A C-shaped story: endodontic management and endocrown rehabilitation
17/04/2024
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
The C-shaped root canal configuration is an anatomical variation which is caused by the fusion of the mesial and distal roots either on the buccal or lingual root surface (1). The term ‘‘C-shaped canal’’ was firstly used by Cooke and Cox in 1979 (2). Numerous studies have reported that the incidence of C-shaped canals is higher in the mandibular second molars at a rate of 2.7- 44.5%, especially in Asian populations (3). The various irregularities present within C-shaped teeth make the cleaning, shaping and obturation of the root canal system a clinical challenge (3). The rehabilitation of C-shaped teeth with significant coronal tooth loss is also a demanding procedure. The use of intraradicular posts may increase the possibility of strip perforation due to the small amount of dentin between the internal canal system and the external root surface (3,4). In such cases other more conservative restorative approaches have been suggested, including but not limited to the endocrown restorations. The endocrown is a relatively new, conservative restoration which consists of the intraradicular post, the core, and the crown in one component. Endocrowns are retained macro-mechanically by the pulp chamber and micro-mechanically by bonding to the remaining tooth structure (5,6).
A 46 year old Greek female patient with a non-contributory medical history presented at the private dental office to restore her fractured left mandibular second molar. Clinically, the tooth #37 had an extensive carious lesion, was not tender to percussion, did not respond to the vitality tests and had normal periodontal probing depths. Post-cementation Radiograph Of The Endocrown Restoration. For the cementation of the endocrown restoration a dual-cured, universal, self-adhesive resin cement was used according to the instructions of the manufacturer.

Fig. 1
Preoperative Radiograph. The tooth #37 had one root with a radiolucency on the apical area. The diagnosis after clinical and radiographic examination was tooth necrosis and asymptomatic apical periodontitis.
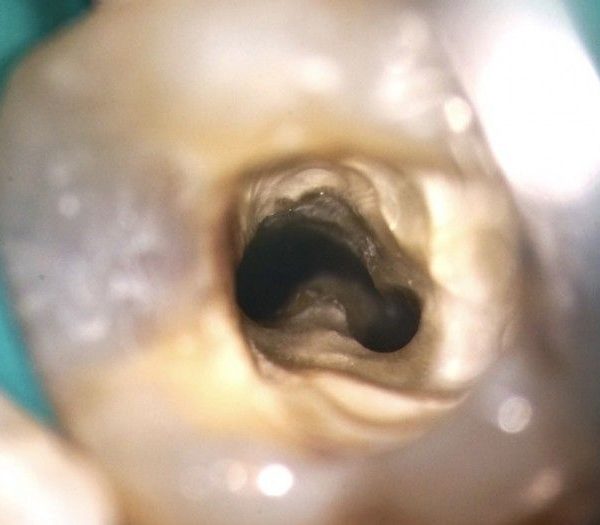
After the rubber isolation, low speed round carbide burs size 018 were used for the caries excavation following by size 010 for locating the orifices. In the final access cavity 4 canal orifices were detected; 3 canals were located distally and had an evident isthmus between them, while one canal mesially was separated by dentin from the others.
An orifice opener was used and then apical patency was achieved using C-Pilot 08, 10 stainless steel hand files. Working length determination was done with an electronic apex locator. Cleaning and shaping of the root canals were done with rotary instruments until size 25.04 under copious irrigation with 3% NaOCl. EDTA gel was used on the rotary files during the procedure.

Fig. 2
After checking the fit of gutta-percha master cones, the root canals were dried with paper points and obturation was carried out using an epoxy resin sealer and the continuous wave of condensation technique. A temporary filling was placed and a postoperative radiograph was taken. In the next appointment the tooth was restored with a direct composite overlay.

