Root canal retreatment of upper left canine using iRoot Pro with integrated apex locator
21/03/2026
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
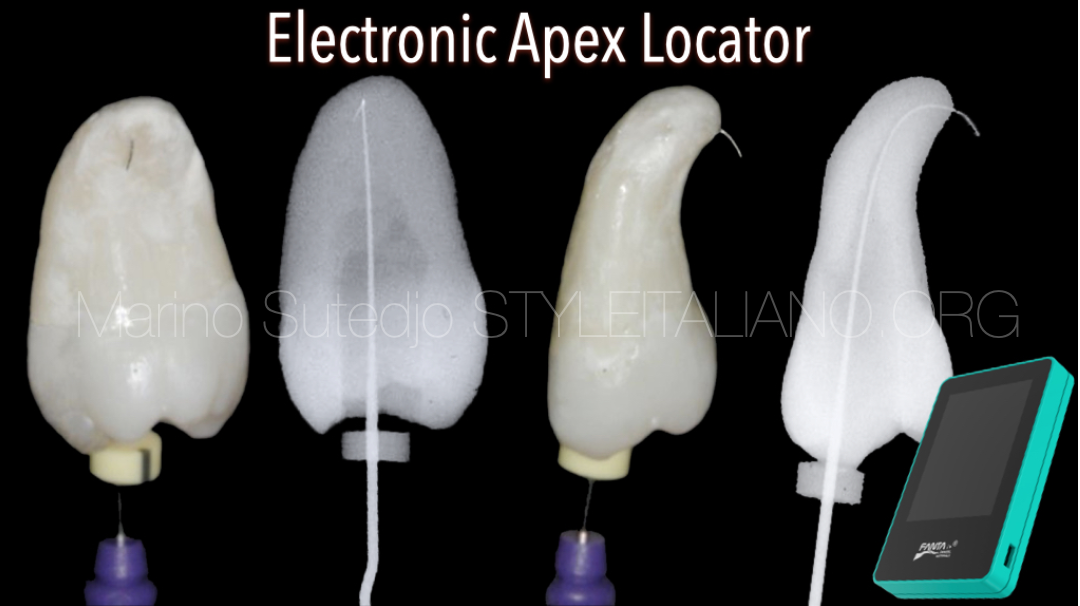
In root canal retreatment, we always focus on files only. While another important factor to consider is we should preserve apical construction during retreatment as possible
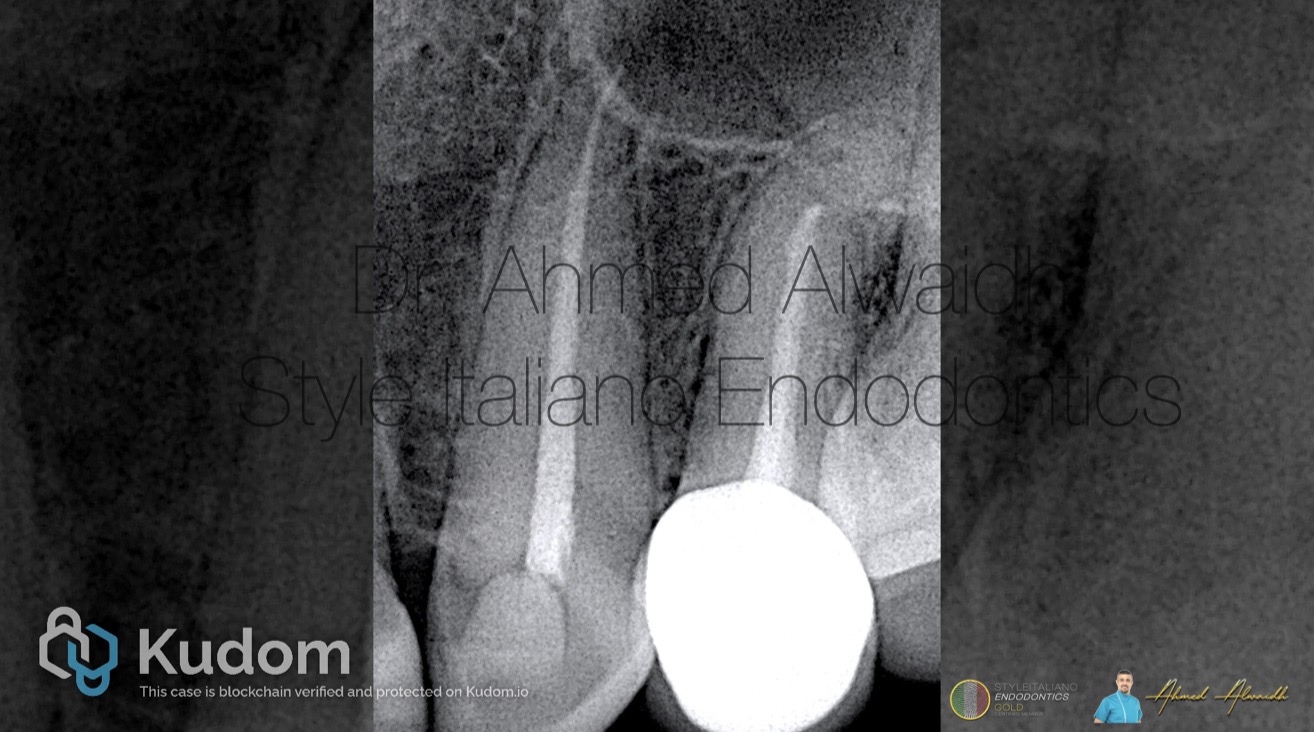
Fig. 1
A 40 years old female presented complaining of dull pain that increases during eating in her upper left canine. History of root canal treatment in UL3 around a year ago, and since then the symptoms started.
