Endodontic retreatment of a maxillary second premolar with multiple shortcomings.
10/12/2020
Garima Poddar
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Knowledge of the root canal morphology and location of canals is important in a root canal treatment. Inability to locate and treat all the canals could lead to failure of a root canal treatment. For this purpose, first of all knowing the usual anatomies of all teeth and then their variations proves to be helpful. A proper access cavity preparation is very important in localizing the orifices of the root canals of that particular tooth being treated.
Goals of a root canal treatment is to clean, shape and disinfect the root canal system properly till desired working length and then obturate and seal them satisfactorily, both apically as well was coronally, for preventing entry of microbes in future in the treated teeth. Complications like creation of a ledge, prevents cleaning, shaping and obturation of canals till desired working length.
There are many retreatment case reports available in literature to understand the clinical impact of missed anatomy. Many a times the reason for failure of an endodontic therapy is a missed canal.
This article presents a case report of re-root canal treatment of tooth number 15 with missed anatomy, under obturation and some other complications which lead to intermittent pain and discomfort in patient’s tooth.
Case Report-
Patient information –
Age- 60
Gender- Female
Medical history- Non contributory.
Tooth identification- Maxillary right second premolar (tooth 15)
Chief complaint-
Patient complained of intermittent pain and discomfort in maxillary right posterior region since 1 month of reporting to a dentist who referred the patient to us. She gave history of rct being done 5 months back. Pain was intermittent and showed slight tenderness to percussion. Patient also complained of fractured restoration in association with tooth number 15.
Diagnosis- Pulpal – previously treated. ( inadequate treatment).
Peri apical – Chronic apical periodontitis.
Preliminary procedures:
- Local anesthesia- 2% lignocaine with adrenaline injection, was infiltrated buccally using a 30- gauge needle.
- Rubber dam isolation- tooth number15 was isolated using rubber dam isolation.
- Magnification- The treatment was performed under magnification. A dental operating microscope was used throughout the procedure.

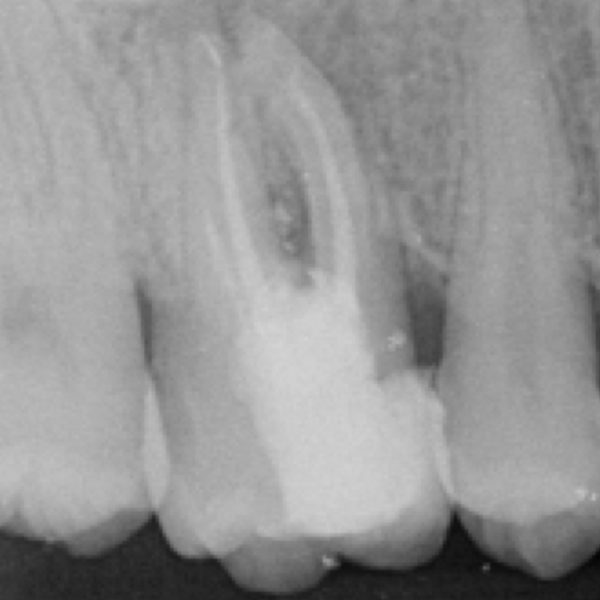
Fig. 1
The pre operative radiograph revealed the following –
1. Missed palatal canal.
2. Buccal canal with very short obturation ( only till the middle third of the canal).
3. Fractured restoration associated with the tooth.
4. Suspected ledge in buccal canal.

