary Endodontic Therapy Provided by Endodontic Specialists Compared with Other Providers. J Endod. 2016;42(5):702-5.