Clinically, UL3 was tender to percussion. IOPA revealed UL3 with existing root canal treatment, and peri apical changes.
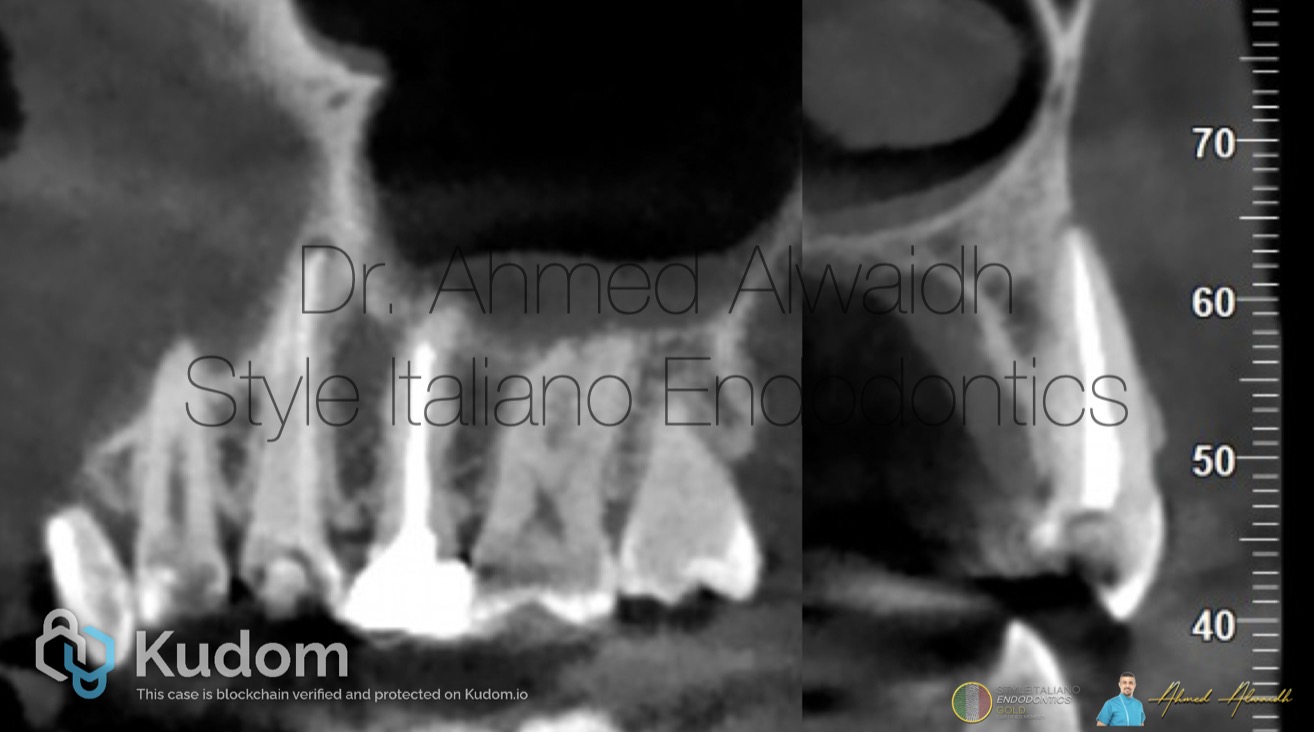
Fig. 2
Cone beam CT confirmed the presence of peri apical changes around the apex of UL3
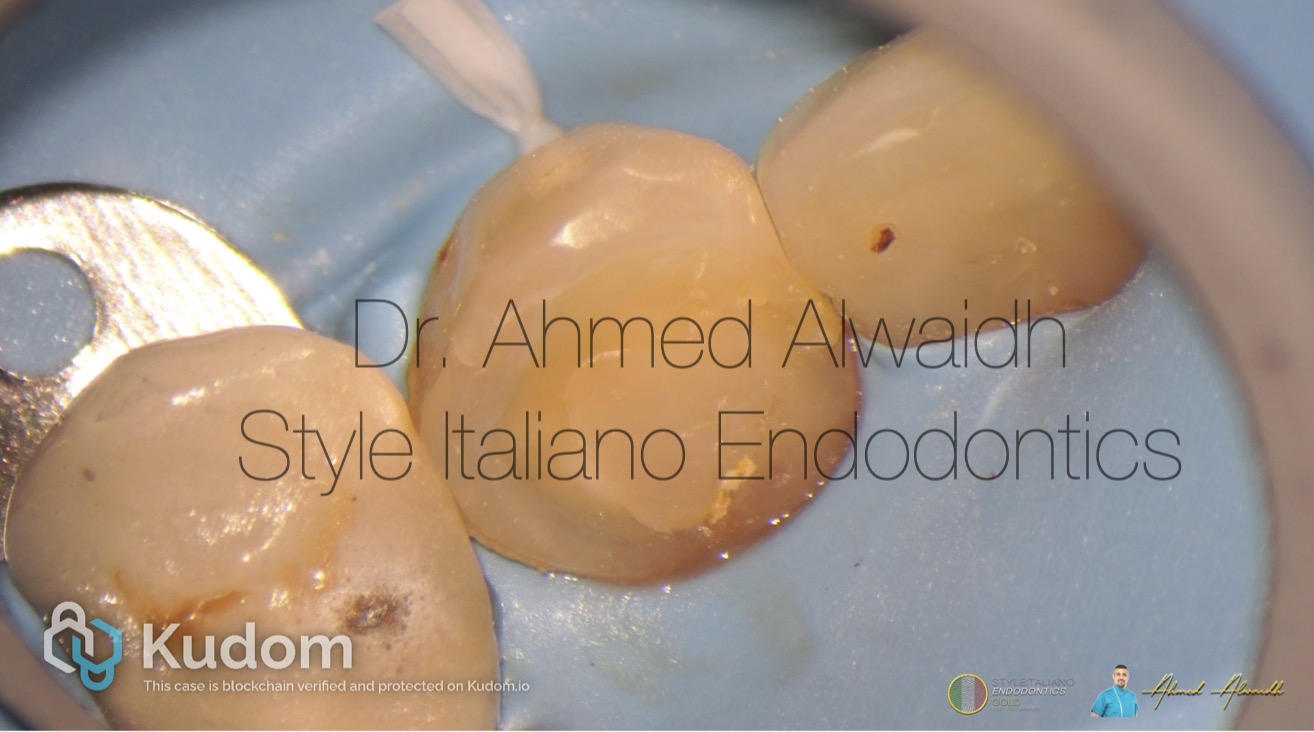
Fig. 3
Diagnosis: Previously treated UL3 with symptomatic apical periodontitis. Treatment plan: Root canal retreatment for UL3
Fig. 4
After buccal infiltration anaesthesia and rubber dam isolation, access been made to UL3
ReRCT to UL3 been made with Fanta F One #25/06 to full working length, using integrated apex locator option with iRoot Pro endomotor, which prevents the file to go beyond the working length. Then the canal been enlarged with F One #35/04 with copious irrigation with NaOCl 3% and PUI (US activation), and the canal been dressed with non setting calcium hydroxide for two weeks
Fig. 5
After two weeks, the patient presented with complete absence of symptoms. Irrigation with Naocl 3%, EDTA 17%, PUI.
Fig. 6
Hydraulic obturation with premixed BC cement.

Fig. 7
UL3 been restored with resin composite
Conclusions
Successful endodontic treatment depends heavily on the precise determination of the working length (WL). Accurate measurement of the tooth length is essential to carry out key stages of root canal therapy, including biomechanical preparation and obturation. Inadequate establishment of the correct WL can result in periradicular tissue injury and increase the likelihood of procedural complications (Chukka et al. 2020).
The most favorable outcome in root canal therapy is achieved when proper canal instrumentation is performed and the obturation is uniformly condensed up to the apical constriction. In contrast, the poorest prognosis occurs when both instrumentation and filling extend beyond the apical constriction (Ricucci & Langeland 1998)
