Apical control management with bioceramic sealer
06/07/2023
Marc Kaloustian
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
One of the most critical steps in endodontic treatment is the filling of the root canal system. The goal of 3D obturation is to fill the entire root canal system with a biocompatible material to prevent the entry of bacteria and other irritants that can cause infection or inflammation (Camilleri J. 2015).
Many techniques and material were proposed over the years to fill the root canal system (Pirani C et al. 2022).
Bioceramic sealers are nowadays used during endodontic treatment. Their gain in popularity among clinicians is related to their numerous properties such as biocompatibility, flowability and antimicrobial power on resistant bacteria such as Enterococcus Faecalis. It is a hydrophilic material that sets in the presence of moisture and releases calcium hydroxide. All these features make them a promising alternative to traditional sealers in endodontic treatment (Chybowski EA et al. 2018).
While the technique of bioceramic and single cone obturation seems easy to perform, extrusion of the material beyond the root canal can occur during injection, leading to inflammation, pain, and potential complications. In this article, we will explore a technique and strategy that can be used to deliver the sealer during a complex root canal treatment of a first mandibular lower left molar.

Fig. 1
A 45 year-old patient reported to the office with pain on the left lower mandibular molar. Upon clinical examination. No swelling or sinus tract were detected. The tooth was tender on percussion.
The preoperative mesio-lingualy angulated radiograph revealed an extensive lesion on mesial and distal roots. Underfilled obturation was also noticed with a probable ledge on one of the mesio-buccal canals and a separated instrument in the disco-lingual canal.
A diagnosis of acute periapical periodontitis was established and non surgical retreatment was decided.
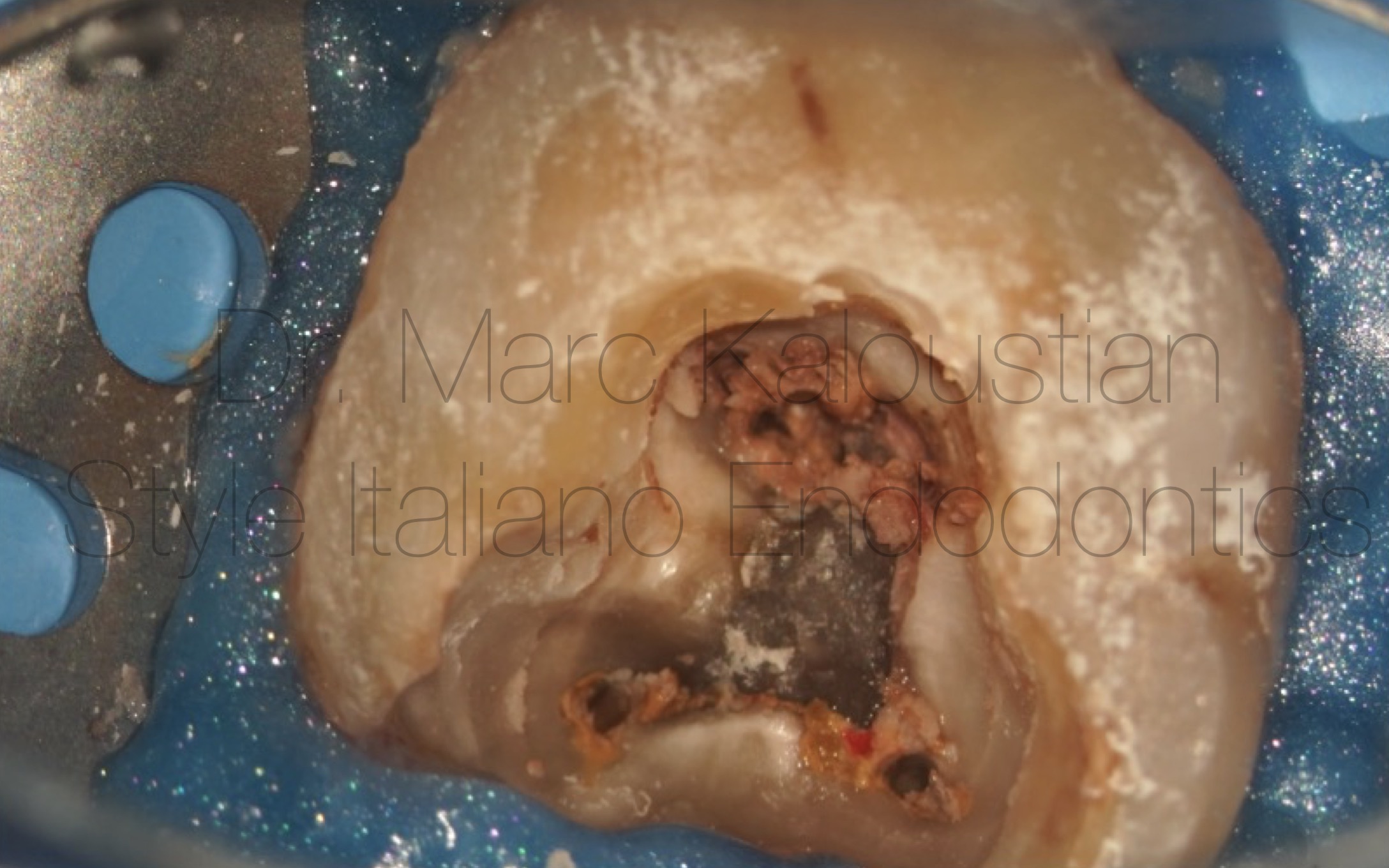
Fig. 2
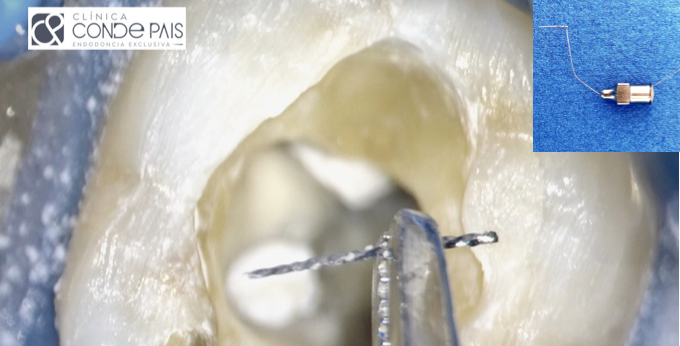
After the elimination of the core build -up, the first step of the retreatment procedure was to refine the access cavity using an ultrasonic tip. A direct access to all orifices was established.
15 mm length DR1 30/.10 file was used to initiate a 3 mm penetration in the gutta-percha in all 4 canals.
After placing a small drop of solvent in the reservoir created during the initial penetration, XP-endo® Rise Max wire instrument was used at 2500 rpm, and 1.5 N/cm torque to remove coronal and middle parts of the filling material.
After preserving a 08 K file using the EndoBender, the ledge was bypassed in the mesio-buccal and patency was established in the mesio-buccal, mesio-lingual and disto-buccal canals.
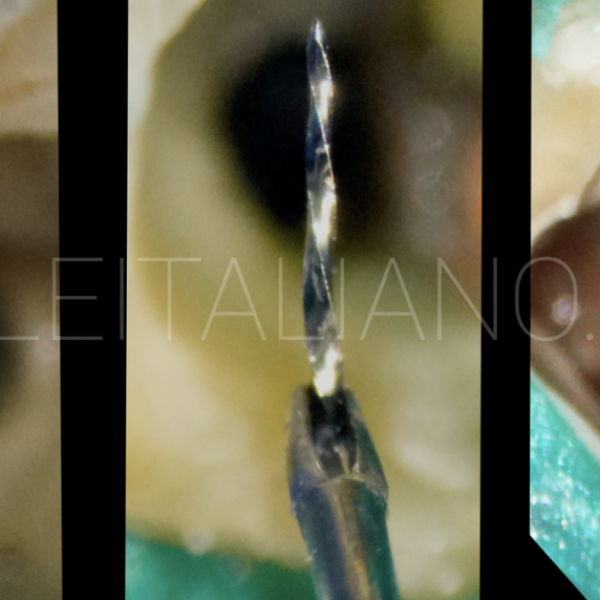
Instrument was removed from the mesio-lingual by vibration using a thin ultrasonic tip, patency was established and working length recorded using an apex locator.

