

Challenges with retreatment of Russian red aka Resorcinol-formaldehyde teeth
18/09/2023
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Retreatment is a complex, difficult and cautionary challenge. Material previously placed in the canals may be difficult to dislodge, visualize, follow and evacuate and when added to the complex anatomy of the canals, this challenge may result in failure of the retreatment. Years ago, when resorcinol formalin was used to deal with difficult and complex anatomy, the material used was often not amenable to retreatment. This was due to the addition of 10% sodium hydroxide to the material, which ensured the polymerization of the material in the canal, thanks to which the canal was resinified, and if this reaction was successful, the resulting material remained stronger than rock in the canal. The resorcinol formalin method has been used since the 1960s, the method included different types of mixing techniques and was used according to the clinical situation. It took several steps and visits to perform the method.
Resorcinol-formaldehyde contains two potentially toxic components, formaldehyde (liquid) and resorcinol (powder). 10% sodium hydroxide is added to the mixture that will promote polymerization. In some cases, material was soft “sap-like” or gel consistency, while in others hard as a brick and hard to recognize visually the material out of dentin. Also known as "Russian red" was very popular treatment method in Russia and other post-soviet countries as well as in Eastern Europe, China and many more countries. Name "Russian red" comes from tooth discoloration properties of the material which changes tooth color to red. With increasing immigration statistics, you can find those treated with "Russian red" all over the world.
Usually, resorcinol formaldehyde was used in molars with complex anatomy, and complete canal treatment was not possible. You will often encounter material before the first curvature, with ledge or broken instruments. RF teeth are usually retreated few times maybe without success or even with added problems like perforations or filed with Gutta-percha until the ledge.
Fig. 1
Recognizable change in color from pink to dark red or burgundy and darker is the sign of RF therapy. But its always a mystery what type of retreatment is on your way, easy one or you will be dialing with impassable canal. An unpolymerized or partially polymerized gel is expected, in case of fully polymerized resin you have brick hard material which is very hard or even impossible to remove.
There is no solvent for Resorcin-Formaldehyde resin. In comparison with other solutions Sodium Hypochlorite shown better penetration but not dissolution properties when used in RF canals. In other studies, sonic and ultrasonic instrument shows effective removal of RF from canals.
X-ray can show hollow space of root canals filled with radiolucent paste , or you can find some radiopaque material inside the canal.
Variations in mixing and techniques gives unique presentation of materials in every case and sometimes in each canal for same tooth.

Fig. 2
Referral patient, 42-year-old women with pain on biting. Tooth previously treated with RF, you can find gel like material in mesial , broken instrument right before curvature, in distal gutta-percha was presented till the ledge.
Treatment was done in two sessions under the operative microscope.

Fig. 3
Coronal part of mesial canals were rinsed with NaOCl 5,25% and ultrasound to clean from paste, broken lentulo spiral was lessened and retrieved with ultrasound, while managing the ledge took an hour with pre-curved C files. Change in canal direction was determined on CBCT and managed in very couscous way not to straighten or perforate canal wall.