Apical constriction, a natural narrowing at the junction between intra canal dentine and extra canal cementum. Using a combination electronic apex locator and endomotor can be an accurate asset to preserve the apical constriction during root canal preparation (Altenburger et al. 2009).
During primary root canal preparation, it is safer to preserve the apical constriction compared to endodontic retreatment. As in primary root canal preparation the working length can be determined before proceeding to apical third preparation. While in secondary root canal treatment, the canal is already filled and it is impossible to determine the canal working length before the treatment.
iRoot Pro endomotor by Fanta offers the advantage of combining both canal working length determination during root canal preparation, due to the integrated apex locator. This option offers a great advantage especially in root canal retreatment, to decrease the chance of apical constriction violation and destruction by large instruments.
Bibliography
- Altenburger M J, Cenik Y, Schirrmeister J F, Wrbas K T, Hellwig E (20090 Combination of apex locator and endodontic motor for continuous length control during root canal treatment. International endodontic journal 42(4), 368-374.
- Chukka R R, Bellam M D, Marukala N R, Dinapadu S, Konda N K, Nagilla J (2020) Efficiency of an Integrated Apex Locator in Determining Working Length in Various Irrigating Solutions: An: In Vivo: Study. Journal of Pharmacy and Bioallied Sciences 12(Suppl 1), S410-S414.
- Ricucci D, Langeland K (1998) Apical limit of root canal instrumentation and obturation, part 2. A histological study. International endodontic journal 31(6), 394-409.