Retreatment of badly decayed tooth with multiple mishaps
19/02/2026
Warning: Undefined variable $post in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Warning: Attempt to read property "ID" on null in /home/styleendo/htdocs/styleitaliano-endodontics.org/wp-content/plugins/oxygen/component-framework/components/classes/code-block.class.php(133) : eval()'d code on line 2
Root canal therapy is a high-precision discipline where success hinges on the delicate balance of biological principles and mechanical execution. However, even in the hands of the most meticulous clinician, endodontic mishaps—ranging from access cavities gone astray to the dreaded separated instrument—are an inherent risk of practice. Rather than viewing these complications as failures, modern endodontics treats them as challenges requiring prompt recognition and evidence-based management
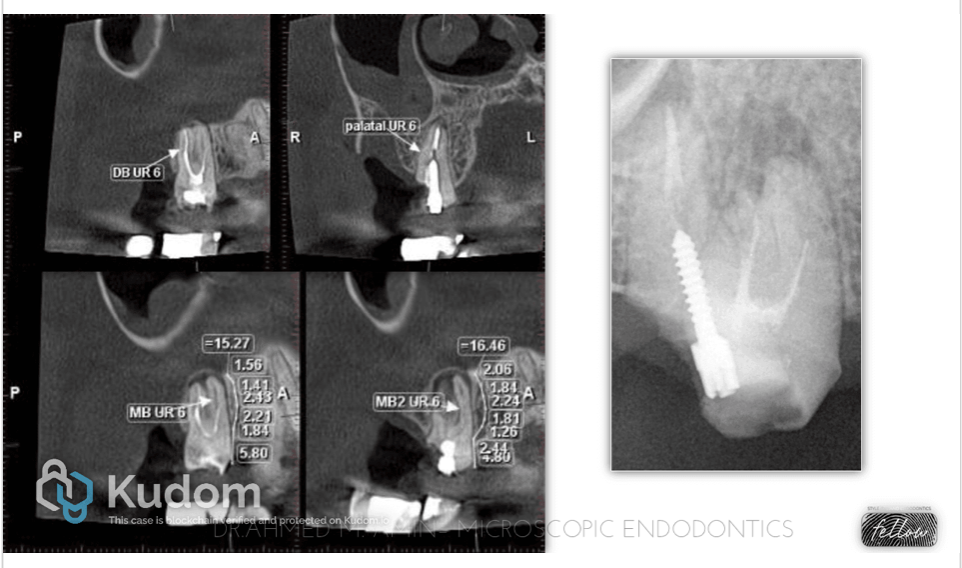
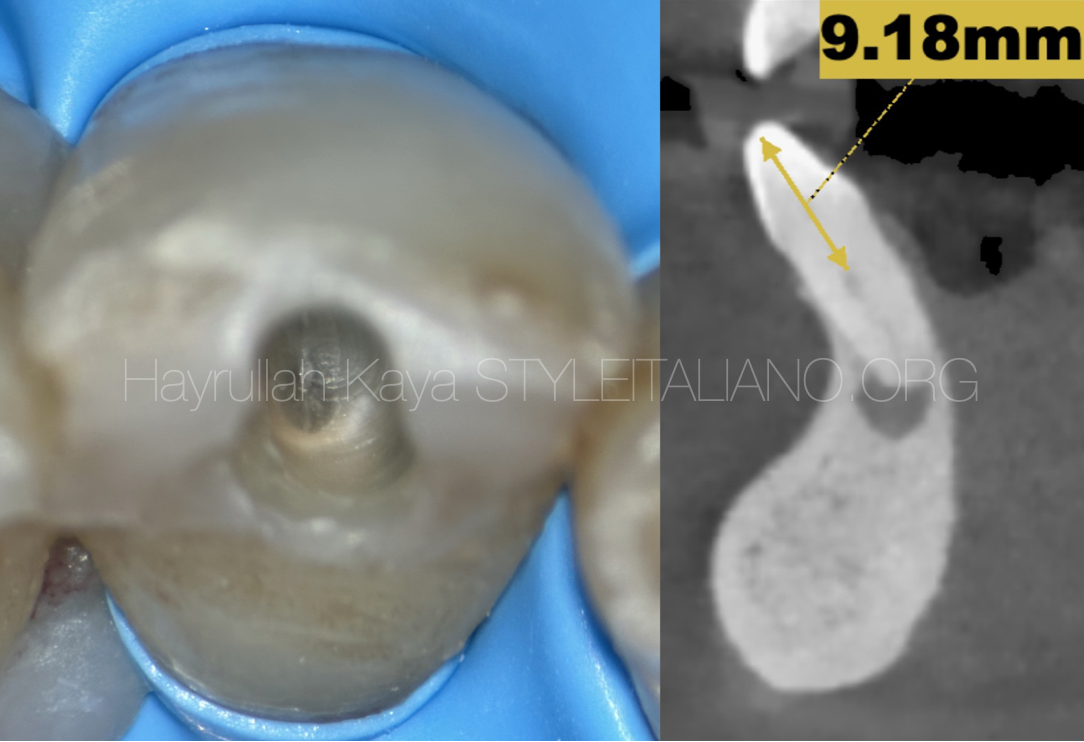
Fig. 1
A 32-year-old male patient presented to my clinic with a badly decayed prepared tooth no. 17, and he insisted on saving it rather than extraction & implant, which was an option.