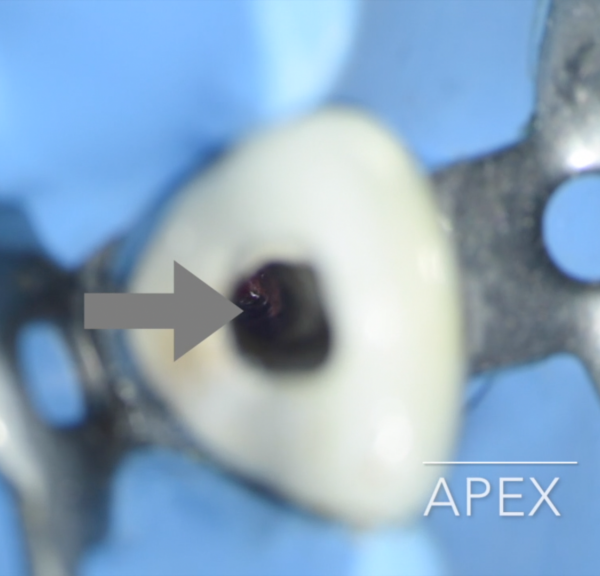
Fig. 2
The tooth was isolated & old restorative material was removed.
It was noted, that due to under extension of access cavity palatally, the canal was missed by previous operator.
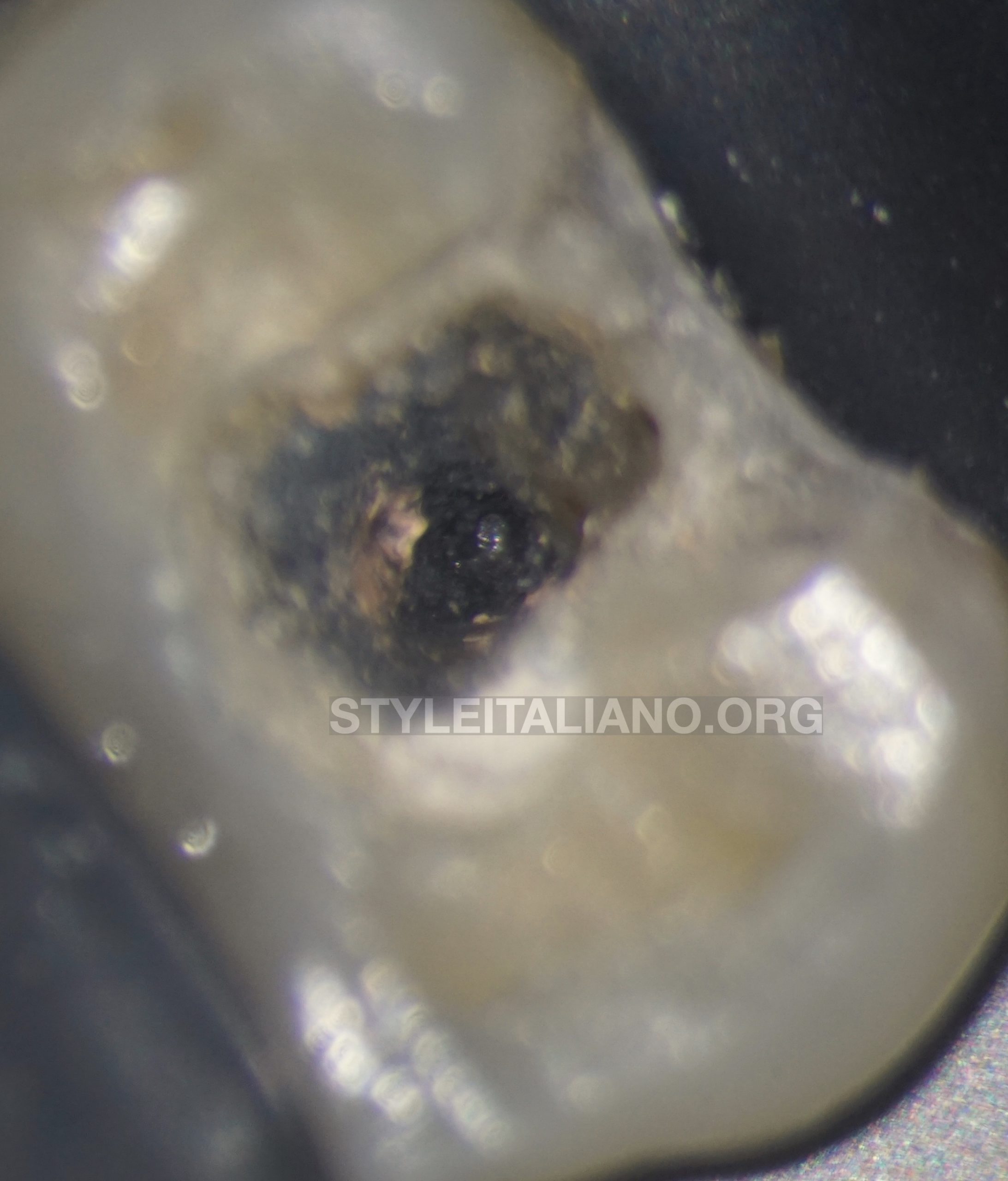
Fig. 3
Old obturation material was removed from the canal, with the help of H files and rotary files used at a high speed.
A ledge was found in buccal canal at the point where previous obturation material had ended. It was bypassed with 10 number k file used in picking motion.
Throughout the process, the canal was irrigated well with sodium hypochlorite after withdrawal of file from the canal each time.

