Dealing with root filling residuals in root canal re-treatment
27/07/2023
Ahmed Alwaidh
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Non-surgical root canal re-treatment is one of the most dental procedures that practitioners face in routine daily work. Though, it remains one of the most challenging procedures, as we are dealing with root canal complexities, different root filling materials, and most importantly, infection.

Fig. 1
Clinically, LR6 has defective restorations, negative to cold test (compared to adjacent teeth which responded normally), mild tenderness to percussion, normal probing.
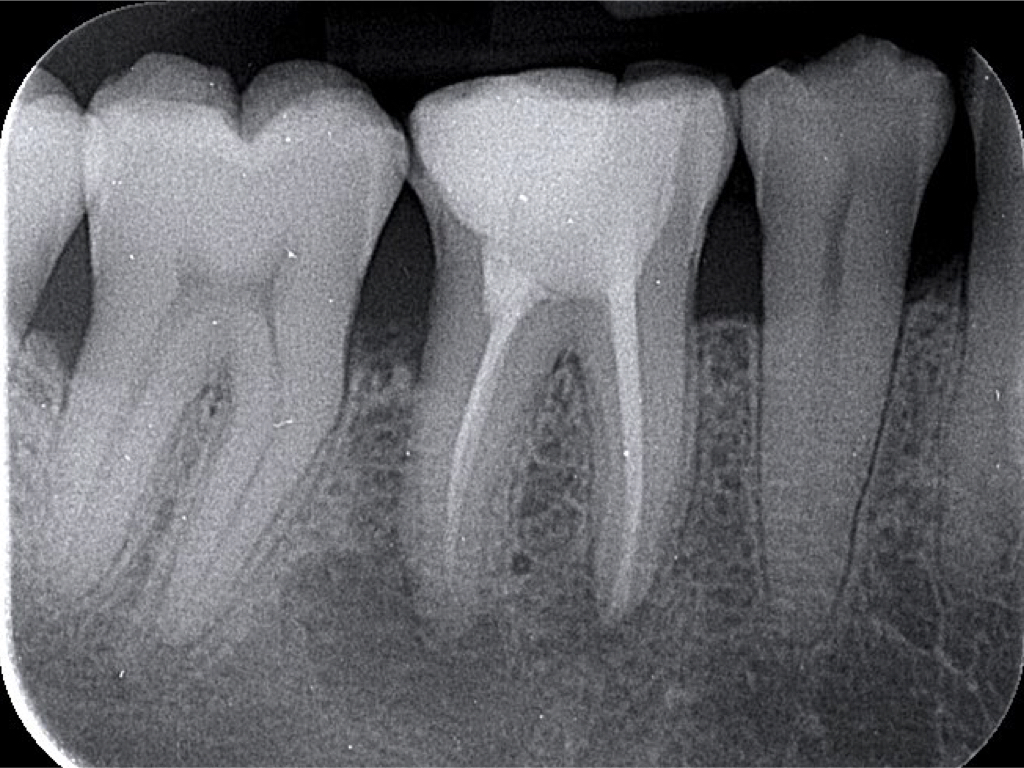
Fig. 2
Radiograph: IOPA revealed large PA radiolucencies around apices of LR6.
Diagnosis: LR6 previously treated and symptomatic apical periodontitis.
Treatment plan: Non-surgical root canal re-treatment for LR6.

Fig. 3
After removing old restorations, different filling materials were evident in the distal orifice.
Retreatment for all canals was done easily using F One file #25/06 (Fanta Dental, Shanghai, China) to full working length, with the aid of endomotor with integrated apex locator, without any solvent.
Many remnants of root canal filling sustained in the root canal system. I was able to remove majority of them with rotary file debridement, lots of sonic and ultrasonic activation.