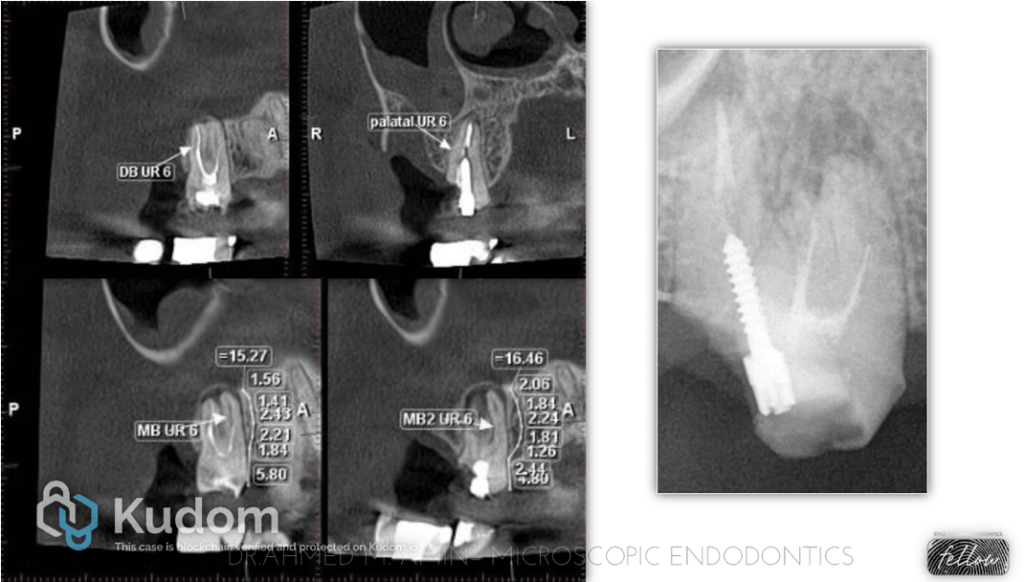
At first, I’d like to highlight the importance of CBCT for the assessment of such cases to be able to put the best treatment plan for the patient and also to determine the cost of all procedures.
We requested CBCT, and we found 3 roots with 4 canals.
-MB Root had 2 root canals with an isthmus connection and separate apical foramina.
-Missed Mb2 Canal
- A ledge & unextended root canal filling material of the MB root canal
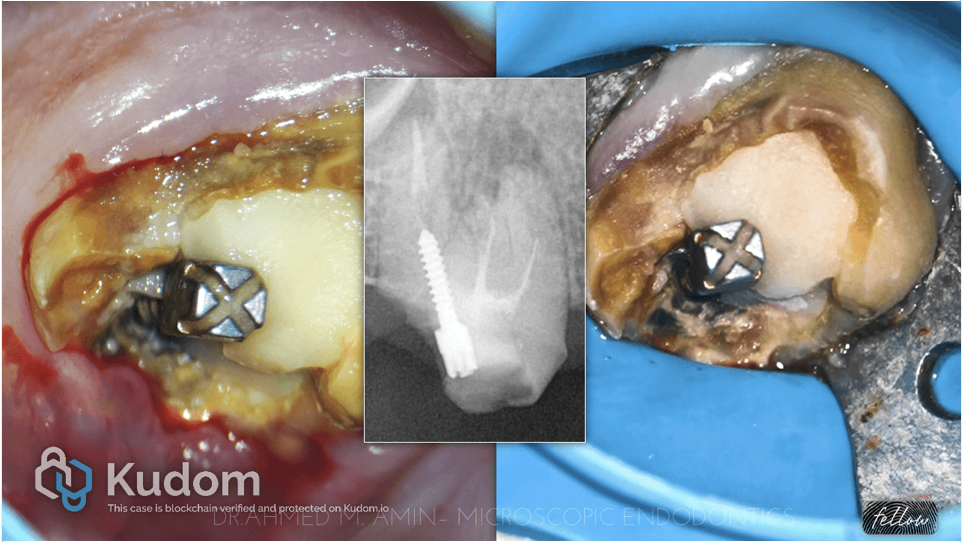
Fig. 2
We decided to do a gingivectomy on the distal side, remove all the caries, and remove the metal post to be able to assess the restorability of the tooth.
