
AF F One Essential Kit in the treatment of a lower left first molar in a patient with periodontal disease
31/08/2023
Francesca Cerutti
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Multidisciplinary in dentistry is essential in order to treat correctly our patients. When for a clinician it is not possible to manage all of the branches of dentistry, the possibility to work in a team is the key to give the patient the best treatment.
When I see a patient for the first time, apart from the visit, inspection, palpation and necessary X-rays, a PSR (periodontal screening and recording) is done. In case of a PSR of 3 or 4, the patient undergoes a series of further investigation about his medical history and habits, a periodontal charting, the periodontal risk assessment, specific photographies and X-rays, then he sees the periodontologist.
In case of periodontal disease, the treatment is articulated and requires the collaboration of the patient in order to succeed, that is the reason why instruction and motivation of the patient have to be done properly.
The article will show the case of a patient treated for periodontal disease, with consequent endodontic treatment of two teeth.

Fig. 1
The baseline pictures show the presence of several questionable restorations, some hopeless teeth and the need for a full mouth periodontal approach.

Fig. 2
Baseline: detail of the lower arch. One missing restoration on tooth 4.5 is evident.
Amalgam restorations on teeth 3.6 and 4.6 need to be replaced.
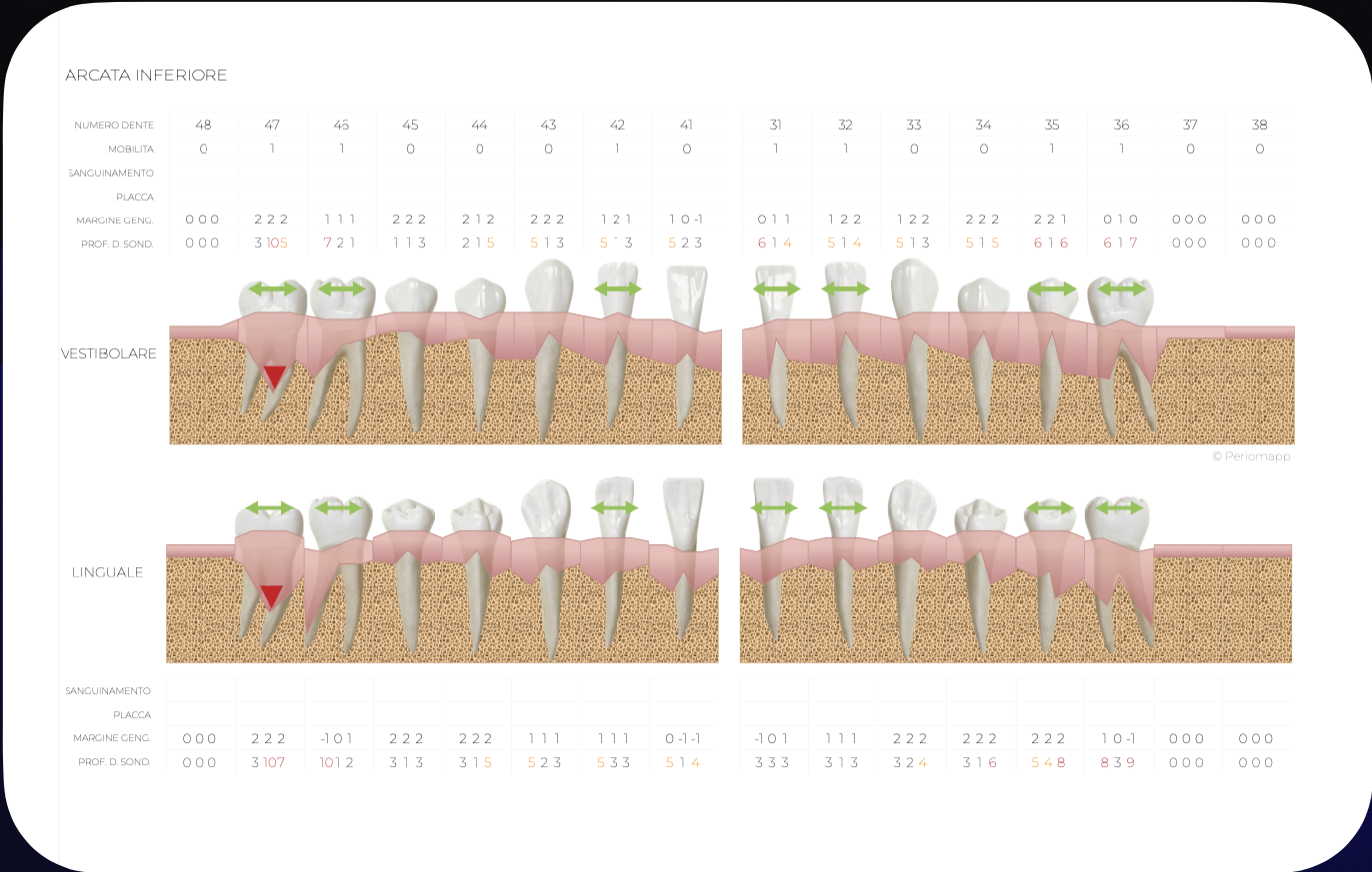
Fig. 3
Periodontal charting of the lower arch at the baseline