Fig. 4
Access cavity was extended palatally. Palatal canal was found and negotiated with k file.

Fig. 5
Both the canals were negotiated till proper working length.
The working length was determined using an electronic apex locator and was confirmed on a radiograph.

Fig. 6
Coronal flaring was done and glide path was properly established.
The canals were shaped till 25-06% size till the working length.

Fig. 7
Thorough irrigation protocol was followed throughout the procedure which was as follows –
During shaping-
- 5.25% NaOCl used after each file use
After shaping –
- 5.25% NaOCl was introduced in the canal. It was heated within the canal using the down pack tip of obturation device and then was ultrasonically activated using Endo Ultra. This sequence was repeated 5 times per canal.
- Distilled water was used to flush the canals.
- Canals were then irrigated with Bioakt and the solution was activated ultrasonically.
- Canals were once more rinsed with distilled water.
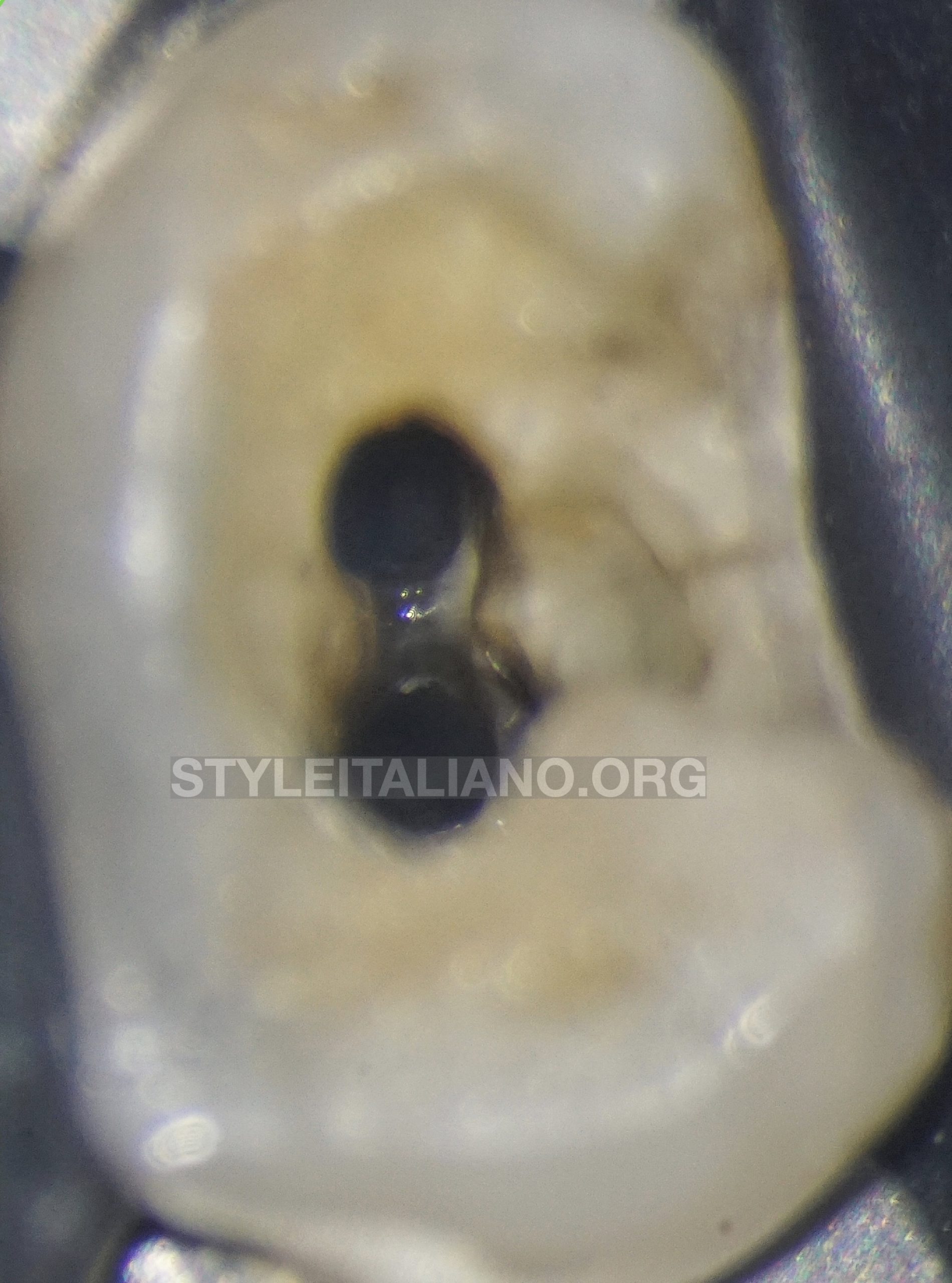
Fig. 8
Microscopic image of shaped and cleaned canals and isthmus area.