But first we need to isolate the tooth as In endodontics, the rubber dam is not just an "option"; it is the standard of care. It serves as the primary barrier between a successful clinical outcome and a potential failure due to contamination or accident.
The use of a rubber dam serves three critical roles during root canal therapy:
Asepsis: It prevents saliva (and the millions of bacteria it carries) from entering the pulp chamber, ensuring the root canal system remains as sterile as possible during instrumentation.
Patient Safety: It acts as a safety net, preventing the accidental aspiration or ingestion of small endodontic files, irrigation solutions (like sodium hypochlorite), and debris.
Clinical Efficiency: By retracting the cheeks, tongue, and lips, it provides a dry, high-contrast field of view, allowing you to focus entirely on the tooth's internal anatomy.

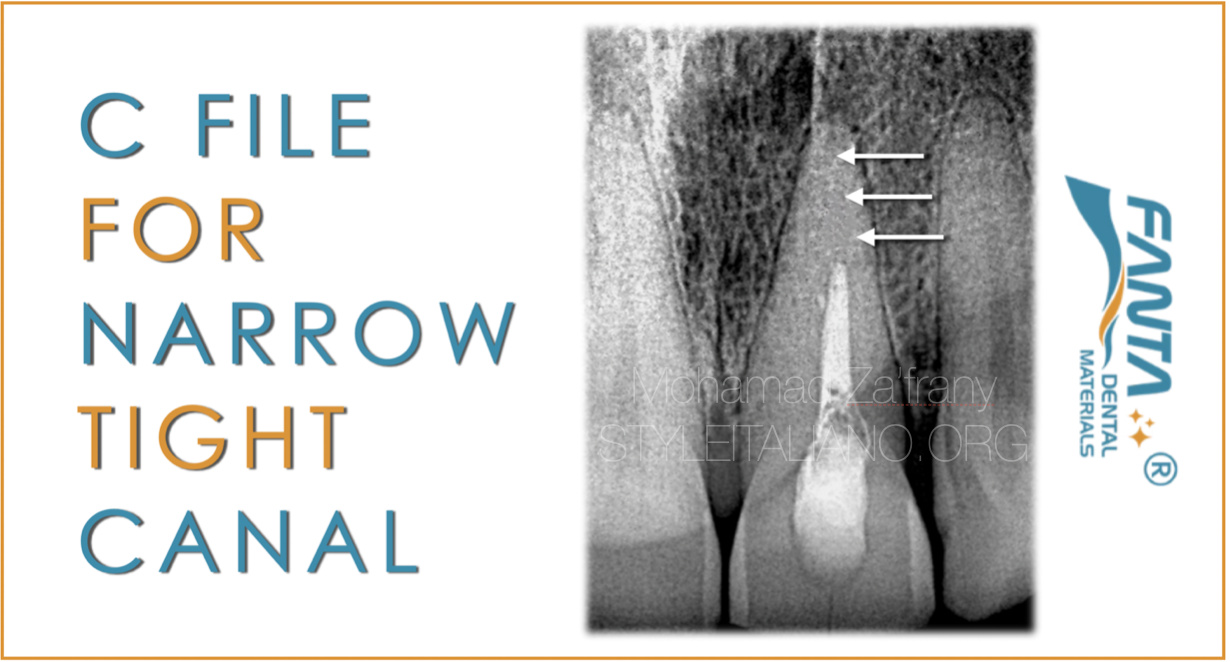
Fig. 3
1st & 2nd XRAY : Here, we removed the metal post using ultrasonics, and then we removed all the gutta-percha.
scout the canals and bypassd the ledge
Taking working length
Catching the MB2 canal
Preparation for all canals
3rd Xray : Intracanal medication to elevate the PH and to act as antibacterial
4th XRAY : Master cone fitting xray
5th XRAY : Obturation of Mesials & DB Canal with WVC + Bio C Sealer
Then we decided to obturate the palatal canal with MTA apical plug.
