

Dealing with hard canals, the easy way.
02/04/2024
Fellow
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
This article demonstrates the protocols followed on two teeth with unique anatomical features in a conservative, feasible, teachable and repeatable way.

Fig. 1
Upper second premolar (#15)
The patient was referred and presented with thermal hyperesthesia and reported discomfort upon masticatory exertion.
Radiographic evaluation of the maxillary left second premolar revealed distal carious involvement. The internal morphology suggested anatomical intricacies, with a provisional diagnosis indicating a potential supernumerary root.

Fig. 2
Multiple isolation was placed with clasps on the teeth #24 and #26.
The old restoration and the carious lesion were removed.
Under high microscopic magnification, a split of the mesial buccal root is observed with two orifices.
A coronal flaring of the canals was performed using a 25/0.4 rotary instrument at 500rpm.
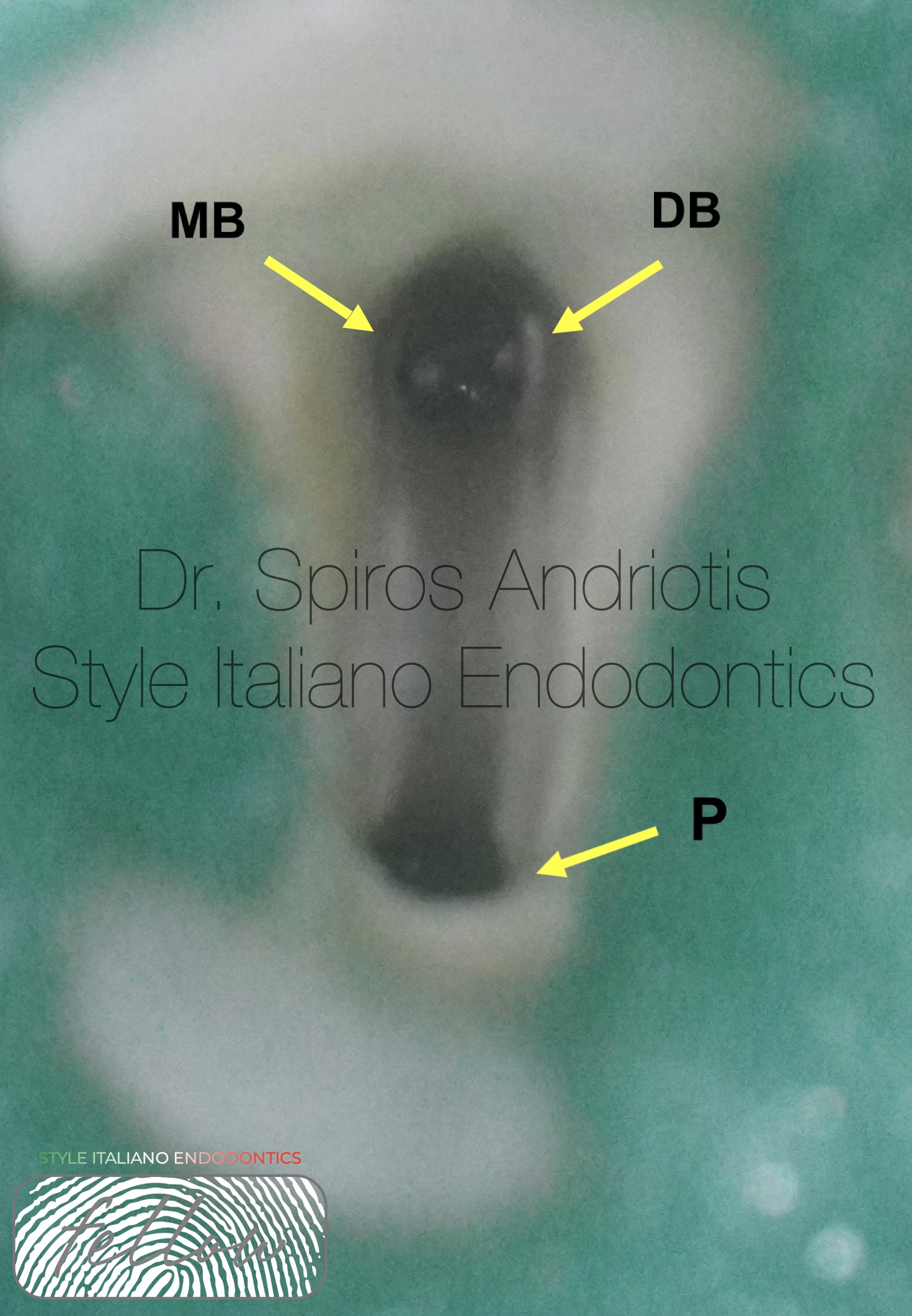
Fig. 3
The coronal flaring of the canals in such cases is vital, as it will remove coronal pulp tissue and create space for the NaOCl solution to dissolve tissue and enhance the lubricating effect of our first files attempting to reach the apical constriction of the root canal. A 5.25% solution of NaOCl delivered through an irriflex needle is .
Once we have rinsed the canals with a fair amount of NaOCl solution, the #8 K hand file reaches the working length of the canal even at the double curved DB root.
The working length estimation was carried out with the us of an electronic apex locator (Morita ZX mini).
The next step would be to create a reproducible glide path using a 15/0.3 NiTi rotary instrument with high flexibility. In this case, Plex V (Orodeca) was used.
At 300 rpm and torque 0.6 we performed gentle pecking motions in the canal, 2-3 mm each time, before cleaning the instrument and repeating the process to full working length. The files are put to motion after their placement in the canal. Every 5 seconds of rotary instrumentation the canal is washed with NaOCl 5.25% delivered by an irriflex needle until no more debris can be seen exiting the canal and the files are inspected.
Its important to note that in this step, the tactile sense is crucial as we must feel the resistance of the motion and avoid debris accumulation.
Creating a glide path, is the checkpoint of our shaping procedure as it will make the following process predictable. The final apical sizes of preparation were 25/0.4 for the buccal canals and 40/0.4 for the palatal.

