Management of a retreatment case (RADIX ENTOMOLARIS) with FANTA AF F ONE ESSENTIAL KIT
03/11/2020
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
A more reflecting practical definition of non surgical retreatment by Car was described as a procedure performed on teeth that received failed prior attempts at definitive root canal treatment, requiring further endodontic therapy to achieve a successful result.
Mishaps as missed canal, ledges, incomplete filling or even loss of coronal seal can lead to root canal treatment failure.
Incomplete Treatment of the Root Canal System as when the working length stops short of the canal end, due to anatomical problems (curvature, bifurcations, etc.) or even preparation errors may lead to root canal treatment failure
Our main goal in non-surgical retreatment is to regain access to the periapical area of the treated tooth.
This case report shows previously failed root canal treatment with missed anatomy to be disinfected, inadequate obturation, loss of coronal seal and missed extra distal root (RADIX ENTOMOLARIS)
Radix entomolaris is frequently seen in caucasians and africans by the range of lkess than 5% more frequently seen in mongoloid traits (like Chinese, Inuit, and Native Americans), by the ranges from 5% to >30%.

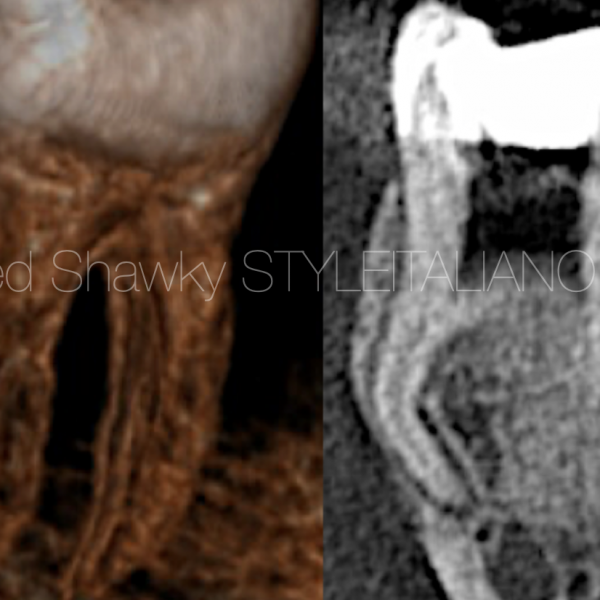
Fig. 1
A 40 years old male patient came to my clinic with lower first molar complaining of swelling with pain on biting
Upon clinical examination the molar is tender to percussion and old amalgam restoration with intraoral swelling associated with sinus and pus draining through a draining fistula
The radiographic preoperatively showed
- Short obturation
- Periapical radiolucency
- Missed canal anatomy
- Suspected another distal root (radix entomolaris)
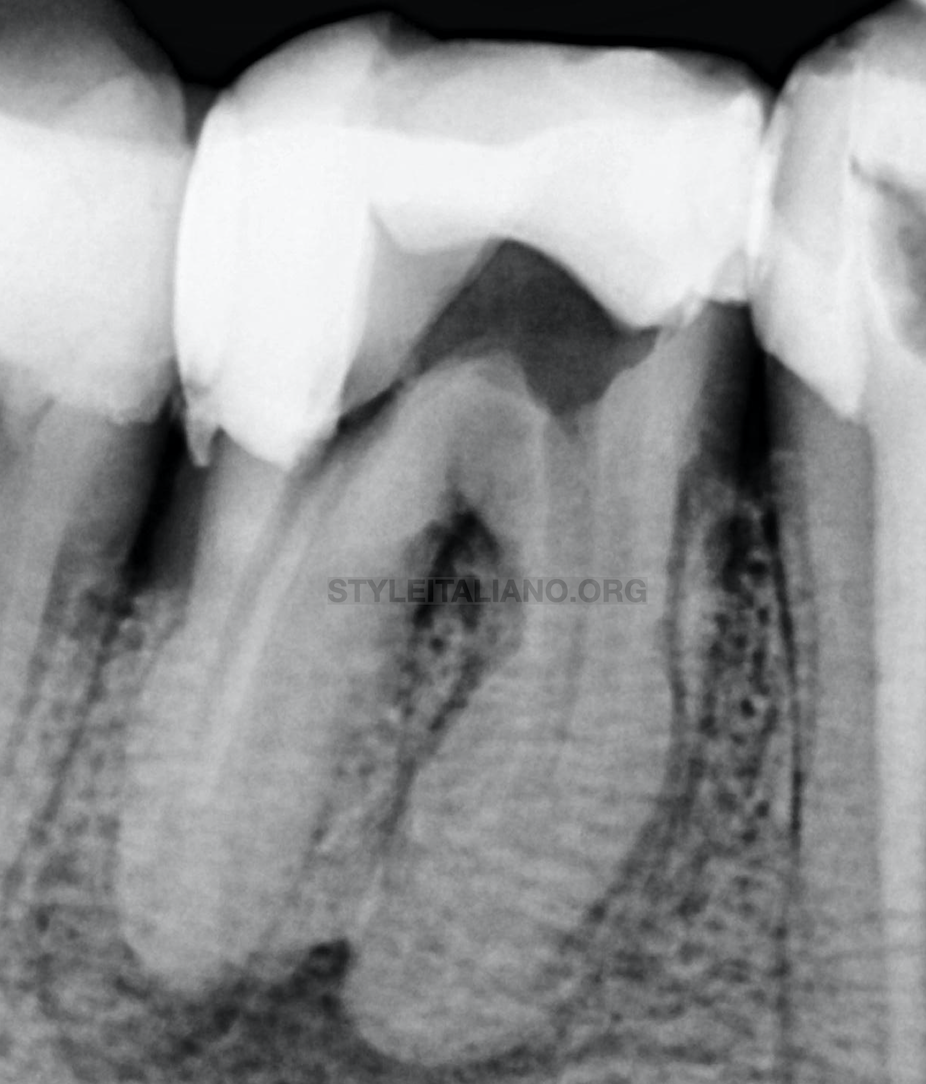
Fig. 2
- Local anesthesia was administered and rubber dam was applied.Previous amalgam restoration was removed with high-speed burs and endodontic ultrasonic tips were used to gain entry into the pulp chamber and location existing gutta percha and extra orifices.Access cavity to have straifght line access to the canals was done with round and safe-end tapered fissure bur.Composite build up was done with composite restoration.