“X-ray of plugger fit 2 mm short of the working length”

Fig. 4
1st & 2nd Xray : First MTA Apical plug
3rd Xray : Obturation the rest of the canal with WVC + Bio C sealer
4th Xray : Final Obturation
5th Xray : Final Restoration

Fig. 5
MTA Apical PLUG, Clinically & Radiographically
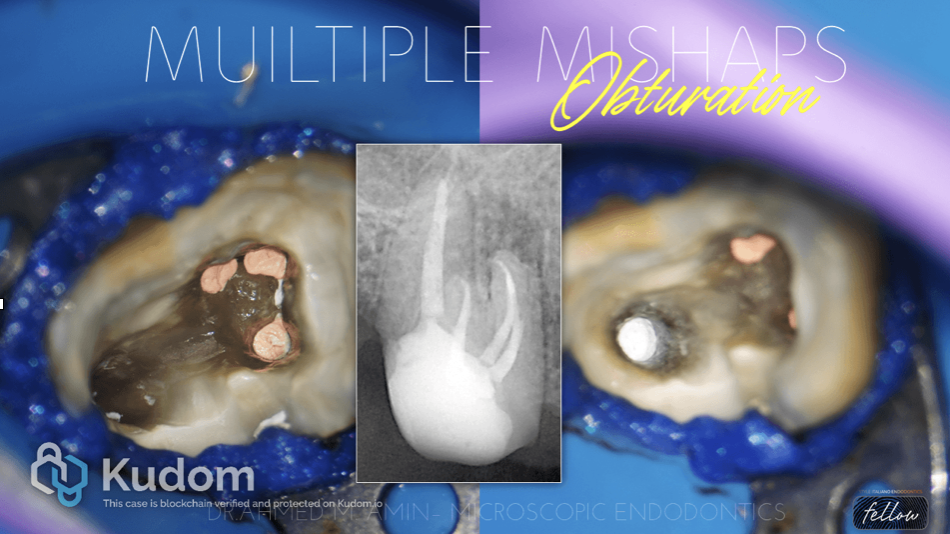
Fig. 6
Final Obturation View, Clinically & Radiographically

Fig. 7
Final restoration :
- Flowable Composite Over orifices as Intra-Orifice barrier
- Ever X As Dentin replacement
- Core build-up composite
Clinical View explains the Preparation for the crown with sufficient ferrule
Xray view : after Emax Crown Cementation
Video explains Steps of the whole Case

Fig. 8
About the author:
Ahmed M Amin
Endodontic Specialist at Kareem Elkabany Dental Clinic Since 2019
Microscopic Practionner Since 2020 at Amin Dental Clinic
Conclusions
An accurate assessment of the clinical and imaging diagnosis, comprehensive knowledge of the anatomy of the tooth and concerning the instruments being used, as well as consistently relying on the operating microscope can provide significant means in order to avoid a troublesome experience and perform the best endodontic treatment possible
Bibliography
1.Gluskin AH. Mishaps and serious complications in endodontic obturation. Endodontic topics. 2005 Nov;12(1):52-70.
2. Torabinejad M. Endodontic mishaps: etiology, prevention, and management. The Alpha omegan. 1990;83(4):42.
3.Clauder T, Shin S-J. Repair of perforations with MTA: clinical applications and mechanisms of action. Endodontic Topics 2006;15:32–55.
4.Management of ledge formation in root canal treatment . Aravind.N, Pradeep.S. International Journal of Current Advanced Research. 2017
5.CohenS, Burns RC. Pathways of the pulp. 8th ed. St Louis: Mosby, 2002
6.Jafarzadeh H, Abbott PV. Ledge formation: review of a great challenge in endodon- tics. J Endod 2007;33:1155–62.
7.Green KJ, Krell KV. Cilinical factors associated with ledged canals in maxillary and mandibular molars.Oral Surg Oral Med Oral Pathol 1990; 70: 490-7.
8.Fabio G. Gorni, DDS Andrei C. Ionescu, DDS, PhD, Federico Ambrogi, MSc, PhD Eugenio Brambilla, DDS Massimo M. Gagliani, MD, DDS Prognostic Factors and Primary Healing on Root Perforation Repaired with MTA: A 14-year Longitudinal Study DOI:https://doi.org/10.1016/j.joen.2022.06.005