Fig. 4
Finally, the shaping procedure was completed, and the gutta-percha cones were fitted in the canals. Sterilized scissors were used to adjust the cones and ensure an apical seal before the final irrigation protocol was carried out.
It is always important to mention that shaping is responsible for creating sufficient space in the canal systems. By doing that the irrigating solutions can disinfect its three-dimensional structure, especially in complex anatomies like the one being shown.
-Final irrigation protocol:
Needle used: Irriflex
In order:
- 1.NaOCl 5.25% solution is injected in the canals and activated for 30 seconds each with sonic activation (Eddy VDW)
- 2.EDTA 17% solution is injected and activated for 30 seconds at each canal (3 times) with sonic activation.
- 3.NaOCl 5.25% solution is injected in the canals and heated with a plugger at 180 degrees for 3 seconds in each canal (3 times)
- 4.A final, sonic activation of each canal was performed for 30 seconds
- 5.All canals were washed with saline and dried with sterile paper points.

Fig. 5
The obturation of each canal was performed with a single cone-warm vertical compaction technique and bioceramic sealer (Ceraseal). The patient was referred back for restorative and prosthetic rehabilitation of the tooth.

Fig. 6
The story of a unique upper second molar, presenting a long palatal root canal with a working length of 32mm and a severe apical curvature by the mesial root canal.
The workflow followed on this case didn’t differ from the previously mentioned case, with just one important detail. The mesial root canal was very thin and the apical hook too sharp for a hand instrument to scout.

Fig. 7
In this case the scouting and the working length determination was carried out with a 15/0.3 NiTi instrument, following the same guidelines with the three rooted premolar and the assistance of lubricant (RC prep). The endo motor was connected with an electronic apex locator. After several gentle peckings and multiple rinsing of the canals with NaOCl 5.25% delivered through an irriflex irrigation needle, the glide path file was able to overcome the sharp turn with ease and provided the space required for our 20/0.4 NiTi file to finish the shaping of the root canal in this case.

Fig. 8
Single Cone Warm obturation for all three canals combined with bioceramic sealer (Ceraseal).
A temporary restorative material was placed on top of a sterilized cotton pellet and the patient was referred back for indirect restoration.

Fig. 9
An exceptionally enthusiastic, motivated, and reliable individual. I spent a majority of my teenage years in a dental practice watching and assisting both of my parents. I have been a semi-professional football player from 2011 to 2017 as well as being an active member of the philharmonic society of Corfu, having performed in numerous concerts, playing the trumpet or the piano. All having helped me obtain important life and working skills which I have not only demonstrated during my studies and clinical practice, but continue to do so in everyday life. These include good communication skills, being able to work under pressure, as part of a team and take lead when needed.
During my high school and university years. I have spent my free time in Corfu assisting my parents when performing routine clinical examinations and treatments (restorative dentistry, endodontic therapy, prosthetic and implant dentistry). I have prepared the workplace between patients, helped with booking of appointments and assisted wherever I have been able to.
Conclusions
Modern instruments like NiTi heat-treated instruments, flexible irrigation needles and a set of safety rules have revolutionized root canal shaping even in cases with increased difficulty due to anatomical considerations. The modern way of root canal shaping is a more conservative philosophy, aiming to maintain as much sound tooth structure as possible, in comparison with older techniques which removed large amounts of peri-cervical dentin and that of the coronal third of the root canal, thus risking tooth fracture to achieve thorough shaping.
Bibliography
- Effectiveness of different final irrigant activation protocols on smear layer removal in curved canals
Gregory Caron, Khan Nham, Francois Bronnec, Pierre Machtou
2. Intracanal heating of sodium hypochlorite: Scanning electron microscope evaluation of root canal walls
Alfredo Iandolo, Massimo Amato, Alberto Dagna, Claudio Poggio, Dina Abdellatif, Vittorio Franco, Giuseppe Pantaleo
3. Maxillary Premolars with Three Root Canals: A Case Report
Reza Beyraghshamshir, Elnaz Karimian, Salehe Sekandarib