Fig. 3
X-ray showing the removal of the filling material and the retrieval of the broken file and Working length registration of the disco-lingual canal.
After removal of the separated files pus drainage was successfully fulfilled.
Canals were shaped using the XP-endo® Rise Max wire instrument was used at 1000 rpm and 1.5 N/cm torque.
At the second session the rubber dam was placed and patency checked in all 4 canals.
The irrigation protocol was performed using the IrriFlex needle with 9 cc of NaOcl 6 % in each canal, followed by 1 cc of EDTA 17 % and finally distilled water.
NaOcl and EDTA were activated for 30 seconds each, using the XP Endo Finisher file at the WL -1 with an in and out motion.
Sterile medium paper points were used to check that all 4 canals were dry from pus.
Cone fit was done and tug back was established at the WL for all 4 canals.
Adequate Deppeler pluggers were chosen according to the orifice diameters.
After one last irrigation using distilled water, and since a bioceramic premixed sealer with single cone gutta-percha technique was planned, canals were lightly dried using a micro-aspirator and one paper cone in each canal
Obturation was done using a modified single cone technique proposed by Dr Riccardo Tonini, the cold molding technique (CMT). The sealer was injected at mid-root with light pressure, and an IrriFlex polymer needle was introduced passively till working length -2 mm, to diffuse it in the entire canal with minimal extrusion. Cones coated with sealer were introduced in the canals, cut at orifice level and packed with the selected pluggers. The details of this technique that minimize the extrusion to a small puff are described in the following link:

Fig. 4
The final Xray showing the obturation of the canals with equal puff extrusion in all of them. Patient was sent back to the referring dentist and follow-up appointment has been fixed after 6 months.
Conclusions
One of the key benefits of bioceramic sealers should be their ability to create a strong and tight seal in the root canal system. This is due to their hydrophilic nature, which allows them to adhere to the dentin walls and fill all the irregularities and accessory canals. This tight seal prevents bacteria and other irritants from entering the canal system, reducing the risk of reinfection and improving the long-term success of the treatment. (Sfeir et al. 2021) However, the perfect seal will depend on the technique of injection that should permit an obturation with minimal voids in the canal and minimal extrusion in the surrounding tissue (Mancino D et al. 2021). The recent development of a new technique (CMT) for injecting bioceramic sealers is promising concerning the accuracy and efficiency of the obturation process. Further clinical and in-vitro studies should be done to confirm these findings.
Bibliography
- Pirani C, Camilleri J. Effectiveness of root canal filling materials and techniques for treatment of apical periodontitis: A systematic review. Int Endod J. 2022 Jun 23. doi: 10.1111/iej.13787. Online ahead of print.
- Camilleri J. Sealers and warm gutta-percha obturation techniques. J Endod. 2015 Jan;41(1):72-8. doi: 10.1016/j.joen.2014.06.007.
- Chybowski EA, Glickman GN, Patel Y, Fleury A, Solomon E, He J. Clinical Outcome of Non-Surgical Root Canal Treatment Using a Single-cone Technique with Endosequence Bioceramic Sealer: A Retrospective Analysis. J Endod. 2018 Jun;44(6):941-945. doi: 10.1016/j.joen.2018.02.019.
- Mancino, D.; Kharouf, N.; Cabiddu, M.; Bukiet, F.; Haïkel, Y. Microscopic and chemical evaluation of the filling quality of five obturation techniques in oval-shaped root canals. Clin. Oral Investig. 2021, 25, 3757–3765. doi: 10.1007/s00784-020-03703-9.
- Sfeir G, Zogheib C, Patel S, Giraud T, Nagendrababu V, Bukiet F.Calcium Silicate-Based Root Canal Sealers: A Narrative Review and Clinical Perspectives. doi: 10.3390/ma14143965.