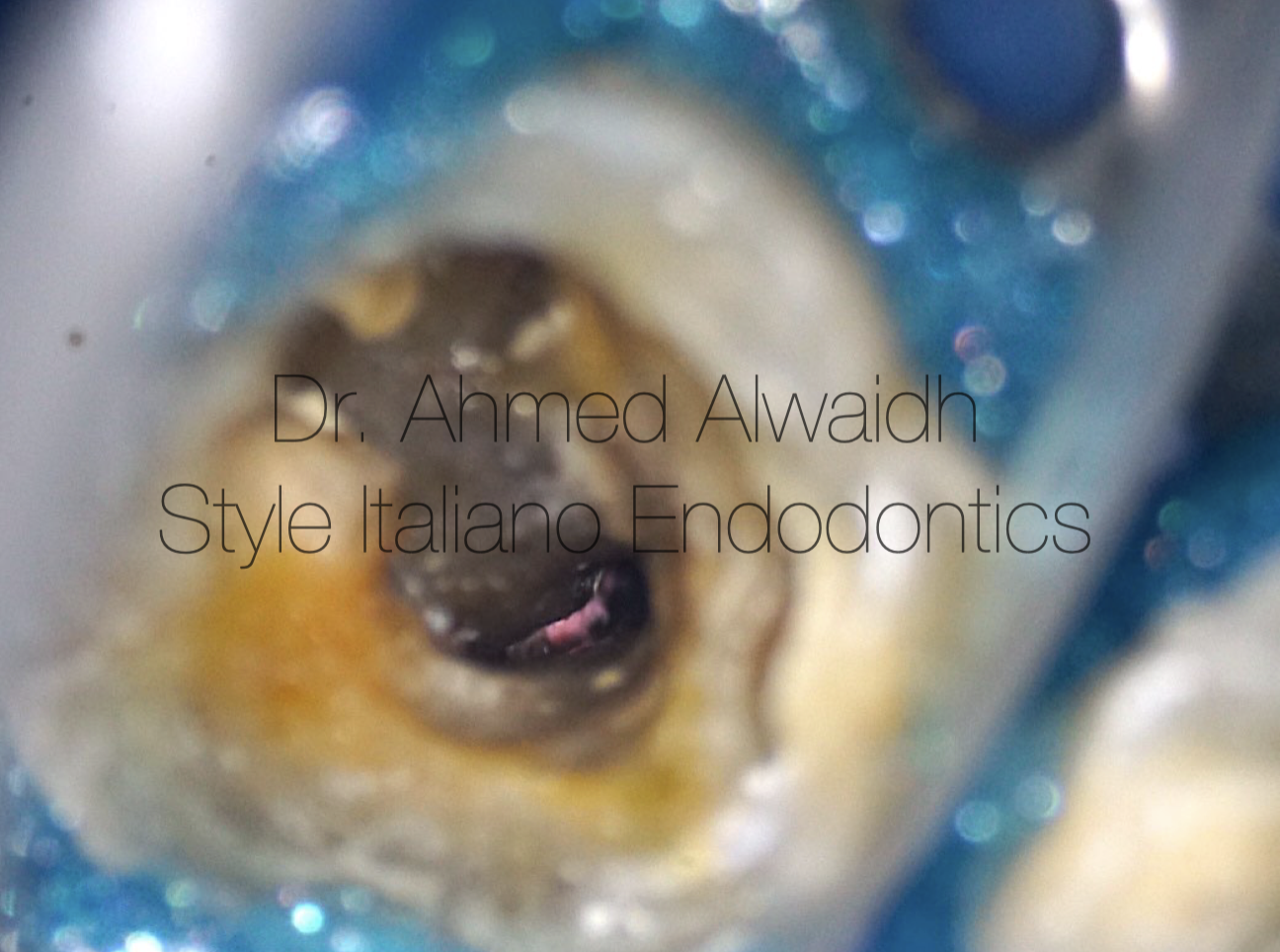
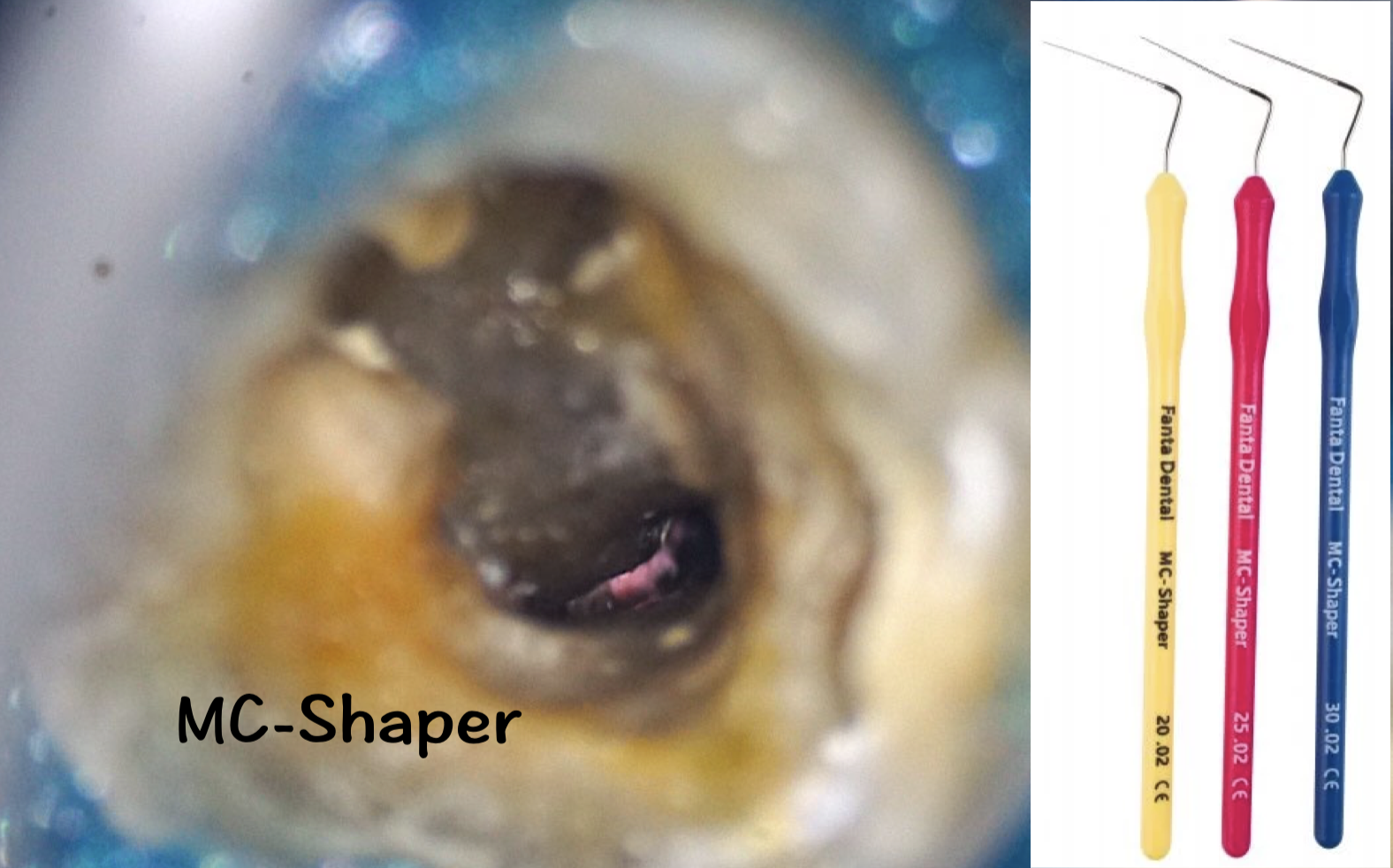
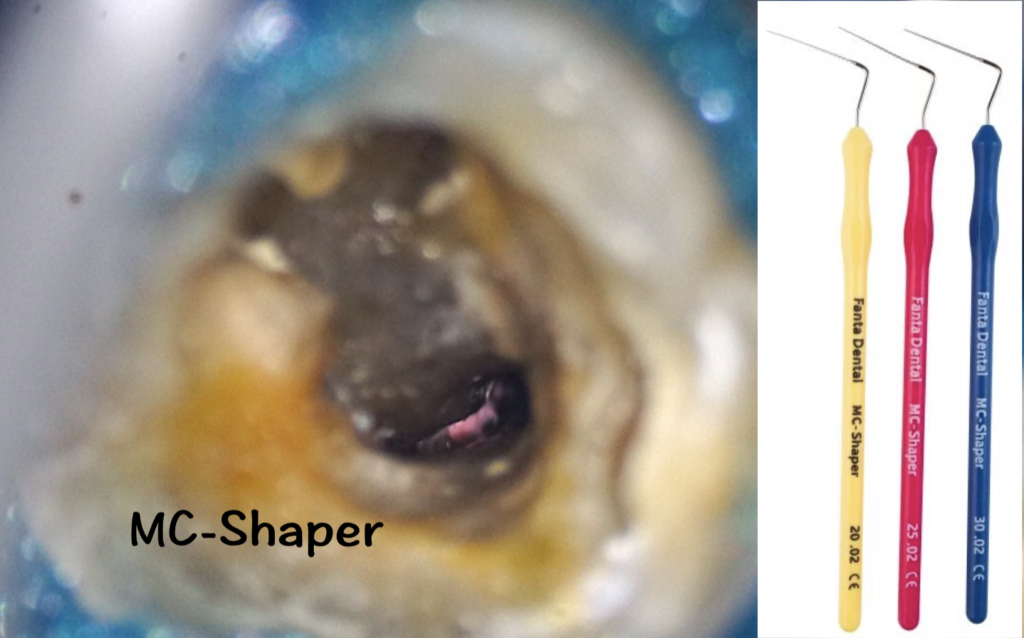
Fig. 4
Few remnants sustained even with many efforts
Debridement of root canal walls and removing residual root filling materials by MC-Shaper (Fanta Dental, Shanghai, China).
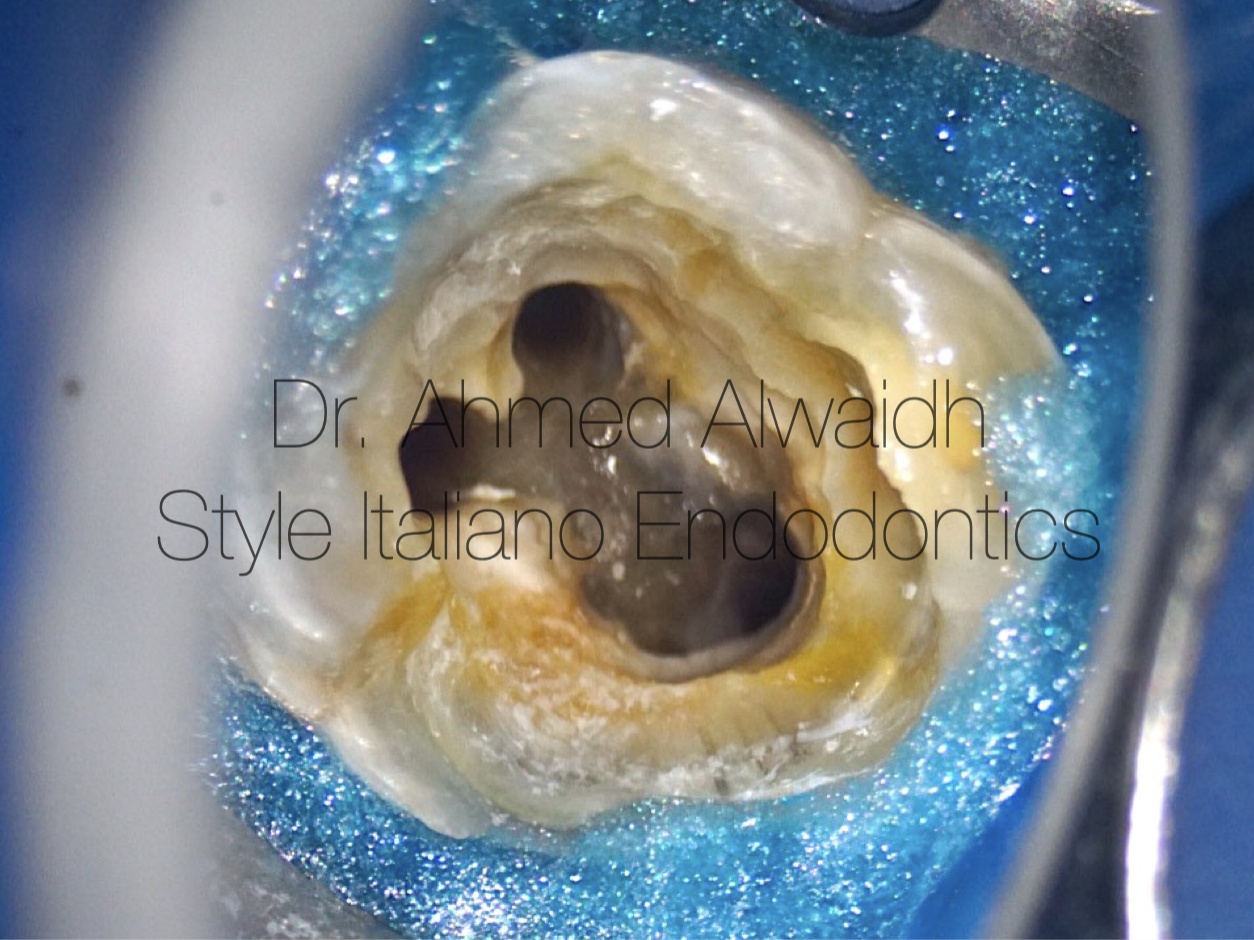
Fig. 5
LR6 is now ready for obturation.
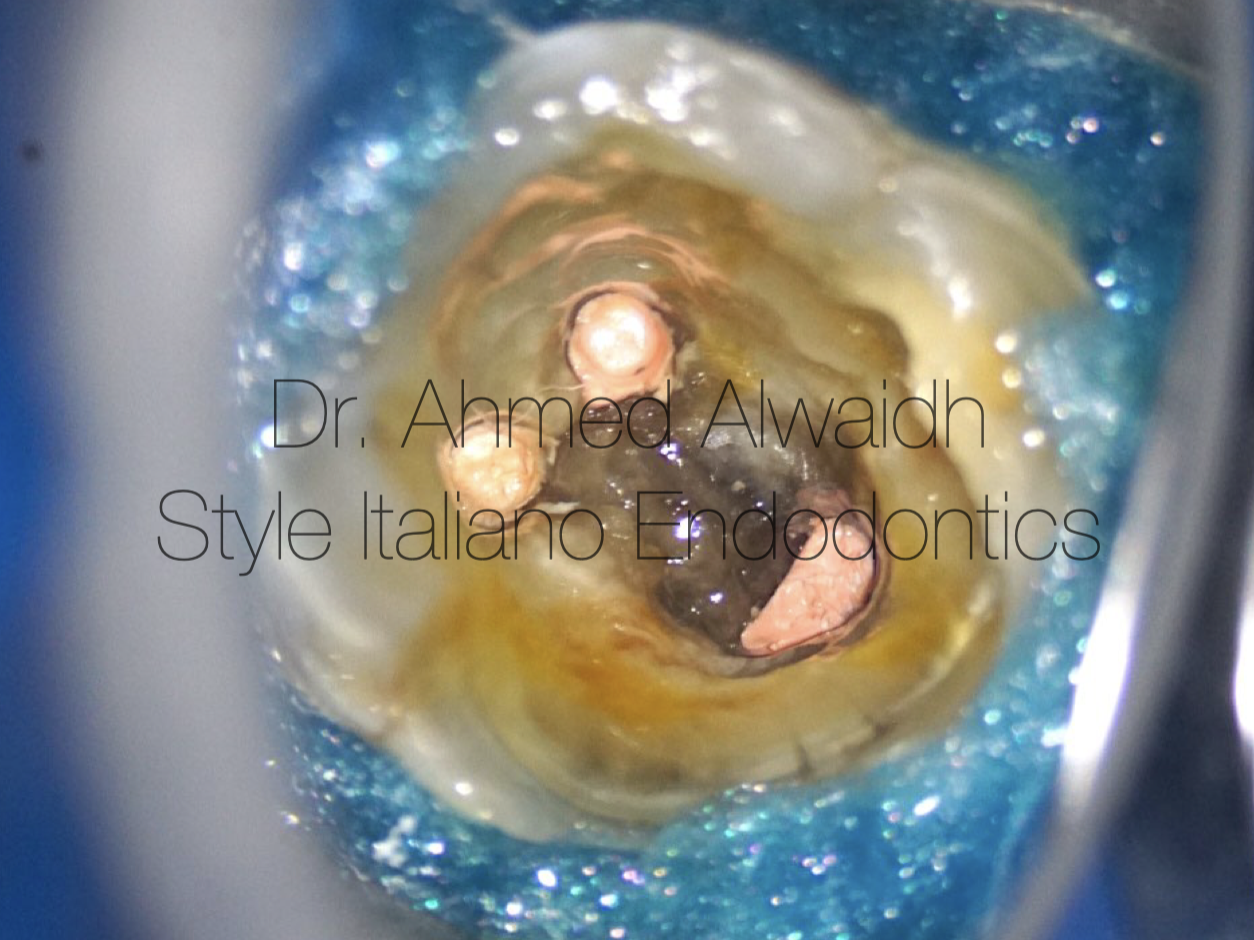
Fig. 6
Hydraulic obturation with premixed bioceramic cement. Composite restoration after making the tooth out of occlusion, and been scheduled for indirect cusp coverage.

Fig. 7