Fig. 4
The X-rays confirm the presence of bone resorption and the need for the patient to undergo periodontal treatment.
Tooth number 4.5 has been endodontically treated and restored immediately after the first visit because the patient was in pain.

Fig. 5
At the 4 months follow up the patient shows a good response to the therapy and a the capability to maintain a good level of oral hygiene.
Tooth 4.5 and 4.6 have been treated and restored.

Fig. 6
The hopeless 3.7 tooth has been extracted and the patient has started periodontal therapy. It is time to take care of the replacement of the amalgam restoration on tooth 3.6. The patient has been warned that probably an endodontic treatment will be necessary due to the proximity of the infiltrated amalgam restoration to the pulp chamber.
The pre operative X-ray shows a large horizontal resorption of the alveolar bone due to the periodontal disease and the recent extraction of the second molar.

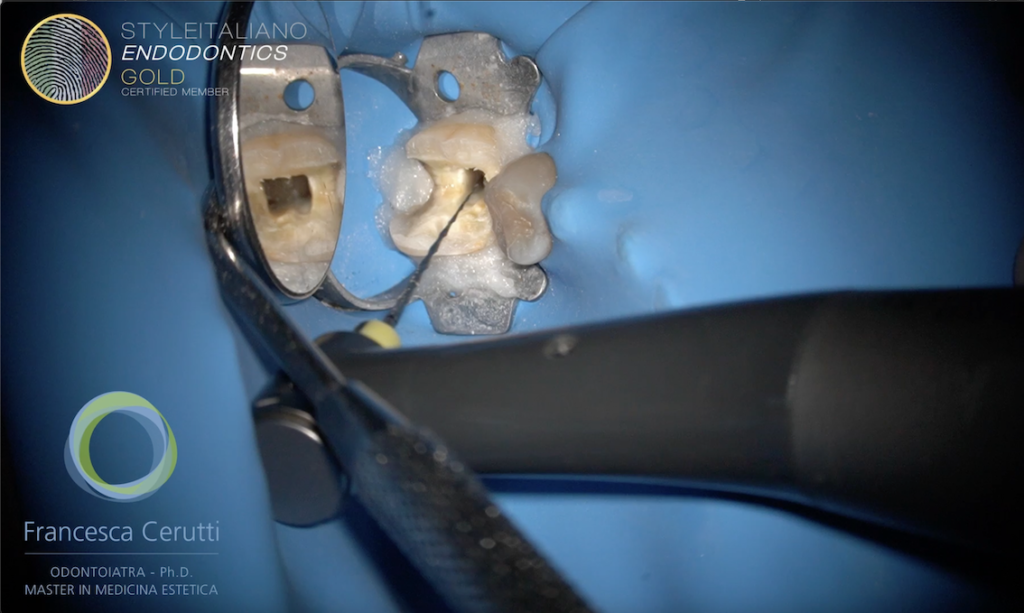
Fig. 7
Detail of the situation of tooth 3.6
After rubber dam isolation, the old restoration and the decay are removed. The access cavity is drawn and refined with ultrasonic tips, then the endodontic treatment is begun.
AF F one 13.03, 20.04 and 25.06 are used short to the WL in order to do some coronal pre flaring and to allow a smooth and centered path to the apex. The WL is then recorded with a manual #.10 K.file in the 4 root canals. Then, the sequence is repeated bringing the files at the working length.