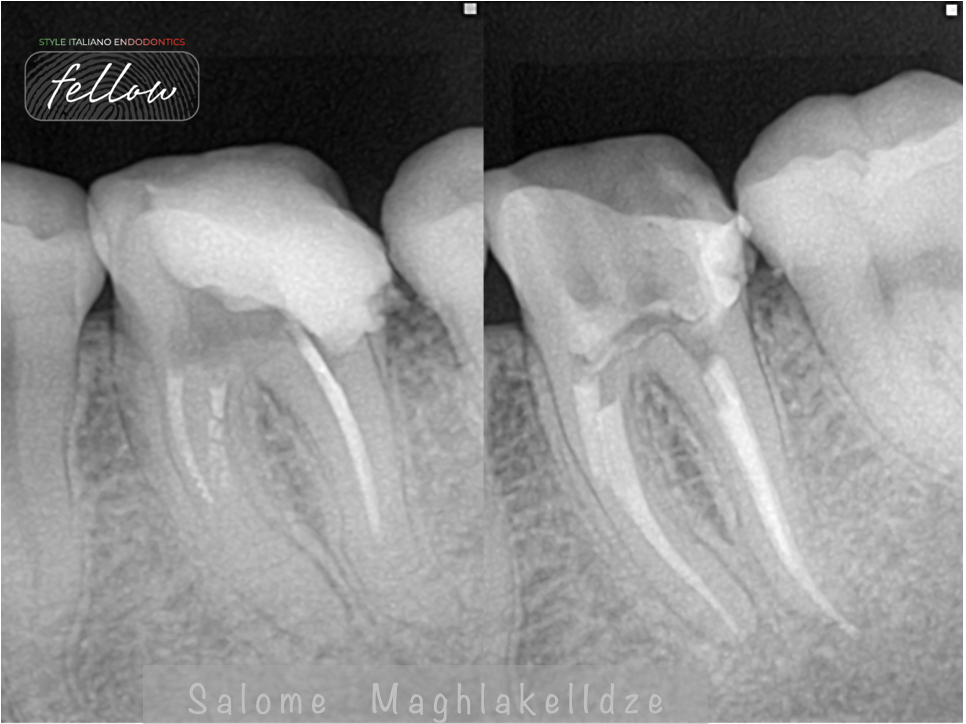
Fig. 4
Distal canal was filed with gutta-percha which was removed with rotary instruments. Ledge menagment was done with pre-curved instruments size #8 and #10 , shaping was finished with rotary instruments. Irrigation protocol was NaOCl 5,25 % activated with ultrasound , finished with 17% EDTA activated for 1 min. Obturation was done with AH plus and CWC.
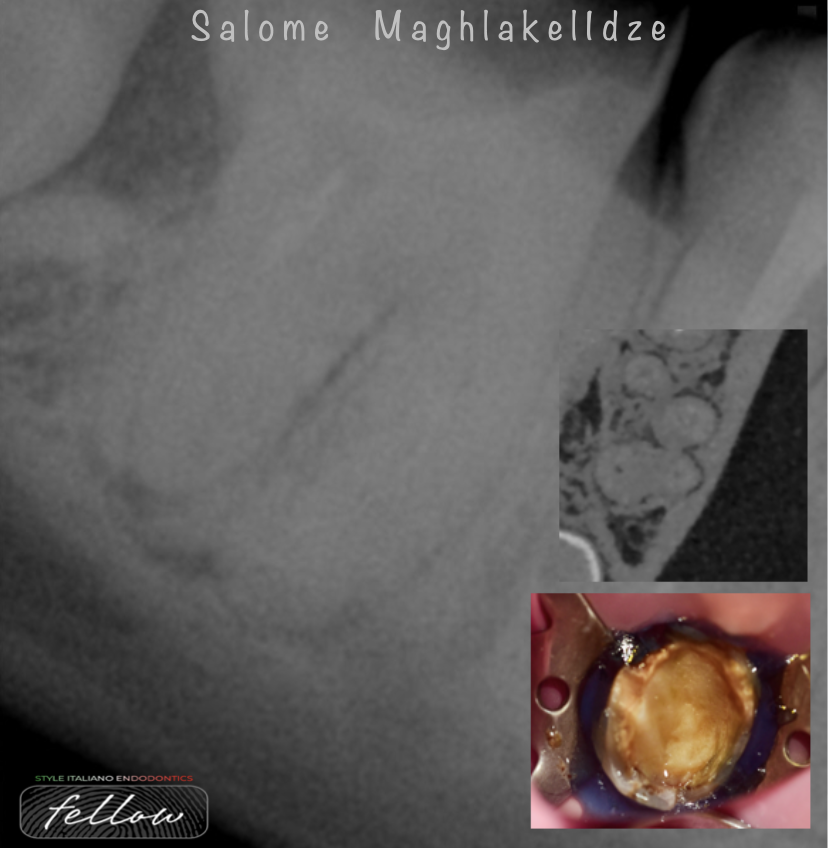
Fig. 5
Referral case 45-year-old women with previously initiated retreatment on 46 tooth. Doctor couldn't negotiate canals. CBCT was used to understand tooth complex anatomy and evaluated the curvatures. Material was barely visible under the microscope it was presented as a hard glossy colorless substance. entrance into canal was modified and negotiated with rotary instruments, middle part was scouted with bended file #10.