Fig. 3
Removal of gutta percha was started by using step down technique starting by 25 6% then 20 4%

Fig. 4
Once gutta percha removed, I started my glide path journey with the great new innovative fanta path file 13 3% to the apex using electronic apex locator then flaring the 4 canals by the great sequence of the fanta essential kit 20 4%, 25 6% then 35 4%.
During cleaning and shaping, the root canals were irrigated with copious amounts of 5% sodium hypochlorite solution.
Intracanal medication of calcium hydroxide was then used and access sealed with temporary filling.
After one week master cone check up done

Fig. 5
Obturation was done with bioceramic sealer and the root canal filling was evaluated radiographically

Fig. 6
post operative x-ray with distal shift
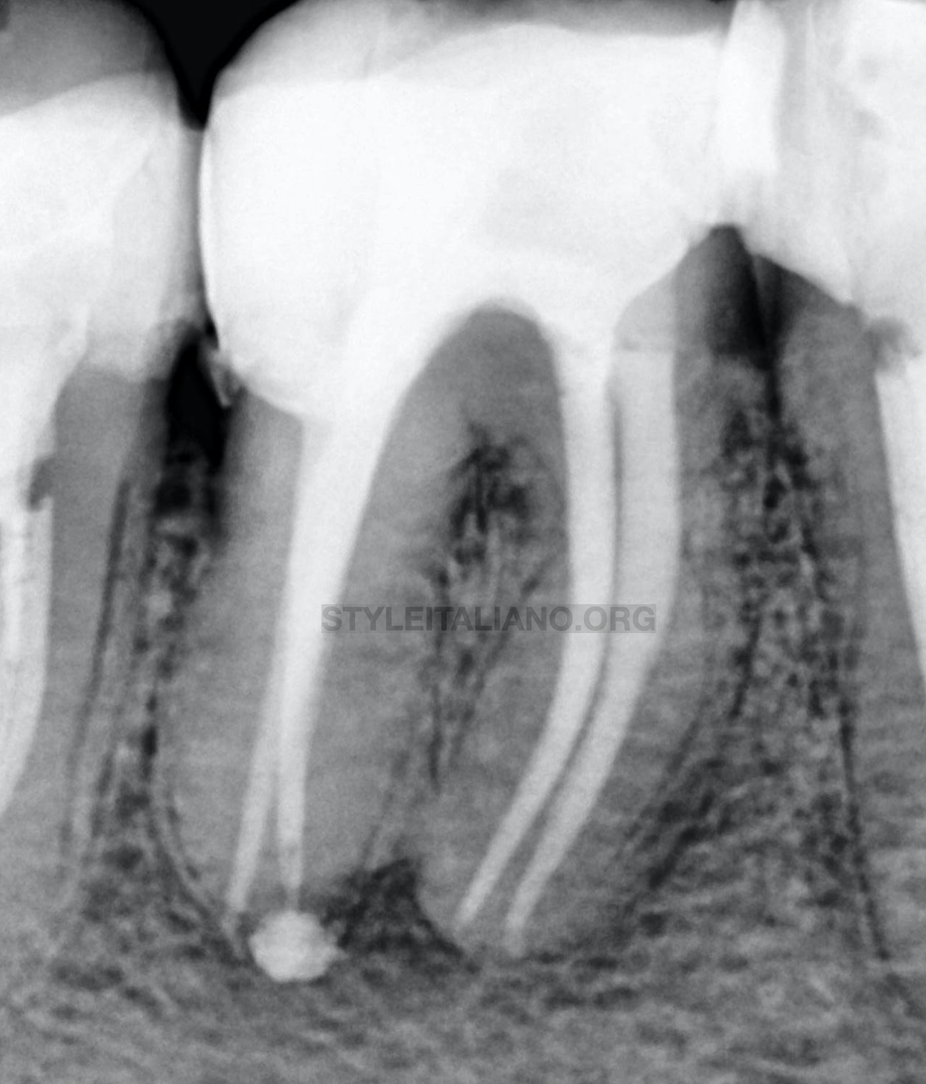
Fig. 7
Follow up a three months follow up shows signs of good healing in the periapical area
Conclusions
The article is to focus on certain guidelines that may help in radix entomolaris cases
- Access cavity maybe modified a lkittle bit to be trapezoidal in shape to gain straight line access to decrease the incidence of mishaps during work in such cases
- The reader should make a good preoperative analysis radiographically of the case with different angulations to confirm RE.
- Sufficient coronal preflaring and glide path creation will decrease the incidence of problems in the apical third during shaping of the canals
- Flat side design of the new fanta files improves resistance to flexural fatigue due to the major flexibility reached giving more space for the debris and previous gutta percha in retreatment cases to be removed coronally more frequently
- Most of root canal failure of cases with RE is due to missed canal because of the overlapping of the radix root over the mesial or dital root in the radiographs
- Length of the RE differs from a few millimeters to equal length of the mesial and distal other roots so electronic apex locator during working length determination step is a must.
Bibliography
1. Carabelli G. Systematisches Handbuch der Zahnheikunde. 2nd ed. Vienna: Braumuller and Seidel; 1844. p. 114.
2. Curzon ME. Three-rooted mandibular permanent molars in English Caucasians. J Dent Res. 1973;52:181.
3. Sperber GH, Moreau JL. Study of the number of roots and canals in Senegalese first permanent mandibular molars. Int Endod J. 1998;31:117–22.
4. Yew SC, Chan K. A retrospective study of endodontically treated mandibular first molars in a Chinese population. J Endod. 1993;19:471–3.
5. Curzon ME, Curzon JA. Three-rooted mandibular molars in the Keewatin Eskimo. J Can Dent Assoc (Tor) 1971;37:71–2.