The root canals are cleaned by NaOCl and EDTA, activated by means of an ultrasonic K-file, then they are filled with bioceramic sealer and single cone technique.
Post endo build up is done immediately in order to take the scan for the composite overlay in the same appointment.
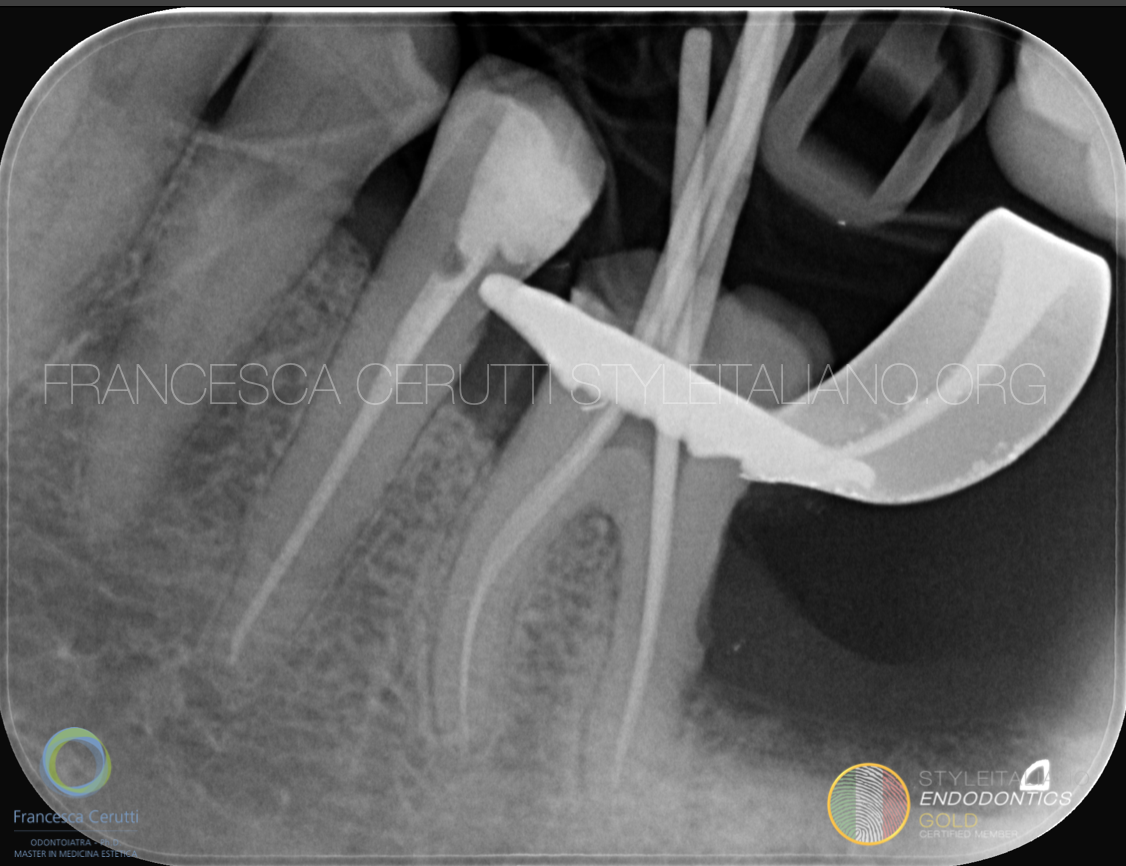
Fig. 8
The intra operative X-rays shows the fit of the selected gutta percha points

Fig. 9
The post operative X-ray shows the confluence of the mesial and of the distal canals.

Fig. 10
Post operative X-ray after the luting of the onlay.
Conclusions
A multidisciplinary approach is often necessary when treating our patients.
The AF F One Essential Kit by Style Italiano Endodontics is a powerful tool that can adapt to most of the clinical scenarios that we face in our practice.
Bibliography
Farman M, Joshi RI. Full-mouth treatment versus quadrant root surface debridement in the treatment of chronic periodontitis: a systematic review. Br Dent J. 2008 Nov 8;205(9):E18; discussion 496-7. doi: 10.1038/sj.bdj.2008.874. Epub 2008 Oct 3. PMID: 18833208.
Curtis DA, Lin GH, Rajendran Y, Gessese T, Suryadevara J, Kapila YL. Treatment planning considerations in the older adult with periodontal disease. Periodontol 2000. 2021 Oct;87(1):157-165. doi: 10.1111/prd.12383. PMID: 34463978.
Zitzmann NU, Krastl G, Hecker H, Walter C, Waltimo T, Weiger R. Strategic considerations in treatment planning: deciding when to treat, extract, or replace a questionable tooth. J Prosthet Dent. 2010 Aug;104(2):80-91. doi: 10.1016/S0022-3913(10)60096-0. PMID: 20654764.