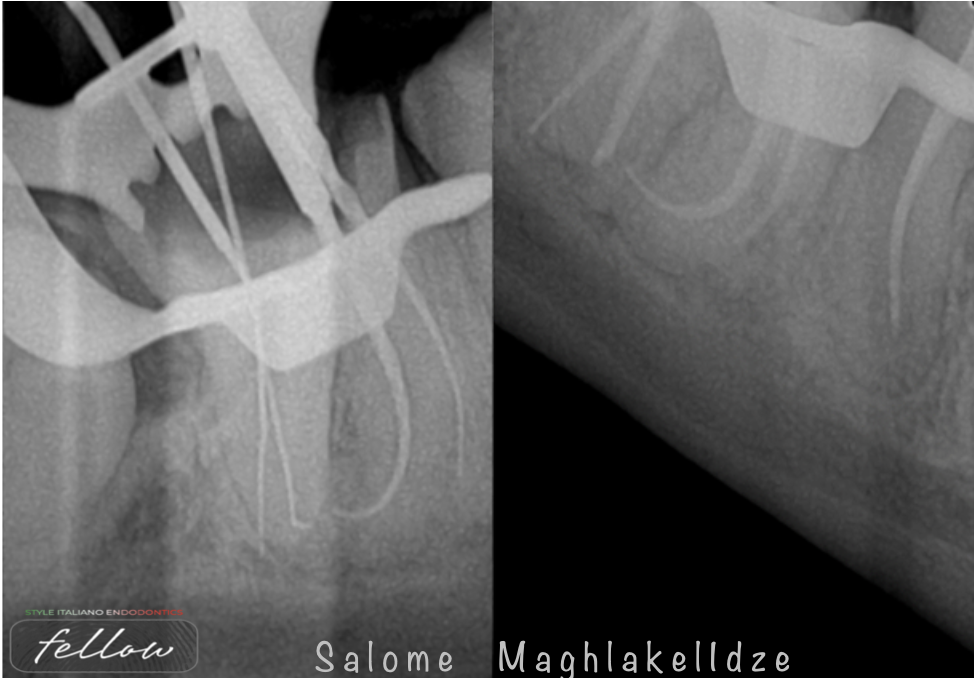
Fig. 6
Dentinal walls were shiny and not easy to cut due to changes in dentinal structure, it seams like instruments were sliding in canal without cutting it. Working length was determined by apex locator and a heat treated rotary file was used to mechanically clean canals. Copious irrigation and activation was done with NaOCl and EDTA 17 %. Canals were closed with heat compatible Bioceramic sealer and Warm Vertical Compaction.

Fig. 7
Referral case with initiated treatment on tooth 26. Canals were filed with gel like material till curvature. Palatal canal was not “filed” at all based on X-ray , material in Palatal canal was radiolucent, not having any specific color and was resembling very much dentinal structure.
Ultrasound was used to regain the path in palatal canal from the beginning, after hand pre-curved files were introduced until patency was achieved and right after rotary instruments were used for finishing canal shaping.