Final IOPA
Conclusions
Root canal re-treatment is different from primary root canal treatment in terms of disinfection. Although the microorganisms are different, as the prevalence of E. faecalis in secondary Endodontic cases is higher than primary Endodontic cases (Stuart et al. 2006), but microorganism resistance in both conditions is mostly similar. However, gaining disinfection in secondary Endodontic treatment is more difficult, as the residue of previous root canal filling offers more protection for the biofilm from disinfectant solutions (Zehnder & Paque 2008). Generally speaking, all root canal system is having residual root filling materials after re-treatment, regardless of the system been used, size, movement, and even if larger sizes been used (Hülsmann & Stutz 1997, Hülsmann & Bluhm 2004, Marques Da Silva et al. 2012, Zulu et al. 2013).
MC-Shaper (Fanta Dental, Shanghai, China) is a very great asset especially in root canal re-treatment. It helps in debridement of root canal walls from existing root filling materials, especially in areas beyond visibility, thanks to its flexibility, stiffness and different range of sizes (#20, #25, #30).
Bibliography
- Hülsmann M and Bluhm V (2004) Efficacy, cleaning ability and safety of different rotary NiTi instruments in root canal retreatment. International endodontic journal 37(7), 468-476.
- Hülsmann M and Stotz S (1997) Efficacy, cleaning ability and safety of different devices for gutta‐percha removal in root canal retreatment. International Endodontic Journal 30(4), 227-233.
- Marques da Silva B, Baratto‐Filho F, Leonardi D P, Henrique Borges A, Volpato L, Branco Barletta F (2012) Effectiveness of ProTaper, D‐RaCe, and Mtwo retreatment files with and without supplementary instruments in the removal of root canal filling material. International endodontic journal 45(10), 927-932.
- Stuart C H, Schwartz S A, Beeson T J, Owatz C B (2006) Enterococcus faecalis: its role in root canal treatment failure and current concepts in retreatment. Journal of endodontics 32(2), 93-98.
- Zehnder M & Paque F (2008) Disinfection of the root canal system during root canal re‐treatment. Endodontic Topics 19(1), 58-73.
- Zuolo A S, Mello Jr J E, Cunha R S, Zuolo M L, Bueno C E S (2013) Efficacy of reciprocating and rotary techniques for removing filling material during root canal retreatment. International Endodontic Journal 46(10), 947-953.