Fig. 3
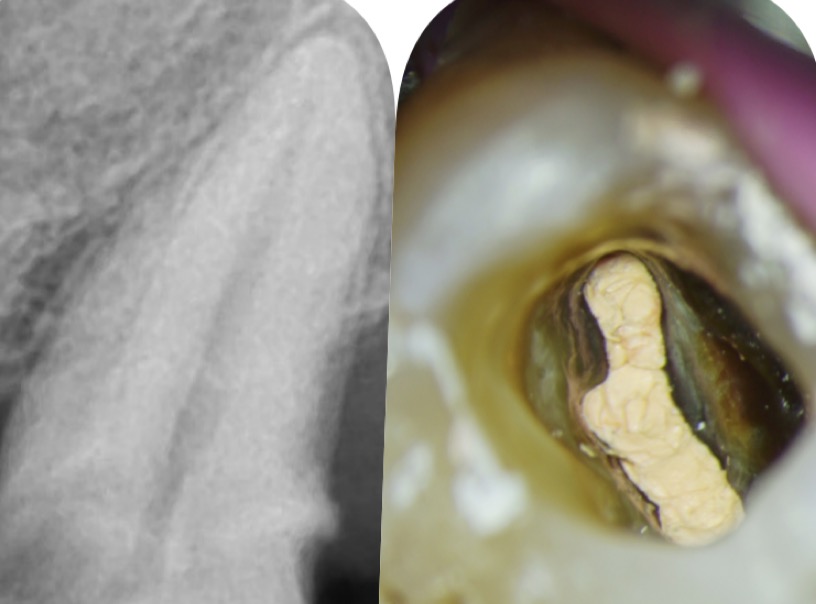
Recall Radiograph After 2,5 Years. The patient came to the dental office after 2,5 years due to a fraction in the distal area of the overlay. The recall radiograph revealed a healed periapical region, while the patient reported no symptoms from tooth #37. For the prosthetic rehabilitation of tooth #37 an endocrown restoration was chosen due to the deep pulp chamber, which would provide good retention for this type of restoration.

Fig. 4
Distal, occlusal, buccal, mesial, and lingual surfaces of the E.max endocrown restoration. Sandblasting of the restoration was done by the laboratory technician.

Fig. 5
Post-cementation Radiograph Of The Endocrown Restoration. For the cementation of the endocrown restoration a dual-cured, universal, self-adhesive resin cement was used according to the instructions of the manufacturer.

Fig. 6
Clinical Images Of The Endocrown Restoration After Cementation.

Fig. 7
Ourania Tsiouma
2016: Award of Excellence in the Physiology course from the Laboratory of Experimental Physiology, Medical School, National and Kapodistrian University of Athens.
2015-2019: <<Antonios Papadakis>> scholarship holder during her undergraduate studies.
2019: 1st "Ioannis Karkatzoulis" Prize for the best Oral Presentation in the 19th Pampeloponnesian Dental Congress.
2020: Graduated second with honours from the Dental School of the National and Kapodistian University of Athens, Greece.
2020–2022: Research Associate in the Department of Endodontics, Dental School, National and Kapodistrian University of Athens.
2023: Master in Clinical and Surgical Microendodontics, University of Turin, Italy.
Author of scientific articles published in national and international peer-reviewed journals.
Fellow Member of Style Italiano Endodontics.
Private practice focused on Endodontics and Restorative Dentistry in Athens, Greece.
Conclusions
The C-shaped root canal configuration has a high prevalence rate in mandibular second molars and numerous studies prove that this variation is linked to ethnic diversities. The debriment, obturation and rehabilitation of such cases still remains a clinical challenge. The endocrown restoration seems to be a good solution for the rehabilitation of C-shaped teeth because not only it requires minimal removal of sound tissue for its preparation design, but also can make use of the deep pulp chamber for its retention. However, further studies are needed to confirm that the endocrowns are more beneficial than other restorative approaches for the rehabilitation of C-shaped teeth.
Bibliography
- Manning SA. Root canal anatomy of mandibular second molars. Part II: C-shaped canals. Int Endod J. 1990;23:40–5.
- Cooke HG 3rd, Cox FL. C-shaped canal configurations in mandibular molars. J Am Dent Assoc. 1979 Nov;99(5):836-9. doi: 10.14219/jada.archive.1979.0402. PMID: 290680.
- Fernandes M, de Ataide I, Wagle R. C-shaped root canal configuration: A review of literature. J Conserv Dent. 2014 Jul;17(4):312-9. doi: 10.4103/0972-0707.136437. PMID: 25125841; PMCID: PMC4127687.
- Grocholewicz K, Lipski M, Weyna E. Endodontic and prosthetic treatment of teeth with C-shaped root canals. Ann Acad Med Stetin. 2009;55(3):55-9. PMID: 20698179.
- Sedrez-Porto JA, Rosa WL, da Silva AF, Münchow EA, Pereira-Cenci T. Endocrown restorations: A systematic review and meta-analysis. J Dent. 2016 Sep;52:8-14. doi: 10.1016/j.jdent.2016.07.005. Epub 2016 Jul 12. PMID: 27421989.
- Al-Dabbagh RA. Survival and success of endocrowns: A systematic review and meta-analysis. J Prosthet Dent. 2021 Mar;125(3):415.e1-415.e9. doi: 10.1016/j.prosdent.2020.01.011. Epub 2020 Mar 18. PMID: 32197821.