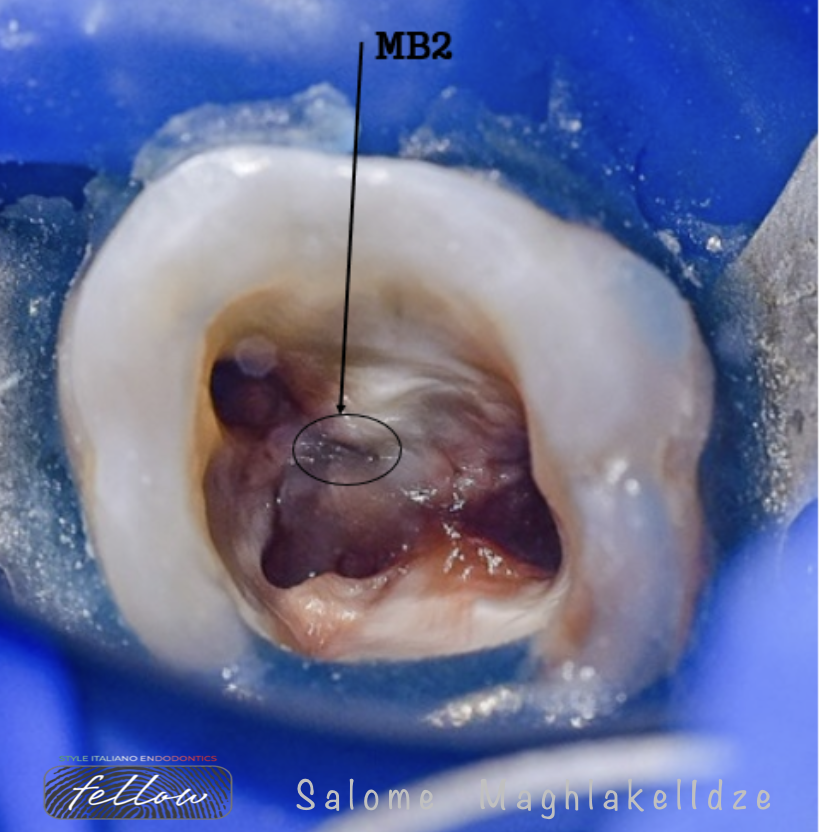
Fig. 8
After finishing all three canals MB2 was prepared. Ultrasound tip was used to clear MB2 area to take off overlying dentinal shelf. MB2 was merging with MB1.

Fig. 9
Canal was obturated with heat compatible Bioceramics and Warm vertical compaction technique.

Fig. 10
About the author: Salome Maghlakelidze
2010: Graduated in dentistry from Tbilisi State Medical University
2011: Residency program in Therapeutic Dentistry
2012: Advances Course in Dentistry at the National Medical Academy of Post-Graduate Education named after P.L. Shupyk
Started the PhD program in Tbilisi State University
Lecturer at New Vision University
Trainer in International Dental Educational Academy
Fellow Member of Style Italiano Endodontics
Opinion Leader for Zarc4Endo
From 2022 President of Georgian Endodontic Association
Focusing on Endodontic in Evergreen Dental Center
Conclusions
RF treated teeth are challenge for dentists in many ways. You can find unpredictable and different scenarios from easy to hard in each RF treated teeth. Armamentarium is very important in cases with RF, machine-driven instruments and ultrasound should be used with caution, while it is valuable tool in retreatments, studies shows that RF teeth can be more fragile, and cracks can be result of ultrasound usage more than in case with machine-driven instruments. While this studies can be questionable, there is also risk of ledges and perforations without proper knowledge and magnification. Last but not least with the knowledge and instruments patience and diligence and determination is also required.
Bibliography
1.Retreatments - Solutions for periapical diseases of endodontic origin- Book by Style Italiano Endodontics
2. Resorcinol-Formaldehyde Resin “Russian Red” Endodontic Therapy Nathan W. Schwandt, DDS, and Tom G. Gound, DDS, MS
3. Nedzinskienė E, Pečiulienė V, Aleksejūnienė J, Manelienė R, Drukteinis S, Jakaitienė A. Potential to induce dentinal cracks during retreatment procedures of teeth treated with "Russian red": An ex vivo study. Medicina (Kaunas). 2017;53(3):166-172. doi: 10.1016/j.medici.2017.05.005. Epub 2017 Jun 7. PMID: 28669594.
4. Gambrel MG, Hartwell GR, Moon PC, Cardon JW. The effect of endodontic solutions on resorcinol-formalin paste in teeth. J Endod. 2005 Jan;31(1):25-9. doi: 10.1097/01.don.0000147783.02453.82. PMID: 15614001.