Fig. 9
The canals were then obturated using warm vertical compaction technique. The sealer used was AH plus.
Immediate post op – angulated view radiograph showed obturation of both the canals till the apex.

Fig. 10
Immediate post op – slightly angulated view.

Fig. 11
Post op x-ray image – straight angulation.
The patient was referred back to the referring dentist for post endodontic restorative work.

Fig. 12
Immediate post obturation image captured through a dental operative microscope.
Fig. 13
Three months follow up showed that patient was absolutely symptom free.
Conclusions
During a root canal treatment, understanding the root canal anatomy and usual location of canals is important in order to be able to locate them. Further, a good, undistorted pre-operative radiograph serves to be of high value in being able to locate all the canals. A proper access cavity preparation plays a vital role in localization of canals and also helps in their easy instrumentation. Using magnification also aids in proper visualization of the tooth structures and canals.
While bypassing a ledge, the key is to not apply force and irrigate well from time to time. Also while negotiating a ledge, understanding the possible reasons for its creation is important.
During a root canal treatment, as well during endodontic retreatment procedures, a good irrigation protocol and using a combination of irrigating solutions in order to achieve proper cleansing and disinfection of the root canal system is important.
Bibliography
- G Cantatore, E Berutti, A Castellucci. Missed anatomy: frequency and clinical impact. Endodontic Topics. 2009;15:3–31.
- Tabassum S, Khan FR. Failure of endodontic treatment: The usual suspects. Eur J Dent. 2016;10(1):144-147. doi:10.4103/1305-7456.175682
- Song M, Kim HC, Lee W, Kim E. Analysis of the cause of failure in nonsurgical endodontic treatment by microscopic inspection during endodontic microsurgery. J Endod. 2011;37:1516–9.
- Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol. 1984;58(5):589–99.
- Mohammadi Z, Asgary S, Shalavi S, V Abbott P. A Clinical Update on the Different Methods to Decrease the Occurrence of Missed Root Canals. Iran Endod J. 2016;11(3):208-213. doi:10.7508/iej.2016.03.012